
Abstract
As a result of the rapid worldwide increase in the older population, the prevalence of dementia and of its common precursor, mild cognitive impairment (MCI), is increasing (Alzheimer’s Disease International, 2015). In light of the extensive disability, need for support, and societal cost associated with dementia, together with the current lack of curative treatment, early detection strategies and interventions targeting maintenance of optimal functioning in everyday life are crucial. Although not everyone with MCI develops dementia (Roberts & Knopman, 2013), people with MCI are likely to experience disabling changes in everyday functioning (Jekel et al., 2015; Lindbergh, Dishman, & Miller, 2016). Early detection strategies targeting people with MCI include developing, validating, and incorporating relevant assessment methodologies that fit the needs of this group in order to determine the level of disability and monitor consequences in everyday functioning (Belchior, Korner-Bitensky, Holmes, & Robert, 2015; Lindbergh et al., 2016). Monitoring everyday technology (ET) use (e.g., microwave oven, cell phone) has shown to be one such promising assessment methodology (Jekel et al., 2015). In this study we used a prospective design to further explore ET use in relation to activity involvement.
Insight into the degree of functional impairment in people with MCI has broadened and deepened over the past 2 decades. Current criteria acknowledge that people with MCI attributable to Alzheimer’s disease perceive subtle difficulties (e.g., taking more time, being less efficient, making more mistakes) when performing complex everyday activities (Albert et al., 2011). A slow process of increasing challenges in and withdrawal from complex activities has been described (De Vriendt et al., 2012; Geda et al., 2011), including early difficulties in, for example, managing finances and medications and participating in outings and other leisure activities (Arrighi, Gélinas, McLaughlin, Buchanan, & Gauthier, 2013). A better understanding of the mechanisms of this decreasing activity involvement is important to be able to provide appropriate support.
In parallel with demographic changes, the contexts in which older adults pursue their lives and involve themselves in activities also have been changing. Many activities at home and in society now involve skilled management of ETs such as household appliances and information and communication technologies (ICTs; American Occupational Therapy Association [AOTA], 2014). In fact, much hope is placed on ICTs (e.g., smartphones, tablets) in the area of e-health as facilitators and problem solvers for the aging population (Cason, 2015; Koch, 2010). However, ICTs as well as other types of ETs, with their complexity and changeability have also been shown to present challenges for people with MCI or dementia relative to older adults without these disorders (Malinowsky, Kottorp, & Nygård, 2013; Patomella, Kottorp, & Nygård, 2013).
The environmental docility hypothesis assumes that the more complex the environment is, the greater the challenges are for people with reduced abilities to manage at home and in society (Lawton & Nahemow, 1973). Because ETs may add complexity to these contexts, it is important for health care professionals to explore and understand the association between the ability to use ETs and activity involvement, specifically, the frequency of performing instrumental activities of daily living (IADLs) and social tasks in both the home and the community. The association between ET use and activity involvement has been shown to grow stronger over time during cognitive decline (Hedman, Nygård, Malinowsky, Almkvist, & Kottorp, 2016) and is supported by cross-sectional findings (Nygård & Kottorp, 2014; Nygård, Pantzar, Uppgard, & Kottorp, 2012). The amount of ET used in a person’s daily activities seems to reflect additional clinically important aspects of cognitive impairment in the older population (Hedman, Nygård, Almkvist, & Kottorp, 2015).
In earlier 2-yr studies using the same sample of people with MCI as the current study, the amount of ET used decreased over time in parallel with decreasing activity involvement (Hedman et al., 2015), whereas the ability to use ETs showed a variable pattern of stability, fluctuation, or decrease over time (Hedman, Nygård, Almkvist, & Kottorp, 2013). Empirical longitudinal research over a more prolonged time period was needed to further explore how changing ability to use ETs is linked to the possibilities for people with MCI to remain active at home and in society while controlling for factors such as aging and diagnostic change. In addition to a decreasing ability to competently use ETs, is the number of ETs used important for continued activity involvement? Or is it to use a large share of the ETs that are accessible and relevant that is vital to staying active? Does the effect of using a large share of relevant ETs differ according to how influential ETs are in one’s life? Such potential interaction effects between ET use and activity involvement need to be explored.
Consistent with the environmental docility hypothesis (Lawton & Nahemow, 1973), in-depth knowledge of person–technology interaction mechanisms and their associations with changes in activity involvement among people with MCI over time may pave the way for more targeted and well-timed interventions that can minimize difficulties in ET use and enable sustainable activity involvement over time. Accordingly, in this study we investigated factors associated with decreasing activity involvement over a 5-yr period in people recently diagnosed with MCI. Special focus was placed on different aspects of ET use. The hypotheses tested are as follows:
Decreasing ability to use ETs, progression from MCI to dementia, and older age are associated with decreasing activity involvement over time.
Two aspects of the amount of ET use are important for continued activity involvement: (1) Use of a broad variety of ETs that are accessible and found relevant is linked to higher activity involvement, and (2) the larger the share of accessible and relevant ETs used, the higher the level of activity involvement. These two aspects of amount of ET use are likely to mutually reinforce each other.
Method
Participants
Participants in this prospective 5-yr study were 37 older adults with MCI who were diagnosed and recruited at a specialized outpatient memory clinic in Stockholm in 2008 and 2009. The inclusion criteria were as follows: fulfillment of MCI criteria according to Petersen (2004) and Winblad et al. (2004), that is, subjectively perceived and clinically verified cognitive decline, no dementia, and essentially intact basic activities of daily living and IADLs (which typically include use of ETs); age ≥55 yr; ability to take part in data collection in Swedish; no cognitive comorbidities; and no severe hearing or vision problems impossible to compensate for. Table 1 presents characteristics of the participants at inclusion, and Figure 1 gives an overview of data available and missing at the seven data collection time points. The regional ethics committee in Stockholm approved this research, and informed consent was obtained.
Participant Characteristics at Inclusion (N = 37)
Note. IQR = interquartile range; M = mean; MMSE = Mini-Mental State Examination (potential score range 0–30; higher scores indicate better cognitive status); SD = standard deviation. M and SD are presented for normally distributed data and median and IQR are presented for skewed data.
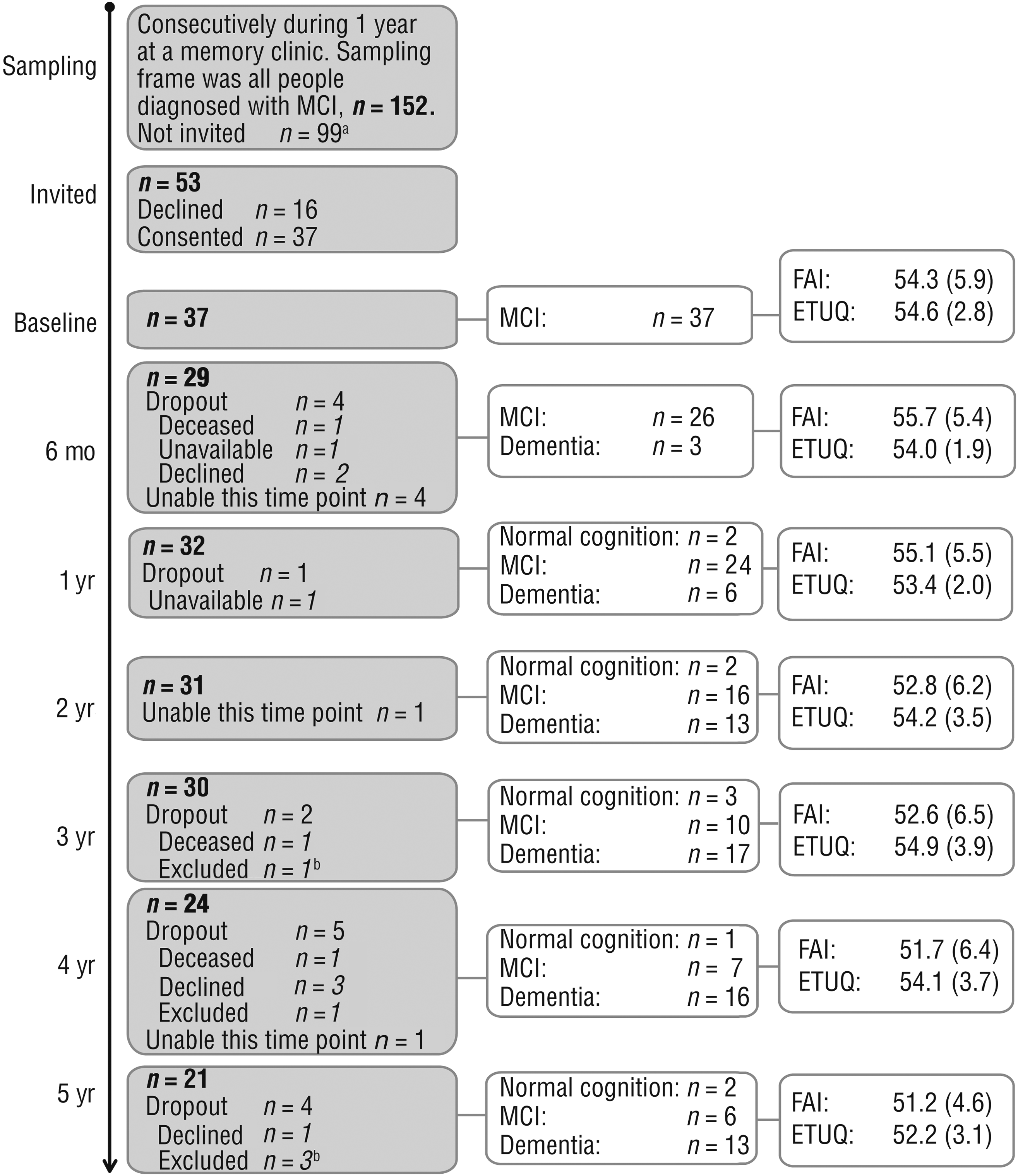
Flowchart of sampling, data collection, available and missing data, diagnostic information, and measures of activity involvement (FAI) and ability to use everyday technology (ETUQ).
Data Collection
Diagnostic information was collected from medical files at the memory clinic. All other data were gathered at each time point through semistructured face-to-face interviews with standardized instruments conducted by one of five research assistants or by the first author (Annicka Hedman). A total of 204 interviews were conducted, most often in the participants’ home. Participants who so wished could be accompanied by a significant other for support, but all scoring was based on the participants’ answers.
To detect potential changes in perceived activity involvement, we used the Frenchay Activities Index (FAI; Holbrook & Skilbeck, 1983). The 15 FAI items cover complex everyday activities such as preparing main meals, actively pursuing hobbies, and reading books. Frequency of activity involvement is rated using a 4-point scale, with higher scores indicating more frequent activity involvement. We used the Everyday Technology Use Questionnaire (ETUQ; Nygård et al., 2012) to capture alterations in perceived ability to use ETs and amount of ET available and currently used. The ETUQ includes 92 ET items that are commonly used by older adults within and outside the home. Ability to use available and relevant ETs is rated on a 6-point scale; higher scores indicate greater ability to use ETs. We used the Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975) to obtain a baseline description of cognitive function. The psychometric properties of these instruments when used with older adults with cognitive impairments have been found acceptable (Nygård & Kottorp, 2014; Nygård et al., 2012; Tombaugh & McIntyre, 1992).
Because no earlier longitudinal studies following people with MCI monitored involvement in complex and social activities as measured with the FAI, no sample size calculation could be performed when we decided to follow an already-identified sample of people newly diagnosed with MCI (n = 37) from an earlier cross-sectional study (Nygård et al., 2012). The findings from this longitudinal study should therefore be viewed as contributing to hypotheses regarding FAI changes over time in this group to support empirically based sample size calculations for future studies.
Data Analysis
Preparatory Data Analysis.
We applied a Rasch rating scale model (Bond & Fox, 2007) to transform the ordinal data from the FAI and ETUQ into linear person measures expressed in logits. This analytic procedure also provides in-depth psychometric information, which we used to ensure proper rating scale functioning of both instruments following standard procedures. The rationale and benefits of these procedures when analyzing ETUQ and FAI data have been described elsewhere (Hedman, Nygård, et al., 2016; Nygård et al., 2012).
Primary Data Analysis.
Linear mixed-effects models (Fitzmaurice, Laird, & Ware, 2004) were applied in the primary analysis, because such models can take into account all available data, including data from participants with missing values at one or several time points. The Bayesian information criterion was used when selecting the appropriate covariance structure in the models, suggesting best fit of a first-order autoregressive structure, which assumes gradually weaker correlations between residuals of the outcome variable over time. The significance level was set at .05.
The primary analysis was divided into two different models, both with activity involvement as the outcome, because our sample size allowed inclusion of a maximum of four explanatory variables at a time. To detect risk of multicollinearity, all explanatory variables were first tested together with follow-up time in bivariate models with activity involvement as the outcome and correlated at all time points using Spearman’s correlations. This procedure revealed significant time effects on activity involvement for each explanatory variable and consistently high (≥.80, p < .001) correlations between ability to use ETs and share of relevant ETs used, which therefore were analyzed in separate models.
Model 1 tested our first hypothesis and included the explanatory variables follow-up time, ability to use ETs, diagnosis (normal cognition, MCI, or dementia), and age. In Model 2, testing our second hypothesis, we aimed for a more in-depth exploration of the potential association of ET use and activity involvement. We therefore operationalized ET use as two additional explanatory variables, using the raw data from the ETUQ in two different ways: number of ETs used and share of relevant ETs used.
In the ETUQ, a relevant ET is defined as an ET that the person has access to and has used in the past, currently is using, or intends to use. In this study, the variable number of ETs used was obtained by counting the ET items each participant currently was using (range = 8–71). The variable share of relevant ETs used (range = 50%–100%) was calculated by dividing the number of ETs each participant currently was using by the total number of ETs the participant found relevant (range = 10–75), reflecting the proportion of ETs perceived as available and relevant that the participant actually used. Because we hypothesized that the effect of share of relevant ETs used might differ depending on number of ETs used, their interaction variable, share * number, was also included in Model 2.
Results for the variables share of relevant ETs used and number of ETs used were centered around their means to reduce the risk of multicollinearity in relation to their interaction variable; that is, the mean values of these variables for each time point were subtracted from the individual values (Fitzmaurice et al., 2004). In both models, all explanatory variables were specified as fixed effects and coded to reflect changes over time. The participants were specified as random effects.
Results
Ability to Use Everyday Technologies, Diagnostic Change, and Aging
The level of activity involvement decreased in the sample over the 5-yr course of the study (see Figure 1). A significant time effect on activity involvement was found, F = 4.555, p < .001. Mean activity involvement decreased significantly between baseline and Year 4 (−3.50 logits, p = .043) and between baseline and Year 5 (−5.09 logits, p = .002); comparisons of mean activity involvement between baseline and the other time points were nonsignificant. Ability to use ETs showed a significant time effect (F = 5.607, p < .01) and decreased over the 5-yr study (see Figure 1); this change was significant compared with baseline only at Year 5 (−2.84 logits, p = .002). In Model 1, decreasing ability to use ETs (b = 0.32, p = .007), progression from MCI to dementia (b = 2.20, p = .011), and older age (b = −0.42, p < .001) were all significantly related to decreasing activity involvement, indicating that decreasing ability to use ETs contributed significantly over time to decreasing activity involvement when controlling for the other variables. For data on diagnostic changes over time, see Figure 1.
Number and Share of Everyday Technologies Used
In Model 2 (Table 2), decreases in both number of ETs used (b = 0.66, p < .001) and share of relevant ETs used (b = 14.69, p = .04) were significantly related to decreasing activity involvement. However, the negative interaction variable (b = −0.46, p = .01) indicates that the larger the share of relevant ETs used by the person, the lower the influence of the number of ETs used on activity involvement. Similarly, the more ETs the person used, the lower the influence of the share of relevant ETs used on activity involvement.
Model 2 Results: Association Between Everyday Technologies Used and Level of Activity Involvement Over Time
Note. CI = confidence interval; ETs = everyday technologies; SE = standard error.
b estimates reflect the effect of a 1-unit increase of each explanatory variable on activity involvement when the other explanatory variables have the value 0.
Discussion
In Model 1, our hypothesis of associations between decreasing ability to use ETs, progression from MCI to dementia, and aging and decreasing activity involvement was verified. The ability to use ETs added significant information to the decreasing frequency in activity involvement of the participants beyond the associations with the parallel processes of time, diagnostic change, and aging. This result is in line with earlier, more descriptive findings of a stronger link between ability to use ETs and level of activity involvement over 4 yr in people with MCI (Hedman, Nygård, et al., 2016). Regarding Model 2, two outputs from ETUQ raw score data—number of ETs used and share of relevant ETs used—were also significantly related to activity involvement over time, which is new and potentially useful information for clinicians.
We also hypothesized that the influence of the number of ETs used and the share of relevant ETs used on participants’ level of activity involvement would reinforce each other. However, a positive interaction was not empirically supported; the estimate of the interaction variable of these two aspects of ET use demonstrated a significant negative relationship, suggesting that the higher the number of ETs used, the lower the influence of the share of relevant ETs used on activity involvement. A possible explanation is that if a person has incorporated and uses many ETs in daily life, the resulting variety of ETs used may compensate for nonuse of some ETs that are accessible and perceived as relevant to use. Some of the many ETs the person uses may have multiple purposes; for example, the cell phone may be used for functions also available on the computer, the television set, and the alarm clock, which may allow for continued activity involvement regardless of nonuse of the latter items. There are also ETs with parallel purposes, such as the microwave oven and the stove; potential problems with using a new microwave oven may be compensated for by instead using the available stove; this replacement strategy has been observed in people with MCI (Hedman, Lindqvist, & Nygård, 2016).
Correspondingly, the findings also indicate that the greater the share of relevant ETs used, the lower the influence of the number of ETs used on activity involvement. This result may reflect the situation of participants who use ETs they perceive as accessible and relevant, even if those ETs are very few, and whose established occupational patterns do not rely heavily on a broader variety of ET use, leaving them well prepared for continued activity involvement despite use of few ETs.
Thus, from the findings in this study, we conclude that using both a broader variety and a larger share of accessible and relevant ETs, regardless of how many, can promote a sustained level of activity involvement, as does higher ability to use ETs. Health care professionals must address the person–environment fit (Lawton & Nahemow, 1973) individually and, on the basis of the specific situation of each client, judge whether it is most appropriate to support use of a broad variety of ETs that are accessible and found relevant or to target specific ETs that are decisive for the client’s continued activity involvement.
Study Limitations and Future Research
The limited sample size and the considerable attrition suggest the necessity of caution in generalizing our findings. Furthermore, the small sample size did not allow us to run all explanatory variables in the same model, which would have been preferable. The use of self-report always involves some uncertainty in samples with cognitive impairments but was required to gain access to the insider perspective. Adding other modes of gathering information (e.g., observations) would have deepened the complexity of findings (Jekel et al., 2015). Additionally, the frequency-based measure (FAI) with a fixed set of activity items that we used to capture involvement in activities did not indicate whether specific activities were performed “as the result of choice, motivation, and meaning” (AOTA, 2014, p. S4). However, withdrawal from performing activities has been identified as an early phenomenon in cognitive decline (De Vriendt et al., 2012; Geda et al., 2011), and the FAI offers a validated way to capture this aspect. Future research should investigate whether minimizing difficulties in ET use through individualized interventions also supports sustained involvement in more complex everyday activities over time despite progressive cognitive decline.
Implications for Occupational Therapy Practice
In a cross-sectional study, both the ability to use ETs and the number of ETs found relevant by the participants showed the potential to predict the level of assistance needed in daily life in a sample of people with MCI or mild-stage Alzheimer’s disease (Ryd, Nygård, Malinowsky, Öhman, & Kottorp, 2016). These findings, together with those from this longitudinal study, underscore the importance of attending to clients’ ET use in occupational therapy evaluation and intervention, also supported in the Occupational Therapy Practice Framework: Domain and Process (AOTA, 2014).
To date, this area of occupational therapy practice has received little attention, although practitioners increasingly recognize ETs as an important topic well suited for their particular expertise and focus on clients’ activity involvement and well-being (Nygård & Rosenberg, 2016; Verdonck & Ryan, 2008). The results of this research have the following implications for occupational therapy:
This study and earlier research provide evidence-based arguments for more emphasis in occupational therapy education, praxis development, and research on evaluation and intervention related to ET use to support activity involvement among older people with early cognitive decline.
Increasing difficulty when using ETs is important to detect early in clients with MCI because such change is associated with decreasing activity involvement over time.
Attention should be paid to decreases both in the number of ETs used and in the share of accessible and relevant ETs used because such changes may indicate increased risk of withdrawal from activities in clients with MCI.
Footnotes
Acknowledgments
We thank the older adults who participated in this study, the occupational therapists who helped us collect data, and the funders who made the project possible: the Swedish Council for Health, Working Life and Welfare (FORTE); the Swedish Research Council (VR); the Strategic Research Programme in Care Sciences at the Karolinska Institutet; and the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and the Karolinska Institutet.