
Abstract
Occupational therapists have a long history of assessing functional cognition, defined as the ability to use and integrate thinking and performance skills to accomplish complex everyday activities. In response to passage of the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014 (Pub. L. 113–185), the American Occupational Therapy Association has been advocating that the Centers for Medicare and Medicaid Services consider functional cognition for inclusion in routine patient assessment in postacute care settings, with important implications for occupational therapy. These efforts have the potential to increase referrals to occupational therapy, emphasize the importance of addressing functional cognition in occupational therapy practice, and support the value of occupational therapy in achieving optimal postacute care outcomes.
The purpose of the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014 (Pub. L. 113–185) is to evaluate and realign the incentives and payment for postacute care (PAC) services provided under the Medicare program and to further the quality of service in PAC settings (i.e., long-term care hospitals, skilled nursing facilities, home health agencies, and inpatient rehabilitation facilities). The IMPACT Act also brings attention to related issues such as improving resource utilization, ensuring patient safety, reducing caregiver burden, and enhancing discharge planning and care transitions. Uniform data gathering tools would allow Medicare to collect identical data across PAC settings and evaluate the effects of PAC health care services on patients’ overall health and functional status over time.
The data collection changes now in development within the Centers for Medicare and Medicaid Services (CMS) in response to the IMPACT Act provide a significant opportunity for occupational therapy. Building on the occupational therapy profession’s understanding of the interrelationship of cognition and occupational performance, the American Occupational Therapy Association (AOTA) is advocating that CMS expand the data collection procedures that are standard in PAC settings to include data on functional cognition, defined as the ability to use and integrate thinking and performance skills to accomplish complex everyday activities. If functional cognition were added to standard data collection, occupational therapists would be in a position to assess and then intervene in this area so as to help Medicare beneficiaries achieve and maintain maximum function and independence.
The areas of emphasis for data and quality identified in the IMPACT Act include medical, functional, cognitive, and social supports. The IMPACT Act requires attention to these constructs for purposes of predicting postacute care resource needs, promoting continuity of care, avoiding preventable hospital readmissions, and achieving positive outcomes for Medicare beneficiaries as a result of receiving Medicare PAC services. The legislative language of the IMPACT Act emphasizes cognition for both patient assessment and quality measure construction and use. Further, in both of these categories, the IMPACT Act mentions functional status. In meetings with CMS and their consultants, AOTA has emphasized the links between cognition and functional performance and the belief that implementation of the IMPACT Act should make clear these links and reflect a broad interpretation of congressional intent.
In the statutory language of the IMPACT Act, cognition is specifically referenced in relation to the required collection of standardized patient assessment data in several key domains. In that section, cognitive function is described as the “ability to express ideas and to understand” (p. 1955). The same paragraph goes on to describe mental status using the examples of dementia and depression. In a separate section addressing the required development of quality measures, the IMPACT Act states that one of its key quality measurement domains is “functional status, cognitive function, and changes in function and cognitive function” (p. 1956).
Prior to the work of AOTA, CMS had been focused on the use of a particular set of assessment items originally developed as the Continuity Assessment Record and Evaluation (CARE) item set (Gage et al., 2012), established to identify the needs of patients in PAC settings. However, there are considerable limitations in the CARE item set, which, without augmentation, would provide only limited data on people with mild cognitive impairment and could therefore fail to identify people with impairments in essential instrumental activities of daily living (IADLs; Jekel et al., 2015). The CARE item data bank currently contains the Confusion Assessment Method (CAM) to identify patients with delirium (Inouye et al., 1990; Wei, Fearing, Sternberg, & Inouye, 2008) and the Brief Interview for Mental Status (BIMS) to identify patients with moderate to severe deficits in memory and orientation (Saliba et al., 2012). Both measures appear to be working adequately to meet these goals. However, the CAM and BIMS items do not capture the capacity to use and integrate thinking and processing skills to accomplish complex everyday activities (i.e., to use functional cognition to accomplish essential IADLs).
Why Address Cognition?
Subtle, but significant, cognitive impairment (terms vary and include mild cognitive impairment and cognitive impairment no dementia) is common in patients in PAC settings (Buslovich & Kennedy, 2012). Cognitive impairment not severe enough to meet diagnostic criteria for major neurocognitive disorder (e.g., dementia) is now widely recognized as being associated with impaired performance of essential IADLs (Gure, Langa, Fisher, Piette, & Plassman, 2013; Jekel et al., 2015; Puente, Terry, Faraco, Brown, & Miller, 2014). Essential IADLs include health management and maintenance (e.g., nutrition, medication management), financial management (e.g., managing finances with long-term and short-term goals), and community mobility skills (e.g., driving, using public transit; AOTA, 2014). Impaired functional cognition critically affects safety, resource utilization, outcome stability, and burden of care and has been established as occurring frequently in chronic neurological and systemic diseases (Baum & Edwards, 1993; Cahn et al., 1998; Klepac, Trkulja, Relja, & Babić, 2008).
As noted in the AOTA (2013) official statement Cognition, Cognitive Rehabilitation, and Occupational Performance, occupational therapists believe that cognition can be adequately assessed only through the evaluation of function. Consistent with this belief, AOTA recommended to CMS that the assessment of cognition be broadened beyond how it was being evaluated in PAC settings. AOTA noted that assessment of cognition and functional status as described in the legislation would not fully achieve the congressional goals of the IMPACT Act. AOTA proposed the development and incorporation of new tools to measure functional cognition to be included in the IMPACT Act data element library and used in PAC settings. In addition, AOTA proposed that CMS gather data on and include functional cognitive performance as a key aspect of assessment data and quality measures and also as a component affecting care planning and resource utilization. Figure 1 illustrates the potential place of functional cognition in a schematic presentation of cognitive processes related to certain diagnoses and associated assessment tools.
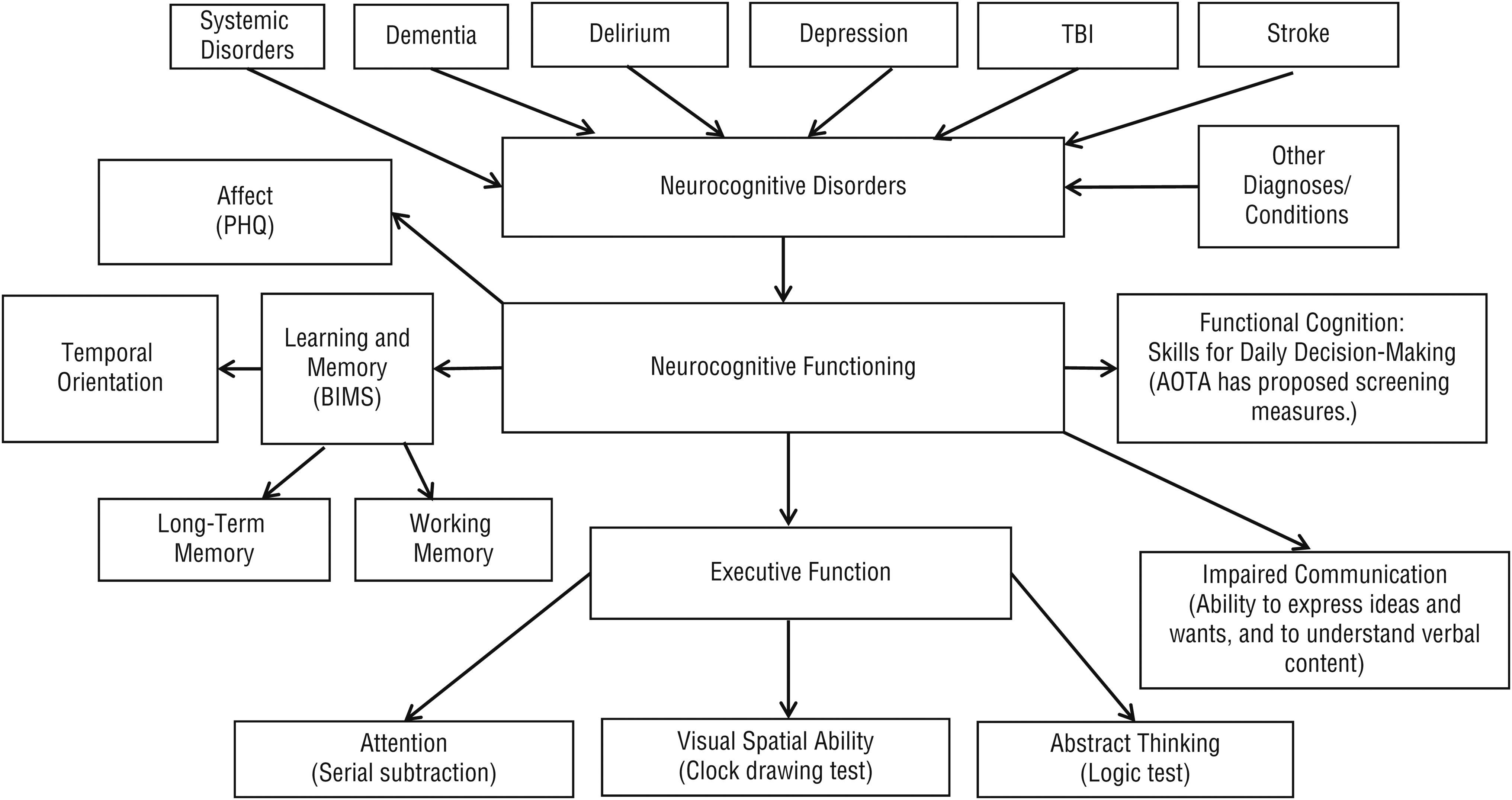
Schema representing cognitive processes and associated assessments for use in postacute care settings.
Assessing Functional Cognition
Functional cognition influences how an individual uses and integrates thinking and processing skills to accomplish everyday activities in clinical and community living environments. Rather than attempt to isolate specific cognitive functions, occupational therapy practitioners administer assessments and interventions that focus on cognition as it relates to the performance and accomplishment of everyday life activities. Practitioners recognize that the performance of essential IADLs involves the use of multiple cognitive and performance skills in concert (Law, Barnett, Yau, & Gray, 2012). Occupational therapy scientists have been developing the concepts of performance-based testing for the last 20 years (Baum & Edwards, 1993). In occupational therapy, performance-based tests have been used to assess the ability of adults across diagnostic groups to live independently in the community (Moore, Palmer, Patterson, & Jeste, 2007; Poulin, Korner-Bitensky, & Dawson, 2013; Wesson, Clemson, Brodaty, & Reppermund, 2016). Performance-based tests of functional cognition are intended to assess the patient at the performance level across several functional domains, including cognition, in real-world contexts (AOTA, 2014).
Critical to the argument put forward by AOTA is that the use of performance-based testing of functional cognition can augment assessments currently in use. Accurate assessment of patients in postacute care settings poses challenges for health care providers. Neuropsychological measures of isolated cognitive function are insufficient to assess capacity and predict everyday life performance (Law et al., 2012; Manchester, Priestley, & Jackson, 2004). Neuropsychological tools used to evaluate cognitive function are highly structured (Lezak, Howieson, Bigler, & Tranel, 2012), obviating their usefulness in predicting IADL performance in populations with compromised initiation and self-organization, and measures are structured in a way that prevents people from using the experience and knowledge supporting task performance they have gained over a lifetime (Law et al., 2012).
Self-report is the most common approach used to assess functional status in older adults. However, changes in cognition, affect, motivation, self-efficacy, and functional status can influence the accuracy of self-reported functional ability (Burnett, Dyer, & Naik, 2009; Patterson & Harvey, 2008). Findings of only weak associations between self-evaluation and real-world functioning are ubiquitous (Burnett, Cully, Achenbaum, Dyer, & Naik, 2011; Cella et al., 2012). The accuracy of self-report measures is potentially compromised in people with neurological and systemic or traumatic disorders by their unawareness of limitations, denial of deficits, lack of opportunity to experience the changed self generally, and more specifically lack of opportunity to experience success or failure in complex IADL tasks (Morrison, Edwards, & Giles, 2015). Evidence also indicates that proxy measures may not be reliable for rating IADL function and can result in over- or underreporting of deficits (Jekel et al., 2015; Zanetti, Geroldi, Frisoni, Bianchetti, & Trabucchi, 1999). Performance-based tests (PBT) have repeatedly been found to outperform other forms of assessment in older adults in predicting real-world functioning (Jekel et al., 2015; Puente et al., 2014; Schmitter-Edgecombe, Parsey, & Cook, 2011).
AOTA has argued that the IMPACT Act provides an opportunity to further ensure that the types of deficits in functional cognition that may affect essential IADLs and the ability to safely sustain community living are addressed. Occupational therapists have traditionally used PBT incorporating everyday activities (real or simulated) to assess functional competency. The activities chosen for PBT must have high potential to engage patients in the task (Schutz & Wanlass, 2009). Additionally, PBT must be sound psychometrically, have the ability to be administered and scored rapidly, and have outcomes that can be communicated in a meaningful way to various stakeholders (Morrison et al., 2015). Performance-based testing is also used to evaluate likely postdischarge level of functioning, including self-care and personally valued roles, routines, and activities. The use of validated performance-based assessment of functional cognition would assist occupational therapy practitioners in implementing the appropriate interventions in PAC settings and in establishing the necessary support to maximize patients’ ability to function in their postdischarge environment.
Evidence Relating IADLs and Functional Cognition to the Goals of the IMPACT Act
The assessment of IADL performance and functional cognition can be predictive of health care resource utilization, thereby leading to reduced caregiver burden and optimal discharge planning and placement. Although observation of activities of daily living (ADLs) or assessment of capacity for ADLs is a component of PAC assessment across settings, IADLs are not readily observable in most PAC settings but are nonetheless critical to success in community living. Traditional cognitive screening tools (e.g., Mini-Mental State Examination; Folstein, Folstein, & McHugh, 1975) have been found to be predictive of hospital admission and burden of care (Joray, Wietlisbach, & Büla, 2004), but these tools are not as sensitive or consistently predictive of health resource utilization as measures of executive function or IADL performance (Buslovich & Kennedy, 2012). Traditional cognitive screening tools may fail to capture anything but relatively severe deficits in cognitive skills and more specifically may fail to identify deficits in executive functions associated with deficits in IADLs (Grigsby, Kaye, Baxter, Shetterly, & Hamman, 1998; Hanks, Rapport, Millis, & Deshpande, 1999).
Assessments of complex and integrated cognition functions (e.g., executive functions) have been found to be independently predictive of hospital readmission and long-term medical resource utilization (Dong et al., 2010; Naik, Burnett, Pickens-Pace, & Dyer, 2008). The fact that hospital readmission is often not directly related to the health care condition that precipitated the first admission has led to the recognition of a posthospital syndrome of generalized increased risk (Krumholz, 2013). Stress, nutritional deficiency, alteration in sleep pattern, deconditioning from bed rest, and medication effects can all potentially compromise posthospitalization cognitive status (Krumholz, 2013) and essential IADLs, suggesting that a screening of functional cognition should not be restricted to patients with diagnoses specifically associated with altered cognitive status.
Performance-Based Testing, Identification of Functional Cognition Limitations, and Promotion of Occupational Therapy
As DeJong (2017) noted, the U.S. health care system is in a period of transition, moving away from a fee-for-service model and toward bundled and population-based payments and quality as measured by postdischarge health care outcomes. The importance of a health care discipline will be judged increasingly by how it adds value to overall patient outcomes (DeJong, 2017). Health care providers need to determine whether and how patients safely and effectively perform essential IADLs, such as medication management and community mobility, to help identify patients at risk for self-neglect and to guide PAC care transition placement, discharge decisions, and patient and caregiver training.
Occupational therapists have used PBTs to assess the ability of adults across diagnostic groups to live independently in the community (Moore et al., 2007; Poulin et al., 2013; Wesson et al., 2016). PBTs of functional cognition are intended to assess the patient at the performance level across several functional domains in real-world contexts. In general, these tasks have greater cognitive than physical emphasis and require the integration of multiple sources of information and sequencing of multiple action steps for goal completion.
As noted, AOTA has proposed to CMS the development and use of performance-based screening measures of functional cognition. Use of such screening tools is intended to better identify patient needs, determine interventions, and predict patient postacute care outcomes in terms of safety, outcome stability, burden of care, resource utilization, and reduced rehospitalizations. People who pass screens (i.e., are negative) for delirium (CAM) and for moderate to severe memory deficits (BIMS) could be administered the functional cognition screening tool. Failure on a functional cognition screening tool could be used to cue referrals to occupational therapy for further evaluation and for intervention or implementation of support services. To be feasible in postacute care settings, the screening tool would need to meet the following criteria: be able to be administered by any health care discipline, be able to be administered bedside and across subacute settings, be transdiagnostic, entail low respondent burden (<5 min), entail low administrative burden (e.g., simple to learn, quick to administer, easy to score and interpret), require no equipment (other than paper and pencil), and be sensitive to mild to moderate levels of impairment.
AOTA has proposed potential screening tools to be used for this purpose (i.e., to trigger referral of patients with suspected impairment in functional cognition to receive a comprehensive evaluation from an occupational therapist). Were CMS to adopt these recommendations, a new referral stream to occupational therapy would be initiated, and Medicare beneficiaries with impaired functional cognition would gain access to needed services with the potential to reduce hospital recidivism and failure to sustain postdischarge placement (Rogers, Bai, Lavin, & Anderson, 2016).
Conclusion
AOTA has recommended to CMS that as part of the response to the IMPACT Act, a performance-based screening assessment of functional cognition be adopted for inclusion in routine PAC data collection. The proposed functional cognition screening tool would be multidisciplinary, rapid to learn, and quick to administer, score, and interpret and would require minimal equipment and be robustly predictive of impaired IADL performance. AOTA has recommended screening tools that measure functional cognition that could be piloted and validated for use in postacute settings and that could be administered by staff of various disciplines. Such functional cognition screening tools would have ecological validity and high face validity.
Adoption of performance-based screening tools for functional cognition would address the gap in care CMS has identified in postacute care settings. Impaired performance on a functional cognition screening tool would prompt referral to occupational therapy for further assessment and intervention and would contribute to predicting care resource needs, promoting continuity of care, avoiding preventable hospital readmissions, and achieving positive outcomes for Medicare beneficiaries.
Footnotes
Acknowledgment
The authors acknowledge the contributions of AOTA staff Sharmila Sandhu, Jennifer Bogenrief, and Christina Metzler in completing this article.