
Abstract
More than 15 million Americans provide unpaid care and services to people with Alzheimer’s disease (AD) and other major neurocognitive disorders (NCDs) that cause dementia (Friedman, Shih, Langa, & Hurd, 2015). For these caregivers, there is typically no advanced preparation and training. In fact, a 2014 Alzheimer’s Association telephone survey of 3,102 respondents revealed that the three primary reasons family members or other caregivers decided to provide care included wanting to keep the person with dementia (PWD) at home, living close to the PWD, and feeling obligated as a spouse or partner (Alzheimer’s Association, 2016). For the 60% of PWDs who live in the community, most have a caregiver living with them who assists with one or more activities of daily living (ADLs), such as bathing and dressing, as well as multiple instrumental activities of daily living (IADLs), such as managing finances and medications (Gaugler, Kane, & Kane, 2002).
In the United States, approximately two-thirds of caregivers are women, and about 1 in 3 caregivers is age 65 or older (Kasper, Freedman, & Spillman, 2014); “more than two-thirds of caregivers are non-Hispanic White, while 10% are African-American, 8% are Hispanic, and 5% are Asian” (Alzheimer’s Association, 2016, p. 475). Regardless of gender or race and ethnicity, 23% of caregivers consider themselves to be in the “sandwich generation,” with caregiver responsibilities for both a parent and children younger than age 18 (Alzheimer’s Association, 2016). Over the course of the disease, caregivers face unexpected challenges, including progressive decline in the PWD’s functional cognition and physical ability and the emergence of behavioral symptoms that are often distressing. As caregiver demands increase, families often face difficult decisions regarding the need for additional care in the home or the placement of the PWD in a residential care facility.
Although families report positive feelings about caregiving (Roth, Dilworth-Anderson, Huang, Gross, & Gitlin, 2015) and a sense of commitment and usefulness (Cheng, Mak, Lau, Ng, & Lam, 2016), caregiving decisions and actions have been found to cause long-term stress, anxiety, depression (Mausbach, Chattillion, Roepke, Patterson, & Grant, 2013; Välimäki, Martikainen, Hallikainen, Väätäinen, & Koivisto, 2015), burden (D’Onofrio et al., 2015; Papastavrou, Kalokerinou, Papacostas, Tsangari, & Sourtzi, 2007), and economic burden (Kelley, McGarry, Gorges, & Skinner, 2015). Difficulty learning and using the skills of caregiving can result in early institutionalization of the PWD (Vandepitte et al., 2016).
To address these multifactorial care challenges, nonpharmacological interventions aim to reduce caregiver burden and depression, improve caregiver knowledge and skills, delay nursing home placement for the PWD, and reduce the cost of formal care and services (Brodaty & Arasaratnam, 2012). Occupational therapy practitioners are skilled in the delivery of interventions that meet the varying and often multifaceted needs of caregivers (Edwards, 2015), resulting in improved caregiver self-efficacy (Vandepitte et al., 2016). Gitlin and Hodgson (2015) identified three intervention characteristics that were most effective in attaining positive outcomes for caregivers: (1) active involvement of the caregiver in the intervention process, (2) tailored and flexible content that meets evolving caregiver needs, and (3) dual focus on the caregiver and PWD.
To best serve the public, occupational therapy practitioners should have access to state-of-the-science, evidence-based approaches that are within the occupational therapy scope of practice to support caregivers in this essential and often complex role. Specifically, this review considers interventions for caregivers or caregiver–PWD dyads that vary in delivery format, dosage, and mode and target skill and wellness outcomes. The purpose of this systematic review was to evaluate and synthesize current evidence for effective educational and supportive caregiver interventions and strategies that facilitate caregiver ability to maintain participation in the caregiver role.
Method
This systematic review is one of three reviews of the AD and major NCD literature relevant to occupational therapy conducted under the auspices of the American Occupational Therapy Association (AOTA) Evidence-Based Practice (EBP) Project. The three questions were based on an earlier set of reviews that covered the literature from 1994 to 2005 (Jensen & Padilla, 2011; Letts et al., 2011; Padilla, 2011a, 2011b; Thinnes & Padilla, 2011) and were updated to reflect present clinical practice. AOTA staff, an advisory board of experts in the field, and review authors provided feedback on the development of the questions. The inclusion criteria and method were specified in advance. Reviews were carried out through academic partnerships, with the review team for this research question (the authors) consisting of one faculty member, three postprofessional occupational therapy doctoral students, and two entry-level occupational therapy students. The two other research questions (published in this issue) focused on the effectiveness of environment-based interventions (Jensen & Padilla, 2017) and the effectiveness of interventions designed to establish, modify, and maintain occupations (Smallfield & Heckenlaible, 2017). The following focused question framed this review: What is the evidence for the effect of educational and supportive strategies for caregivers of people with dementia on the ability to maintain participation in the caregiver role?
Search Strategy
Search terms were developed by the methodology consultant to the AOTA EBP Project and AOTA staff in consultation with the review authors and by the advisory group. Search terms were developed not only to capture pertinent articles but also to ensure that the terms relevant to the specific thesaurus of each database were included. The electronic search strategies can be found in Supplemental Appendix 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). A medical research librarian with experience in completing systematic review searches conducted all searches and confirmed and improved the search strategies.
Databases and sites searched included MEDLINE, PsycINFO, CINAHL, and OTseeker. In addition, consolidated information sources, such as the Cochrane Database of Systematic Reviews, were included in the search. These databases are peer-reviewed summaries of journal articles and provide a system for clinicians and scientists to conduct systematic reviews of selected clinical questions and topics. Moreover, reference lists from articles included in the systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
Inclusion and exclusion criteria are critical to the systematic review process because they provide the structure for the quality, type, and years of publication of the literature that is incorporated into a review. The review of the question was limited to peer-reviewed scientific literature published in English. The intervention approaches examined were within the scope of practice of occupational therapy. The literature included in the review was published between January 2006 and April 2014 and included study participants with AD and major NCD. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Using the evidence hierarchy described by Sackett, Rosenberg, Gray, Haynes, and Richardson (1996), studies in the review include Level I evidence (systematic reviews, meta-analyses, and randomized controlled trials [RCTs]), Level II evidence (two-group nonrandomized studies), and Level III evidence (one-group, nonrandomized, or cross-sectional studies).
Study Selection, Data Extraction, and Risk-of-Bias Assessment
The methodology consultant to the EBP Project completed the first step of eliminating references on the basis of citation and abstract. Review authors completed the next step of eliminating references on the basis of citations and abstracts. The full-text versions of potential articles were retrieved, and the review authors determined final inclusion in the review on the basis of relevance to the question, study quality, level of evidence, and inclusion and exclusion criteria. Disagreements were resolved through consensus. Each article included in the review was appraised and key information extracted to an evidence table that provides a summary of the methods and findings of the article. AOTA staff and the EBP Project consultant reviewed the evidence tables to ensure quality control.
The risk of bias of individual studies was assessed using the methods described by Higgins, Altman, and Sterne (2011). The method for assessing the risk of bias of systematic reviews was based on the measurement tool developed by Shea et al. (2007). Disagreements were resolved through consensus.
Data Synthesis
We used the narrative or qualitative synthesis approach described by Liberati et al. (2009) to examine the studies selected. This analysis process identified similarities across participants (family or informal caregivers and caregiver–care recipient dyads), interventions (e.g., format, dosage, method), and outcomes (e.g., self-efficacy, wellness, skill) and grouped the related findings into themes. The strength of the evidence for each theme was appraised using an adaption of the system proposed by the U.S. Preventive Services Task Force (2016). The strength categories are defined as follows:
Strong evidence indicates consistent results from multiple well-conducted studies, usually at least 2 RCTs.
Moderate evidence indicates 1 RCT or 2 or more studies with lower levels of evidence.
Limited evidence indicates few studies, flaws in the available studies, and some inconsistency in the findings across individual studies.
Mixed evidence indicates inconsistent findings across studies.
Insufficient evidence indicates that the number and quality of studies are too limited to make a clear classification.
Results
Of the 2,476 records that were screened, 288 underwent a full review, and 43 studies met the criteria and were included in the analysis. The flow diagram of studies is provided in Figure 1. The evidence represents 28 Level I studies, 7 Level II studies, and 8 Level III studies. Relevant study details are in Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). Results of the risk-of-bias assessments are in Supplemental Tables 2 and 3 (online). The qualitative analysis and synthesis resulted in five themes that describe types of approaches and interventions targeting the ability to perform and maintain participation in the role of caregiver: (1) case management interventions (2 studies); (2) group interventions (7 studies); (3) cognitive–behavioral interventions (3 studies); (4) single-component interventions (13 studies); and (5) multicomponent psychoeducational interventions (18 studies).
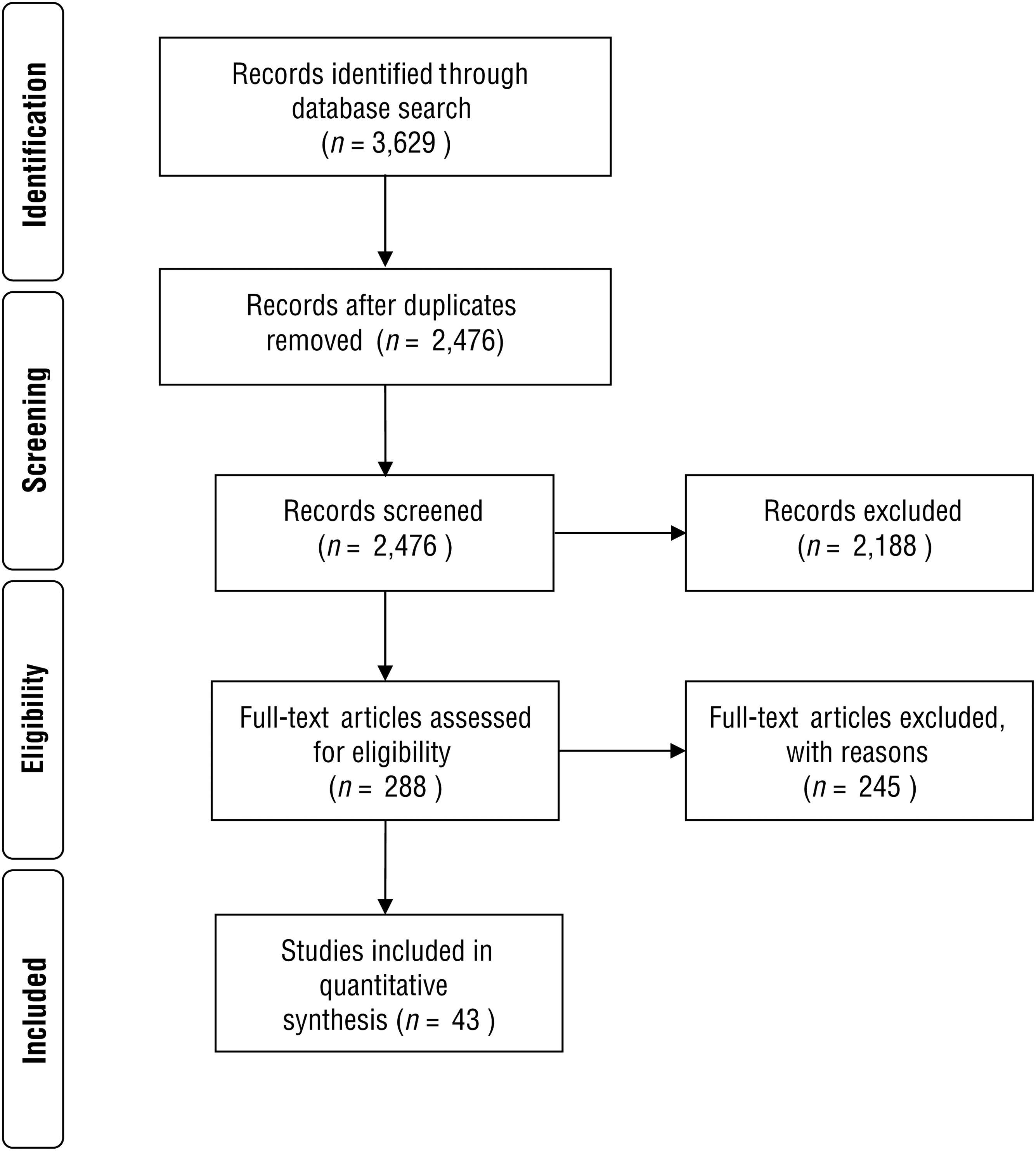
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of published literature search.
Case Management Interventions
Case management for PWDs has been shown to reduce burden and depression and improve well-being for caregivers (Challis, von Abendorff, Brown, Chesterman, & Hughes, 2002; Specht, Bossen, Hall, Zimmerman, & Russell, 2009). Two Level I studies examined the effectiveness of a nursing (Jansen et al., 2011) and an occupational therapy (Lam et al., 2010) case management intervention. There is strong evidence that case management does not affect caregiver burden, quality of life (QOL), or well-being (Jansen et al., 2011; Lam et al., 2010). However, caregivers receiving occupational therapy case management, which included training and cognitive stimulation for the PWD, used significantly more respite services (in-home support and day care services) than those receiving a single visit (Lam et al., 2010).
Group Interventions
The group format allows caregivers to share experiences and learn from one another. The types of groups in this review included in-person support groups and Internet-based support groups. Strong evidence from 2 Level I studies (Chien et al., 2011; Wang & Chien, 2011), 1 Level II study (Wang, Chien, & Lee, 2012), and 1 Level III study (Bartfay & Bartfay, 2013) indicates that in-person caregiver support groups led by professionals improved caregiver well-being and reduced depression, burden, and stress. Additionally, 1 Level III study (Gaugler et al., 2011) found that support groups increased caregiver preparation and confidence in managing memory loss. In contrast, Joling et al. (2012) found that group family meetings did not reduce caregiver burden or improve QOL compared with usual care in a Level I study.
In addition, 1 Level II study (Marziali & Garcia, 2011) provides insufficient evidence for the effect of Internet-based (asynchronous and synchronous) support groups. Both types of Internet group improved caregiver self-efficacy; the asynchronous chat group reduced caregiver distress in managing IADLs, and the synchronous video group improved caregiver mental health and lowered distress in managing deteriorating cognitive function in the PWD.
Cognitive–Behavioral Interventions
Cognitive–behavioral interventions build on the belief that there is an association between thinking and personal behavior or action. Strong evidence from 1 Level I systematic review and meta-analysis (Vernooij-Dassen, Draskovic, McCleery, & Downs, 2011), 1 Level I study (Gallagher-Thompson et al., 2010), and 1 Level III study (Glueckauf et al., 2012) indicates that cognitive–behavioral interventions focused on cognitive reframing and skills training reduced caregiver depression, anxiety, and stress. Gallagher-Thompson et al. (2010) found greater caregiver satisfaction with an intervention that included practitioner interaction compared with a self-directed educational program. Glueckauf et al. (2012) found that mode of delivery (telephone or in person) did not make a difference in caregiver outcomes.
Single-Component Interventions
Single-component interventions use a distinct method or mode of delivery. Nine types of intervention were identified: (1) communication skills training, (2) communication skills training in combination with memory aids, (3) mindfulness-based training, (4) stress management delivered by Internet and telephone, (5) exercise program, (6) nighttime monitoring system, (7) assistive device training, (8) adapted leisure program, and (9) coaching delivered by email and telephone. Table 1 describes the level and strength of evidence available for each of these interventions.
Synthesis of Evidence for Single-Component Interventions
Memory aids included memory books, photos of family, and descriptions of life events.
Multicomponent Psychoeducational Interventions
Multicomponent psychoeducational interventions involve a combination of dementia education, skill training, and coping strategies. Eight Level I studies provide strong evidence that multicomponent psychoeducational interventions improve caregiver QOL, well-being, and self-efficacy in managing problems (Corbett et al., 2012; Ducharme et al., 2011; Elliott, Burgio, & Decoster, 2010; Gitlin, Winter, Dennis, Hodgson, & Hauck, 2010a, 2010b; Kouri, Ducharme, & Giroux, 2011; Kuo et al., 2013; Livingston et al., 2013).
Multicomponent psychoeducational interventions to reduce caregiver depression and burden are supported by strong evidence from 6 Level I studies (Chien & Lee, 2008; Elliott et al., 2010; Elvish, Lever, Johnstone, Cawley, & Keady, 2013; Lee, Sung, & Kim, 2012; Marim, Silva, Taminato, & Barbosa, 2013; Moore et al., 2013), 2 Level II studies (Andrén & Elmståhl, 2008b; Mioshi, McKinnon, Savage, O’Connor, & Hodges, 2013), and 1 Level III study (Ponce et al., 2011). In addition, the Level I study by Chien and Lee (2008) and 1 Level II study (Andrén & Elmståhl, 2008a) provide moderate evidence that multicomponent psychoeducational interventions maintained the PWD at home longer.
Finally, insufficient evidence from 1 Level III study (Gitlin, Jacobs, & Earland, 2010) showed the translation of the Environmental Skill-building Program (ESP), now named Skills 2 Care ® , into home-based clinical practice was moderately successful, with 70% adoption by occupational therapists and close to 60% of eligible caregivers participating in the program. Of significance was the successful reimbursement of ESP/Skills 2 Care sessions through the patient’s Medicare Part B benefit when integrated into the occupational therapy plan of care.
Discussion
This review of the evidence for interventions supporting caregivers of PWDs has implications for occupational therapy practice, education, and research.
Implications for Practice
On the basis of this systematic review of the evidence, we recommend the following caregiver treatment approaches and interventions:
Integration of dementia education, behavior management strategies, communication skills, environmental modification, stress management, anger management, and coping skills
Implementation of cognitive reframing, mindfulness techniques, stress reduction strategies, and physical exercise or activity for caregivers who express anxiety, stress, and depressive symptoms
Interaction with caregivers to explain, discuss, and practice educational content rather than just handing the caregiver a folder with educational materials
Provision of information on respite options (in-home support and day care services) as part of educational content
Delivery of professionally led in-person support groups to increase caregiver preparation and confidence in managing memory loss in the PWD
Promotion of interaction between the caregiver and PWD through communication skills training and the use of memory books, photos of family members, and other memory aids
Provision of caregiver training and practice using assistive devices with or for the PWD (e.g., medication dispenser, raised toilet seat, monitoring system) to promote long-term use and carryover
Integration of caregiver interventions into the PWD’s occupational therapy plan of care to promote insurance reimbursement.
Implications for Education
Growing evidence supports caregiver interventions that are within the scope of occupational therapy practice. In addition, caregiver training and education are a vital component of the treatment plan for all PWDs and are reimbursable. Educators must ensure that students understand caregiver experiences and can deliver evidence-based interventions to family members and other informal caregivers of PWDs by integrating current evidence and specific examples of caregiver interventions into the curriculum and course assignments. Occupational therapy academic curricula and continuing education should include advocacy and policy skills training so students are able to advocate for caregivers and effect policy change to promote best practice in educating and supporting caregivers.
Implications for Research
Research is needed to evaluate the effectiveness and costs versus benefits of caregiver interventions under varying conditions (e.g., stage of dementia, severity of behavioral symptoms, caregiver health and readiness to implement strategies) to build evidence and support reimbursement. Delivery of support groups using telehealth methods shows promise; however, additional research is needed to evaluate its effectiveness and costs versus benefits. Further examination of intervention dosage (i.e., frequency and duration of intervention sessions) will help determine the most effective and efficient mode of delivery, thus supporting sustainability within the health care system. In addition, use of consistent outcome measures in caregiver intervention research would facilitate comparison of results. Last, evaluating longer term effectiveness of interventions over a 1-yr or greater time frame is needed because most studies evaluate outcomes only immediately after the intervention is completed.
Limitations
Limitations of reviewed studies involved sample size (more than 50% had <100 participants), study participant gender (the majority were female), and the use of different scales to measure caregiver outcomes (well-being, quality of life, and burden), limiting the ability to synthesize and external validity of results. In addition, the systematic review included studies that lacked follow-up, did not use a comparison group, and had a short intervention period. Finally, international studies may have limited generalizability to U.S. populations.
Conclusion
The interventions included in this systematic review provided education, training, and support for caregivers to facilitate performance of caregiver tasks and strategies and to promote caregiver well-being. These approaches are within the scope of occupational therapy and can be implemented by occupational therapy practitioners across multiple practice settings. Given the estimated increase in the number of PWDs over the next 30 years and the fact that family members and other informal caregivers provide the majority of care, continued research is needed to test the efficacy, effectiveness, and costs versus benefits of occupational therapy interventions that optimize caregiver skills and promote quality of life and well-being. In addition, further work is needed within occupational therapy to translate caregiver interventions into practice and evaluate the mechanisms for sustainability within the health care system.
Supplemental Material
Supplementary material for Effectiveness of Interventions for Caregivers of People With Alzheimer’s Disease and Related Major Neurocognitive Disorders: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2017.027581.pdf for Effectiveness of Interventions for Caregivers of People With Alzheimer’s Disease and Related Major Neurocognitive Disorders: A Systematic Review by Catherine Verrier Piersol, Kerry Canton, Susan E. Connor, Ilana Giller, Stacy Lipman and Suzanne Sager in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman and Marian Arbesman for their guidance and support throughout the systematic review process. A preliminary review of the data included in this article was presented at the 2015 AOTA Annual Conference & Expo in Nashville, TN.
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.