
Abstract
More than 44 million people around the world, 5 million of them in the United States, are living with Alzheimer’s disease (AD; Alzheimer’s Association, 2016; Van Cauwenberghe, Van Broeckhoven, & Sleegers, 2016). AD is a slowly progressive and irreversible neurodegenerative disorder that begins well before clinical symptoms emerge (Choe et al., 2016) and is the most common cause of dementia (Fiest et al., 2016). Dementia leads to the progressive decline of functions such as memory, orientation, understanding, judgment, calculation, learning, language, and thinking and, consequently, the performance of everyday activities. The impact of AD is enormous, affecting the individual and his or her family and friends at the personal, emotional, financial, and social levels. More than 15 million caregivers provide an estimated 18.1 billion hours of unpaid care each year for people with AD in the United States. Overall, AD and related major neurocognitive disorders (NCDs) cost the nation about $236 billion each year (Alzheimer’s Association, 2016).
Pharmacological treatments for AD have received much attention in the scientific literature and focus variously on symptoms and etiology. Although most side effects of these treatments are minor, they require close monitoring of the patient because of their neurotoxicity. Some evidence suggests that concurrent pharmacological and behavioral methods may maximize functional benefits for patients who have AD and reduce risk of death caused by medications (Buschert, Bokde, & Hampel, 2010; van Dyck, 2004).
Three broad perspectives on nonpharmacological intervention for AD have been described: (1) unmet needs, (2) learning and behavior, and (3) environmental vulnerability (reduced stress threshold). The unmet-needs perspective holds that behavioral symptoms of AD are an expression of an underlying need, such as the need for stimulation, pain reduction, or socialization (Schölzel-Dorenbos, Meeuwsen, & Olde Rikkert, 2010). The learning and behavior perspective considers behavioral symptoms to be the result of inadvertently reinforced behaviors, such as patients receiving attention when they scream (Bourgeois & Hickey, 2009). This article addresses the third perspective, environmental vulnerability and reduced stress threshold, which emphasizes a mismatch between a person’s environment and his or her ability to cope, such as when too much noise in the environment causes patients to overreact and become agitated (Cohen-Mansfield, 2001). The purpose of this systematic review (SR) was to appraise the effectiveness of environment-based interventions that address behavior, perception, and falls in people with AD and related major NCDs.
Method
This systematic review is one of three reviews of the AD literature relevant to occupational therapy conducted as part of the American Occupational Therapy Association's (AOTA's) Evidence-Based Practice (EBP) Project (Lieberman & Scheer, 2002; see also Piersol et al., 2017, and Smallfield & Heckenlaible, 2017, in this issue). The three questions were based on an earlier set of reviews covering 1994–2005 (Jensen & Padilla, 2011; Letts et al., 2011; Padilla, 2011a, 2011b) and were updated to reflect present clinical practice. AOTA staff, an advisory board of experts in the field, and review authors provided feedback on the development of the questions. Reviews were carried out through academic partnerships; the review team for this research question (the authors) consisted of two occupational therapy program faculty members. The review questions, inclusion criteria, and method were specified in advance. The following focused question framed this review: What is the evidence for the effect of environment-based interventions on behavior, perception, and falls in both the home and other settings (e.g., long-term care, assisted living) for people with AD and related major NCDs?
Search Strategy
Inclusion criteria for this review were as follows: Studies were published in English in peer-reviewed scientific journals between January 2006 and April 2014; intervention approaches were within the scope of practice of occupational therapy (AOTA, 2014); and study participants were diagnosed with AD or a related disorder. Although the database searches used the aforementioned dates as parameters, two articles published before 2006 that were not included in previous reviews were located by hand searching reference lists and were included because they provide valuable information to answer the question. Using the evidence hierarchy described by Sackett, Rosenberg, Muir Gray, Haynes, and Richardson (1996), Level IV (descriptive outcome studies such as single-subject and case series designs) and Level V (case reports, narrative literature reviews, and consensus statements) evidence were included only when Level I (systematic reviews, meta-analyses, and randomized controlled trials [RCTs]), Level II (two-group nonrandomized studies), or Level III (one-group, nonrandomized studies) evidence was not found. The review excluded qualitative studies, data from presentations, conference proceedings, non–peer-reviewed research reports, dissertations, and theses.
Search terms were developed by the methodology consultant to the AOTA EBP Project and AOTA staff in consultation with the review authors and the advisory group. Search terms were developed not only to capture pertinent articles but also to ensure that the terms relevant to the specific thesaurus of each database were included. See Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) for the electronic search terms and a sample strategy used for this question. A medical research librarian with experience in completing systematic review searches conducted all initial searches, and the review team followed up with additional searches.
Databases and sites searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews. Additionally, reference lists from articles included in systematic reviews were examined, and hand searches of selected journals ensured that all appropriate articles were included.
Study Selection, Data Extraction, and Risk-of-Bias Assessment
The methodology consultant to the EBP Project completed the first round, and the review authors the second round, of eliminating references on the basis of citations and abstracts. The review authors then retrieved full-text versions of potential articles and determined final inclusion in the review on the basis of relevance to the question, study quality, level of evidence, and inclusion and exclusion criteria. Disagreements were resolved through consensus. Each retained article was appraised and key information extracted to an evidence table that provides a summary of the methods and findings of the article. Supplemental Table 2 (online) summarizes the characteristics, including specific interventions assessed, of all included studies. AOTA staff and the EBP Project consultant reviewed the evidence table for quality control.
We assessed the risk of bias of individual studies using the methods described by Higgins, Altman, and Sterne (2011; see Supplemental Table 3, online). Our method for assessing the risk of bias of systematic reviews was based on the system developed by Shea et al. (2007; see Supplemental Table 4, online). Again, disagreements were resolved through consensus.
Data Synthesis
Given the heterogeneity of the included studies, we used a qualitative approach to data synthesis. Studies were examined for similarities across participants, settings, interventions, and outcomes and were grouped into themes. The strength of the evidence for each theme was appraised using an adaptation of the system proposed by the U.S. Preventive Services Task Force (2016):
Strong evidence indicates consistent results from at least 2 RCTs.
Moderate evidence includes 1 RCT or 2 or more studies with lower levels of evidence.
Limited evidence is based on few studies, flaws in available studies, or some inconsistency in the findings across individual studies.
Mixed evidence indicates that the findings were inconsistent across studies in a given category.
Insufficient evidence indicates that the number and quality of studies were too limited to make any clear classification.
Risk-of-bias appraisals were considered in designating strength of evidence.
Results
A total of 1,854 citations and abstracts were screened during the initial search, of which 154 were reviewed in full (Figure 1). Forty-two articles met the inclusion criteria (12 Level I SRs, 10 Level I RCTs, 4 Level II studies, and 16 Level III studies). Because most studies were not RCTs, there was a relatively high selection bias. Additionally, participants and study personnel in most studies were not blinded to the intervention, leading to a high risk of performance bias. Overall, the risk of bias in the included systematic reviews was low, with the exception of the risk of publication bias because most of the reviews did not include graphic aids or statistical tests. These risks may affect results.
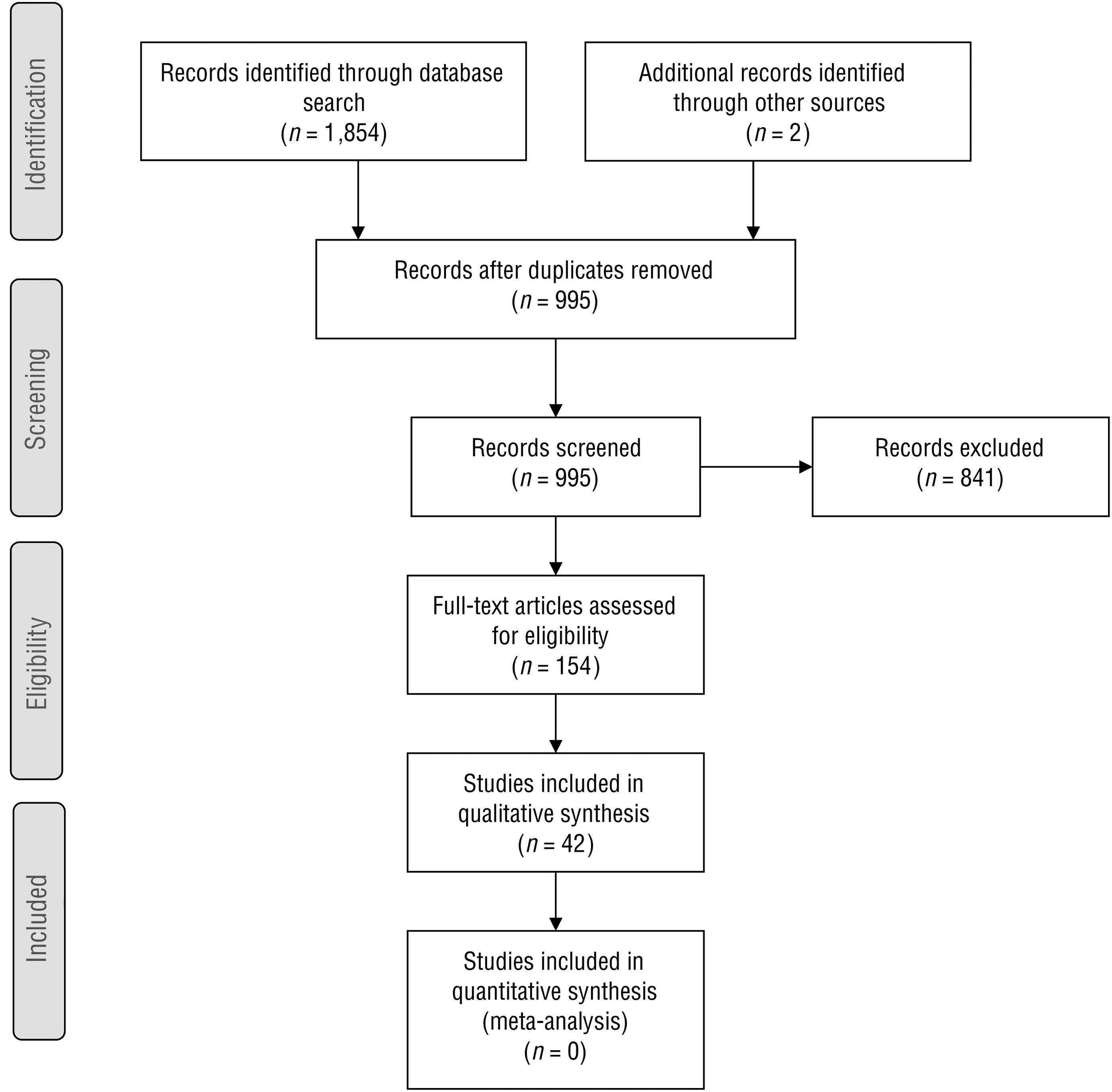
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of published literature search.
Interventions That Address Behavior
Thirty-six studies included in this systematic review evaluated the effect of environment-based interventions on behaviors of people with AD and related major NCDs. These interventions are organized into five themes: unimodal sensory interventions, multisensory interventions, functional task object availability, specialized environments, and person-centered interventions.
Unimodal Sensory Interventions.
Strong evidence was found for the effectiveness of music in improving behavior in people with AD and related major NCDs. Ambient music was modestly effective in reducing agitation, wandering, anxiety, irritability, aggression, and repetitive vocalizations (Padilla, 2011a, Level I SR) and more effective than listening to someone read in decreasing pacing (Hodgkinson, Koch, Nay, & Lewis, 2007, Level I SR). Active and passive music stimulation using preferred songs increased positive participation of residential day care center clients with moderately severe and severe AD (Lancioni et al., 2013, Level III). Evidence is mixed for the effect of mealtime music to improve behavior. Two studies found that quiet music played during mealtimes decreased agitation and improved engagement with eating (Chaudhury, Hung, & Badger, 2013, Level I SR; Gill & Englert, 2013, Level III), whereas 1 study found insufficient evidence for the same intervention (Liu, Cheon, & Thomas, 2014, Level I SR).
Moderate evidence supports noise reduction in institutional settings to decrease undesired behaviors (Fleming & Purandare, 2010, Level I SR; Mercado & Mercado, 2006, Level III). Additionally, regulating noise to a moderate level (i.e., not too quiet and not too loud) improved engagement with functional task objects (Cohen-Mansfield, Thein, Dakheel-Ali, & Marx, 2010, Level II).
The evidence for the effectiveness of aromatherapy in improving behavior is limited. No statistically significant effect was found for aromatherapy in reducing agitation, disruptive or resistive behaviors, or wandering (Burns et al., 2011, Level I; Fu, Moyle, & Cooke, 2013, Level I; Gray & Clair, 2002, Level III; Hodgkinson et al., 2007, Level I SR), and it was deemed only modestly effective in decreasing agitation in the short term (Padilla, 2011a, Level I SR).
Mixed evidence was found for the effectiveness of manipulating light to improve behaviors in people with AD and related major NCDs. Bright light therapy was not found to be more effective than standard light in decreasing agitation (Burns, Allen, Tomenson, Duignan, & Byrne, 2009, Level I) or improving attention and engagement with functional task objects (Cohen-Mansfield et al., 2010, Level II). Although 1 study reported that brighter-than-normal light decreased behavioral disturbance (Fleming & Purandare, 2010, Level I SR) and another that it somewhat reduced tension or anxiety and depression (Royer et al., 2012, Level I), another study found that bright ambient light in a dining room setting may have exacerbated behavior disturbances (Chaudhury et al., 2013, Level I SR). Finally, bright-light therapy coupled with melatonin did have some effect in decreasing agitation (Riemersma-van der Lek et al., 2008, Level I).
Only 1 study tested the effect of proprioceptive sensory input from an air mat. The authors found a short-term effect of reduced wandering (Hodgkinson et al., 2007, Level I SR).
Multisensory Interventions.
Strong evidence supports the effectiveness of multisensory environments (e.g., Snoezelen®) in decreasing agitation and anxiety (Fleming & Purandare, 2010, Level I SR; Kim, Yoo, Jung, Park, & Park, 2012, Level I SR; Marques, Cruz, Barbosa, Figueiredo, & Sousa, 2013, Level III; Maseda et al., 2014, Level I; Padilla, 2011a, Level I SR; Riley-Doucet & Dunn, 2013, Level III; Sánchez, Millán-Calenti, Lorenzo-López, & Maseda, 2013, Level I SR; Zimmerman et al., 2013, Level I SR). No effect or no long-term effect was found on reduction of wandering (Hodgkinson et al., 2007, Level I SR; Marques et al., 2013, Level III; Padilla, 2011a, Level I SR; Sánchez et al., 2013, Level I SR).
Functional Task Object Availability.
The evidence is mixed for the effectiveness of the availability of functional task objects in the environment in improving behavior. Positive effects included increased duration of engagement and improved behavior (Cohen-Mansfield et al., 2010, Level II); increased engagement and pleasure and decreased anxiety, specifically with Montessori-based programming (Padilla, 2011a, Level I SR); and decreased agitation (Cohen-Mansfield et al., 2012, Level I). However, occupational therapy interventions based on functional task activities were ineffective in improving depression and behavioral problems (Kim et al., 2012, Level I SR).
Specialized Environments.
Moderate evidence was found for the effectiveness of special care units (SCUs) or environments that were considered homelike. Homelike environments decreased aggressive behaviors but had a limited effect on agitation, pacing, and exit-seeking behaviors (Fleming & Purandare, 2010, Level I SR). Dining spaces that were smaller and equipped with a mealtime-orienting clock resulted in modest improvements in behavior and confusion (Chaudhury et al., 2013, Level I SR).
Overall, limited support is available that SCUs are superior to traditional nursing homes in decreasing problematic behaviors (Fleming & Purandare, 2010, Level I SR; Hodgkinson et al., 2007, Level I SR; Lai, Yeung, Mok, & Chi, 2009, Level I SR; Padilla, 2011a, Level I SR; Verbeek et al., 2014, Level II). However, 2 studies found benefits favoring SCUs over traditional nursing homes, showing a significant decrease in participant neuropsychiatric symptoms after 1 yr (Wolf-Ostermann, Worch, Fischer, Wulff, & Gräske, 2012, Level II) and increased time and engagement in common spaces (Morgan-Brown, Newton, & Ormerod, 2013, Level III). Environmental relocation from traditional nursing homes to SCUs or small household units resulted in no long-term change in behaviors (McFadden & Lunsman, 2010, Level III; Wilkes, Fleming, Wilkes, Cioffi, & Le Miere, 2005, Level III). One study (Wilkes et al., 2005, Level III) found a significant decrease in agitation immediately after relocation; however, there was no long-term effect.
The evidence is insufficient to support the use of wander gardens to improve behavior. Preliminary results showed a trend toward less agitation in a facility with unrestricted daytime wander garden access, with residents who visited the garden more frequently showing the largest effect (Detweiler, Murphy, Myers, & Kim, 2008, Level III).
Person-Centered Interventions.
Strong evidence is available for environment-based interventions that include a person-centered, individually tailored approach using a client’s preferences to produce improvements in behavior. A structured, multifactorial home-based program that included music therapy was found to significantly improve depression, night behaviors, anxiety, and disinhibition, although effects were lost at 3-mo follow-up (Carbone et al., 2013, Level III). A home-based program that included environmental modification showed improved engagement in people with AD and related disorders (Gitlin, Winter, Dennis, Hodgson, & Hauck, 2010, Level I). Behavior-based ergonomic therapy (e.g., availability of comforting or stimulating interventions) significantly decreased negative behaviors (Mowrey, Parikh, Bharwani, & Bharwani, 2013, Level III).
Multifactorial psychosocial interventions (e.g., music, aromatherapy, sensory environments) yielded a reduction in behavioral symptoms (O’Connor, Ames, Gardner, & King, 2009, Level I SR). Preferred music exposure was reported to improve behaviors in a Level I study (Padilla, 2011a, Level I SR). Namaste Care, which included environment-based interventions such as soft colors, soothing music, stuffed animals, and nature DVDs, showed a trend toward improved behaviors (Simard & Volicer, 2010, Level III). Finally, personalized bathing protocols that included person-centered environmental modifications were found to decrease agitation in a Level I study (Zimmerman et al., 2013, Level I SR). Only 1 study reported that occupational therapy interventions based on person-centered environmental modifications were not effective in improving depression and behaviors (Kim et al., 2012, Level I SR).
Interventions That Address Perception
Insufficient evidence supports the use of optical interventions (e.g., tints, prisms) to decrease neuropsychiatric symptoms (Letts et al., 2011, Level I SR). Likewise, the evidence is limited for the benefit of printed or graphic signage, personal items such as photographs, and other environmental cues (e.g., colors, numbers) to assist people with AD and related major NCDs in way finding (Fleming & Purandare, 2010, Level I SR; Hodgkinson et al., 2007, Level I SR; Letts et al., 2011, Level I SR; Padilla, 2011a, Level I SR). Preliminary evidence suggests that a motorized belt providing vibrotactile cues to enable way finding may be effective for people with mild dementia (Grierson, Zelek, Lam, Black, & Carnahan, 2011, Level III).
A moderate net benefit was found for the use of visual cues in the environment. Black grids on the floor in front of doors and other unobtrusive safety measures (e.g., camouflaged doors, silent electronic locks, horizontal grids of black tape in front of exits, mirrors or cloths in front of exit doors) reduced attempts at exiting (Fleming & Purandare, 2010, Level I SR; Hodgkinson et al., 2007, Level I SR; Letts et al., 2011, Level I SR; Padilla, 2011a, Level I SR). A moderate net benefit was also found for the use of environmental design to reduce disorientation and promote engagement in people with AD and related major NCDs. Making an important amenity such as the toilet easily visible, using L-shaped halls rather than straight corridors, and placing posters and murals on walls were found to reduce disorientation and promote engagement (Fleming & Purandare, 2010, Level I SR; Letts et al., 2011, Level I SR).
Interventions That Address Falls
The evidence is insufficient to fully support the use of wander gardens for fall reduction. Preliminary results suggest that unrestricted daytime access to a wander garden decreased falls and antidepressant and antipsychotic medication use for dementia unit residents, especially those who accessed the garden frequently (Detweiler, Murphy, Kim, Myers, & Ashai, 2009, Level II). Although insufficient evidence indicates that environmental modification alone reduces falls, preliminary results suggest a positive effect when used as part of a multifaceted approach together with exercise and staff-directed, disciplinary interventions (Jensen & Padilla, 2011, Level I SR).
Strong evidence supports the use of night monitoring systems (e.g., bed exit alarms, alarm systems, tracking devices, automatic nightlights, bracelets with teleassistance) to reduce the incidence of falls and unattended exits at home (Rowe et al., 2009, Level I; Tchalla et al., 2013, Level I RCT). However, monitoring systems (bed exit sensors, bathroom and bedroom exit monitors) did not lead to a significant reduction in falls or injuries in a nursing home (Holmes et al., 2007, Level II). In fact, a decrease in the number of falls and fallers in a residential facility appeared more directly related to the removal of bed exit and chair alarms (Bressler, Redfern, & Brown, 2011, Level III).
Limited evidence suggests that the use of music to reduce falls is effective. Six hours of daily music exposure (classical, relaxation, and generationally appropriate) in a facility dining room did not lead to any statistically significant differences in falls per resident (Gill & Englert, 2013, Level III). However, noise reduction and temporally appropriate (i.e., stimulating, upbeat music in the morning and calming, soothing music in the afternoon), controlled background music in a nursing facility reduced accidents and injuries (Mercado & Mercado, 2006, Level III).
Discussion
The literature reviewed on environment-based interventions for people with AD and related major NCDs provides current evidence to inform clinical and community-based occupational therapy practice, future research, and the education of occupational therapy practitioners. To improve behavior in people with AD and related major NCDs, strong evidence supports the use of ambient music other than at mealtimes; multisensory interventions; private, personalized rooms; varied ambiance in common rooms; and orienting room objects for clients who live in institutional settings. Moderate evidence indicates that noise regulation improves behavior. Moderate evidence also indicates that moving residents from a traditional nursing unit to an SCU or other environment has no negative long-term effects on behavior and that SCUs and other homelike environments are not superior to traditional nursing homes. The evidence is mixed for music played during mealtimes, bright light therapy, and the availability of functional items to improve behavior. Finally, limited or insufficient evidence exists for aromatherapy, proprioceptive input, and wander gardens to improve behavior in people with AD and related major NCDs.
In reviewing the literature related to environment-based interventions designed to influence perception in people with AD and related major NCDs, we found moderate evidence to support the use of specific environmental design elements, such as making amenities such as toilets easily visible to reduce disorientation and using L-shaped hallways and placing posters on walls to improve way finding. The use of unobtrusive visual barriers to reduce exiting attempts is also supported by moderate evidence, although the evidence specifically for the use of black stripes or grids in front of doors is mixed. Limited or insufficient evidence is available for the use of orienting signs, personal items, and vibrotactile devices to improve way finding and of optical devices, such as tints and prisms, to reduce the frequency of hallucinations.
We found strong evidence for night monitoring systems to reduce falls and prevent wandering for people with AD and related major NCDs living at home. However, limited evidence supports the use of fall monitoring devices in institutions to reduce falls. Limited or insufficient evidence was found for the use of wander gardens and ambient music to reduce falls.
Implications for Practice
Strong or moderate evidence supports the following environment-based interventions, and therefore we recommend that occupational therapy practitioners routinely use them in practice:
Person-centered, individually tailored, environment-based interventions for improving behavior during the duration of the intervention
Rooms designed for the intended purpose (i.e., privacy and personalization of resident bedrooms and familiar ambiance for living rooms and dining rooms) to improve behaviors
Ambient music for improving behavior at times other than mealtimes
Multisensory interventions (e.g., Snoezelen) for short-term behavior improvements
Environmental noise-level regulation to a moderate level for improving behavior
Concealed or painted doorknobs, murals on doors, or blinds or cloth barriers over doors to reduce exit attempts
Environmental design principles of murals and other art on walls, L-shaped corridors, and good visual access to important amenities (e.g., toilet) for reducing disorientation and promoting engagement
Monitoring devices for fall prevention used in the home.
Weak, conflicting, or insufficient evidence was found that the following interventions are effective for the listed outcome, and therefore we recommend that these interventions be used selectively on a case-by-case basis, heavily considering professional judgment and client preferences:
Aromatherapy to improve behavior
Ambient music to improve behavior during mealtimes
Bright light therapy to decrease behavioral disturbances
Proprioceptive sensory input (e.g., air mat therapy) to improve behavior
Functional task object availability in the environment to improve behavior
Wander gardens to improve behavior and reduce falls
Signage, personal memorabilia, and other environmental cues (e.g., colors, numbers) to facilitate way finding
Sensory devices worn by people with mild AD to facilitate way finding
Black tape grids or stripes on the floor in front of doors to reduce exit attempts
Tinted lenses, prisms, and other optical devices to improve perception
Monitoring devices to prevent falls in institutional settings.
At least fair evidence was found that ambient music was ineffective in reducing falls, and therefore we recommend that occupational therapy practitioners not use this intervention in practice if the desired outcome is fall reduction.
Implications for Education
Interventions supported by strong evidence should be part of entry-level professional education. Students must have a comprehensive understanding of AD and related major NCDs, including the client factors that can be restored or maintained (e.g., strength, endurance) and those for which compensation is appropriate (e.g., memory). The concept of environment as intervention should be emphasized, with a focus on environmental adaptations in various settings, especially the home. Students should be prepared with skills to function as members of interprofessional or multidisciplinary teams to effectively collaborate in the provision of the multifactorial interventions people with AD and related major NCDs need and to advocate for policies that promote best practices in care in the home.
Implications for Research
More studies, especially those that can provide higher levels of evidence such as RCTs and systematic reviews, are needed to strengthen the available evidence for interventions that are occupation based rather than based on isolated sensory inputs. Increased homogeneity of participants (e.g., grouping participants by stage or severity of AD) is needed to more specifically determine the effectiveness of interventions. As aging in place becomes a wider goal, more studies conducted in the home setting will be needed.
Limitations
Limitations found in many of the reviewed studies include small sample sizes, diagnostically heterogeneous populations (both in type and stage of dementia), and possible gender bias, with the majority of participants being women. Additionally, cointerventions and confounding variables were present in many of the studies. Most studies did not evaluate the long-term effects of interventions.
Conclusion
Occupational therapy has long recognized the dynamic interplay among clients, their occupations, and the environments in which these occupations occur (AOTA, 2014). When restoration of impairments is not feasible, as in the case of chronic and degenerative conditions such as AD, environmental intervention is a way to promote continued occupational engagement and positively influence client factors. This systematic review highlights the evidence supporting occupational therapy practitioners in providing environment-based interventions to address behavior, perception, and falls for people with AD and related major NCDs. Continued research is needed to increase the strength of the available evidence.
Supplemental Material
Supplementary material for Effectiveness of Environment-Based Interventions That Address Behavior, Perception, and Falls in People With Alzheimer’s Disease and Related Major Neurocognitive Disorders: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2017.027409.pdf for Effectiveness of Environment-Based Interventions That Address Behavior, Perception, and Falls in People With Alzheimer’s Disease and Related Major Neurocognitive Disorders: A Systematic Review by Lou Jensen and René Padilla in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman and Marian Arbesman of the AOTA EBP Project for their guidance and support throughout the entire process. Additionally, we thank Stacy Smallfield for her leadership. Elements of this study were presented at the 2015 AOTA Annual Conference & Expo in Nashville, TN.
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.