
Abstract
This study examined whether sensory modulation disorder–sensory overresponsivity (SMD–SOR) and attention deficit hyperactivity disorder (ADHD) have a significant effect on the perception of aversive auditory stimuli. Participants were 66 young adult women. The diagnosis of SOR was made using the Sensory Responsiveness Questionnaire, and ADHD was diagnosed by a qualified psychiatrist or neurologist using criteria from the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Participants were presented with the Battery of Aversiveness to Sounds, short presentations of daily life sounds, and rated each sound stimulus verbally according to its perceived unpleasantness. Participants with SOR rated low-intensity aversive sounds as significantly more aversive than participants without SOR. High-intensity sounds obtained a marginal significant difference exclusively in participants with ADHD. The perception of aversive auditory stimuli in adults with SOR appears to be unique and different than the profile of adults with ADHD.
Sensory modulation is the ability to regulate and grade responses to the sensory environment so that responses to sensory input are appropriate to the demands of daily life (Miller et al., 2007). Sensory modulation disorder (SMD), a subtype of sensory processing disorder, refers to a person’s difficulty in responding to sensory stimuli with an adaptive and graded behavior. SMD results when a person has difficulty achieving and maintaining emotional, attentional, or motoric responses to sensory stimuli (Miller et al., 2001, 2007). Three subtypes of SMD are recognized: sensory overresponsivity (SOR), sensory underresponsivity, and sensory seeking/craving (Interdisciplinary Council on Developmental and Learning Disorders, 2005; Miller et al., 2007; Zero to Three, 2005).
SMD in adulthood is associated with mental health and social–emotional issues and decreased coping strategies (Jerome & Liss, 2005; Kinnealey & Fuiek, 1999). Researchers assert that sensory modulation problems across the life course can negatively affect a person’s quality of life and activity choices (Bar-Shalita et al., 2015; Blanche et al., 2014; Kinnealey et al., 2011). SMD has been accentuated as one of the areas of particular importance recommended for extended coverage in the World Health Organization’s (2001) International Classification of Function, Disability and Health (Simeonsson et al., 2003).
Sensory modulation problems in adults have been present, in most cases, since childhood and throughout the course of life (May-Benson, 2011; Oliver, 1990). Research on adults with SMD is scarce. The few existing studies (Jerome & Liss, 2005; Kinnealey & Fuiek, 1999; Kinnealey et al., 1995; Liss et al., 2005; Pfeiffer & Kinnealey, 2003) have focused on SOR, a condition in which sensations are felt more intensely and for a longer duration than is typical. Otherwise benign sensations are experienced as unpleasant, distracting, or even painful. Overresponsiveness to sensory stimuli, especially somatosensory and auditory, can have a negative effect on social interactions as well as participation and engagement in everyday occupations (Kinnealey et al., 1995, 2011).
Possible behavioral expressions of SMD such as distractibility, hyperactivity, and impulsivity in children (Mangeot et al., 2001; Miller et al., 2012; Mulligan, 1996) and in adults (Kinnealey et al., 1995, 2011) are also the constituents of attention deficit hyperactivity disorder (ADHD) as classified in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM–IV–TR; American Psychiatric Association [APA], 2000; and 5th ed.; DSM–5; APA, 2013). ADHD is among the most common and widely researched early childhood developmental disorders. The DSM–5 (APA, 2013) criteria state a prevalence of 5% among children in most cultures with a ratio of 2 boys to 1 girl in the general population. ADHD is not outgrown in adulthood. Ten percent to 60% of young adults with ADHD were diagnosed with the disorder as children, and up to 5% of the adult population has ADHD (Faraone et al., 2000). High comorbidity rates of SMD and ADHD have been reported (Miller et al., 2001; Parush et al., 1997; Yochman et al., 2006).
The diagnostic assessment of SMD in adults uses standardized questionnaires and informal interviews. Such self-report assessments—that is, the Adolescent/Adult Sensory Profile (Brown & Dunn, 2002), the Sensory Responsiveness Questionnaire (SRQ; Bar-Shalita et al., 2009), and the recently developed Adult Sensory Processing Scale (Blanche et al., 2014)—can be referred to as subjective assessment tools. In this respect, the term subjective refers to the person’s self-evaluation of his or her sensory patterns of responsiveness. A standard method of assessment for adults that uses an examiner-administered scale (i.e., a performance measure) does not exist. The newly developed Sensory Processing Scale (SPS) Assessment (Schoen et al., 2014) is aimed at filling this void with a standardized objective exploration of sensory modulation. The SPS Assessment uses direct observation of all sensory domains to assess behavioral responses to sensory occurrences that are similar to daily life experiences. Unfortunately, the SPS Assessment does not target the adult population. Future development of more direct and objective methods to diagnose adults with SMD is an important step toward a better understanding of the underlying mechanisms and consequently for the advancement of effective therapeutic measures.
The most common domains of SOR studied are tactile and auditory, both of which affect the ability to perform everyday activities (Schoen et al., 2008). Goldsmith and colleagues’ (2006) population-based twin study reported that auditory and tactile SOR were largely distinct from other common childhood disorders. Some researchers have chosen only tactile and auditory defensiveness as markers of a broader sensory defensiveness (Goldsmith et al., 2006; Van Hulle et al., 2012).
Taking into account that certain behavioral expressions of SMD are often similar to those of ADHD in pediatric and adult populations, and the high comorbidity rates between these two diagnoses, the purpose of this study was to investigate the possible differential perception of auditory stimuli among participants with SOR and ADHD. Specifically, the current study sought to answer the following research question: Does the presence of SMD–SOR, ADHD, or both have a significant effect on the perception of aversive auditory stimuli?
Method
The Ethics Committee of the School of Occupational Therapy, Faculty of Medicine, Hebrew University of Jerusalem, approved all procedures for this study.
Participants
Sixty-six young adult women aged 18–34 yr (mean [M] = 25.03, standard deviation [SD] = 3.47) participated in this study. Study participants were university students, some fulfilling course requirements. All participants had completed at least 12 yr of education and had normal hearing and normal or corrected to normal vision. A comparison between the study groups’ ages using 2 × 2 analysis of variance (ANOVA) indicated no significant difference in age between participants with and without ADHD, F(1, 62) = 2.81, p = .10, and between participants with and without SMD, F(1, 62) = 2.69, p = .11, and no significant interaction effect of ADHD × SMD, F(1, 62) = 1.97, p = .16. See Mazor-Karsenty et al. (2015) for further details of participants’ demographic characteristics and the classification measures of the study.
Initially, we intended to recruit a balanced gender sample. However, we encountered considerable difficulty in recruiting adult men for the SMD group, which, in turn, obligated an exclusively female study. In retrospect, this gender bias is supported by several research articles published on SMD in adults (Kinnealey & Fuiek, 1999; Kinnealey et al., 1995, 2011; Pfeiffer & Kinnealey, 2003). It is also supported by the higher rates of sensory sensitivity in Israeli women compared with men as reported by Engel-Yeger (2012).
Participants With SMD.
Twenty women with SMD participated in this study. They were diagnosed for SMD–SOR according to the SRQ. They had no known psychological, medical, or learning disorder according to self-report. The MATAL ADHD Questionnaire (Ben-Simon, 2007) was used to screen for no ADHD. A short interview verified no ADHD diagnosis in childhood or at the present time.
Participants With ADHD and SMD.
Twenty women with ADHD and SMD took part in this study. ADHD was diagnosed by a qualified psychiatrist or neurologist based on DSM–IV–TR (APA, 2000) criteria. Diagnosis for SMD–SOR was made according to the SRQ.
Participants With ADHD and No SMD.
Six female participants had ADHD without SMD. ADHD was diagnosed according to criteria described in the previous section. The SRQ served as a screening tool to verify no SMD.
Healthy Participants.
Twenty female participants with no SMD and no ADHD were recruited. Inclusion criteria were similar to those mentioned previously for the SMD group with the exception of the SRQ serving as a screening tool to verify no SMD.
Procedure
The following testing procedure was part of a larger study, parts of which were recently reported (Mazor-Karsenty et al., 2015). Testing took place at the neurocognition laboratory at the School of Occupational Therapy, Hebrew University, Jerusalem. All participants read a brief explanation regarding the testing process and signed an informed consent. We then administered the Battery of Aversiveness to Sounds (BAS; developed by the first and last authors).
Measure
The BAS includes 10 standardized sound presentations of 30 s duration each (3 times each, 30 sound presentations in total) that are based on comprehensive and detailed interviews with adults with SMD and on literature review (Kinnealey et al., 1995; Miller, 2006; Schoen et al., 2008). Sounds were recorded using a waveform audio file format and programmed into a p file. The sounds in the BAS are dish (eating utensils scratching dish), apple eating, ocean waves, rain, clock ticking, high pitch tone, water drops, alarm, machinery (construction equipment), and birds chirping. A Dell (Round Rock, TX) laptop controlled auditory stimuli presentation. All sounds were presented binaurally in pseudorandom order via Koss (Milwaukee, WI) TD-80 headphones with an intensity range of 55–80 dB. Participants were asked to rate each sound stimulus according to its perceived unpleasantness (level of aversiveness) on a visual analog scale of 0 (no unpleasant sensation) to 10 (the most unpleasant sensation imaginable) adapted from Price et al. (1983). Every participant rated each sound three times and a mean score for each sound was calculated.
Data Analysis
The data were analyzed with IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY). To compare between study groups regarding the 10 sound presentations in the BAS, we performed descriptive statistics (means and standard deviations) as a first step. We then analyzed the sounds using a 2 (SMD/No SMD) × 2 (ADHD/No ADHD) factorial ANOVA where the dependent variables were the unpleasant sensation ratings of each sound. The 2 × 2 factorial design, in which the factors of ADHD and SMD were analyzed independently, was used to investigate the effects of ADHD and SMD independently. In this method, the comparison was between the participants with SMD (n = 40) and those without SMD (n = 26) and between participants with ADHD (n = 26) and those without ADHD (n = 40).
Because the sounds in the BAS represent a spectrum of intensity, although a narrow one (55–80 dB), we calculated a new variable that grouped the 10 sounds into three categories according to their intensity levels: high-intensity sounds (78–80 dB), calculated from the mean level of aversiveness to high pitch (80 dB), alarm (80 dB), rain (78 dB), and machinery (78 dB); medium-intensity sounds (63–74 dB), mean level of aversiveness to clock (63 dB), waves (70 dB), and birds (74 dB); and low-intensity sounds (55–60 dB), mean level of aversiveness for apple (55 dB), water drops (55 dB), and dish (60 dB). With the purpose of examining the effects of SMD and ADHD on the level of aversiveness to each of the three intensity levels, a 2 × 2 × 3 factorial ANOVA was carried out.
Results
Table 1 outlines participants’ BAS scores by study groups. A closer inspection revealed that there might be specific effects of the factors of SMD and ADHD on some of the sounds (e.g., waves, rain, clock, high pitch, water drops, birds). With the purpose of examining whether there were differences between groups regarding level of aversiveness to each of the 10 sounds, a 2 (SMD/No SMD) × 2 (ADHD/No ADHD) factorial ANOVA was carried out (see Table 1).
Participants' BAS Scores by Study Group and Between-Subjects Effects for the 2 (SMD or No SMD) × 2 (ADHD or No ADHD) Factorial ANOVA
Note. ADHD = attention deficit hyperactivity disorder; ADHD+ = participants with ADHD; ADHD– = participants without ADHD; ANOVA = analysis of variance; BAS = Battery of Aversiveness to Sounds; M = mean; SD = standard deviation; SMD = sensory modulation disorder; SMD+ = participants with SMD; SMD– = participants without SMD.
p < .05.
Because the BAS sounds have a spectrum of intensity (55–80 dB), we hypothesized that the intensity level of sounds might affect the perceived level of aversiveness of participants according to their group placement. We therefore calculated three new variables that grouped the 10 sounds according to their intensity levels (low, medium, and high, discussed previously). The design for analysis included two between-group variables (SMD, ADHD) and one within-subject variable (sound intensity). It was performed using a 2 × 2 × 3 (SMD × ADHD × Sound Intensity) ANOVA with repeated measures on intensity.
A significant interaction effect was found for Intensity × SMD, F(2, 124) = 3.274, p = .041, ηp 2 = 0.050. No similar interaction effect was observed for Intensity × ADHD, F(2, 124) = 0.857, p > .05). An independent samples t test was conducted to compare intensity levels in SMD and non-SMD conditions (Figure 1). There was a significant difference in the low-intensity scores for SMD (M = 7.01, SD = 1.69) and non-SMD (M = 5.82, SD = 1.96) conditions, t(64) = –2.610, p = .011. There was not a significant difference in the medium-intensity scores for SMD and non-SMD conditions, t(64) = –0.546, p > .05, or in the high-intensity scores for SMD and non-SMD conditions, t(64) = –0.931, p > .05. These results suggest that only the low-intensity sounds differentiate between participants with and without SMD. Specifically, our results suggest that people with SMD perceive low-intensity sounds as significantly more aversive than those who do not have SMD. Interestingly, this significant result was obtained only for the low-intensity sounds.
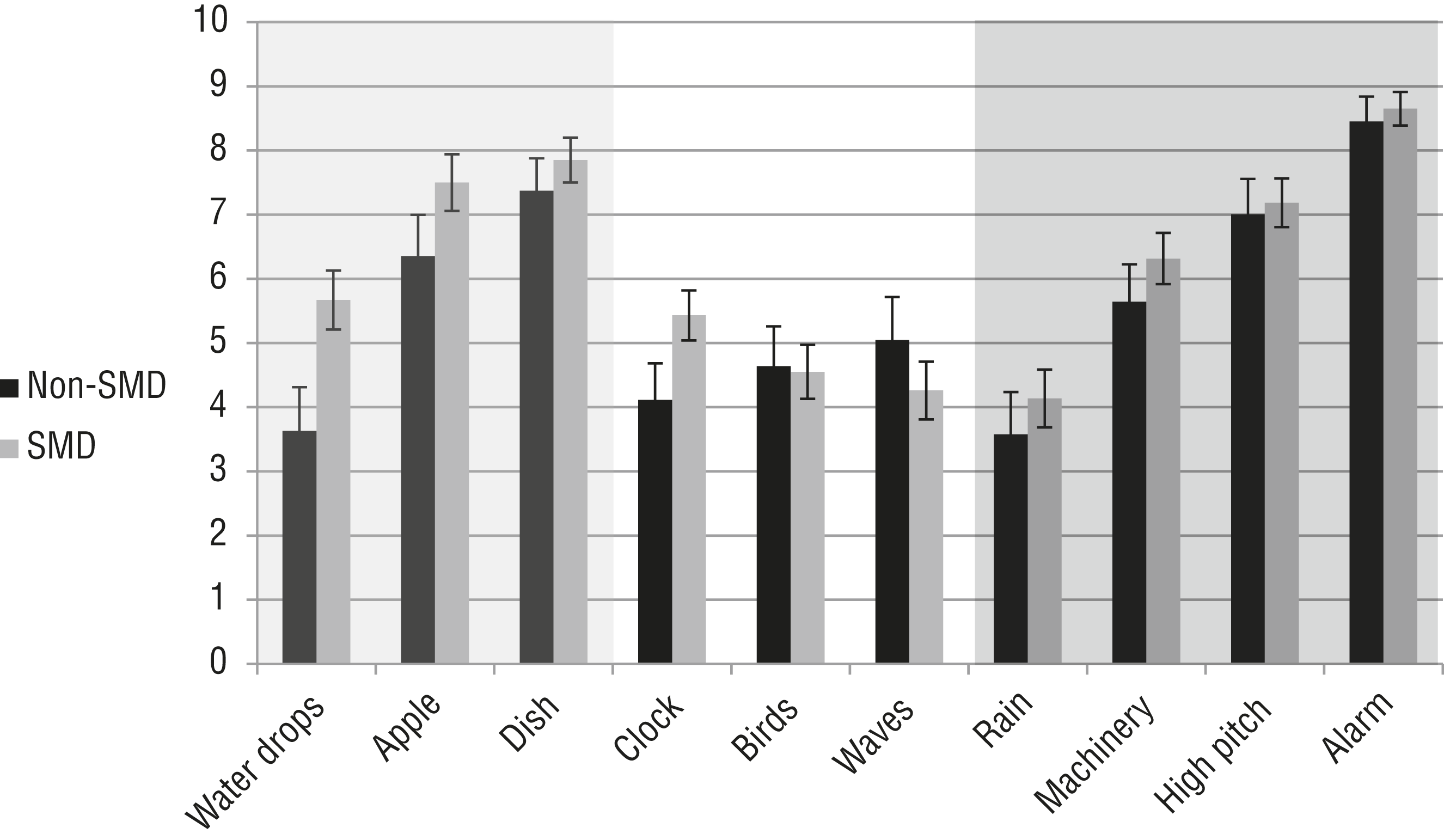
Participants’ BAS scores according to sound intensity levels for those with and without SMD. For low-intensity sounds, the effect of SMD is the largest.
For the ADHD factor, a closer examination of the difference between means on each intensity level revealed a larger disparity between participants with and without ADHD in the high-intensity sounds (no ADHD: M = 6.08, SD = 2.07; with ADHD: M = 6.86, SD = 1.51) and the medium-intensity sounds (no ADHD: M = 4.32, SD = 1.95; with ADHD: M = 5.14, SD = 1.63) compared with the low-intensity sounds (no ADHD: M = 6.32, SD = 2.03; with ADHD: M = 6.872, SD = 1.60). Interestingly, when we carried out a 2 × 2 (SMD × ADHD) multivariate ANOVA to examine whether there were differences between groups regarding level of aversiveness to the four high-intensity sounds (high pitch, alarm, rain, and machinery), a significant difference was obtained for ADHD, F(4, 59) = 2.477, p = .05, ηp 2 = 0.144. No difference was obtained for ADHD regarding the medium-intensity sounds, F(3, 60) = 1.40, p > .05, or the low-intensity sounds, F(3, 60) = 0.201, p > .05.
Discussion
The standardized BAS enables a direct psychophysical measurement of sensory responsivity in one specific modality, the auditory one. Using the BAS, the current study set out to examine the possible differential role of SMD and ADHD in the perception of aversive auditory stimuli.
Initial descriptive statistics indicated possible group differences in participants’ perceived aversiveness. There were sounds that seemed to elicit high levels of unpleasant sensations, such as the dish and the alarm, in all study participants. Specifically, the similar levels of perceived aversiveness for the alarm suggest a ceiling effect for all groups. The other eight sounds evoked a more heterogeneous pattern. Therefore, we investigated this diversity in physical quality, or intensity level, of each sound stimulus. Results indicate a different and unique profile for SMD and ADHD. SMD had a significant effect only on low-intensity sounds but not on medium and high ones. The high-intensity sounds obtained a marginal significant difference exclusively in participants with ADHD.
Noise is known to generally increase arousal and stress levels (Hommel et al., 2012). Studies conducted on noise (auditory or visual) in people with ADHD have referred to the effects of these distracting conditions on cognitive performance, arguing whether they hinder or facilitate such performance (Lineweaver et al., 2012; Söderlund et al., 2007, 2010). Extensive efforts have been made to investigate the effects of noise on nonauditory aspects of performance, such as attention, information processing, and memory, in healthy people. A large meta-analytical study showed that effects of noise depend on the type of noise and the nature of the activity being performed (Szalma & Hancock, 2011). Alternative views (Smith, 2012) relate to a person’s beliefs and perception of the aversiveness of the noise, which interact with task demands and instructions as well as the person’s individual perception of what is competent performance.
There are no comparable studies in which the perception of auditory aversiveness has been measured among people with SMD. In studies of sensory modulation dysfunction in children (Mangeot et al., 2001; McIntosh et al., 1999) using the sensory challenge protocol and electrodermal reactivity (EDR), researchers concluded that reactivity was consistent across sensory domains, therefore averaging data across sensory modalities. No data were made available about the specific effects of the auditory stimulus (in these cases, a 90-dB siren). More recently, using the same sensory challenge protocol, Miller et al. (2012) demonstrated that the EDR magnitudes of children with SMD were significantly greater than those for children with ADHD and typically developing children in response to auditory, visual, and movement stimuli. In all sensory domains, there were no significant differences between ADHD and typically developing children. Yet, again, only one auditory stimulus was used (a 90-dB siren). In the current research, high-intensity sounds (e.g., the 80-dB alarm) elicited high rates of aversiveness, regardless of group placement.
Many studies have reported on the difficulty of screening out irrelevant sensory stimuli in children (Cohn et al., 2000; Miller et al., 2007) and adults (Jerome & Liss, 2005; Kinnealey & Fuiek, 1999; Kinnealey et al., 1995, 2011; Liss et al., 2005; Pfeiffer & Kinnealey, 2003) with SMD–SOR. To date, no study has attempted to characterize these irrelevant sensory stimuli. However, our results indicate that specifically for auditory stimuli, these stimuli should not be regarded as a homogeneous group. Why do participants with SMD perceive low-intensity sounds as more aversive? To give a concrete idea of the meaning of low intensity, quiet conversation corresponds to an intensity of about 50 dB (Khalfa et al., 2004). Dunn (2008) mentioned that sensitive people may notice sounds others do not notice at all, such as the sound of a refrigerator or a toilet flushing. Could this possibly be the reason why people with SMD–SOR frequently describe ordinary, daily sounds (e.g., hearing other people chewing or using eating utensils) as particularly irritating?
The differentiation between SMD and ADHD has been the object of several research groups in the past two decades, with preliminary and promising results indicating that SMD and ADHD may be different diagnostic categories (Miller et al., 2012; Parush et al., 2007; Yochman et al., 2013). The ability of the BAS to distinguish between the SMD and ADHD factors, indicating a unique profile for each factor, is a first step in the characterization of SOR in adults. We recently demonstrated that SMD is uniquely associated with impaired conflict resolution only when aversive sounds were presented (Mazor-Karsenty et al., 2015). This unique interaction effect of SMD and aversive sounds was obtained exclusively in participants with SMD, without a parallel effect among participants with ADHD (who displayed a core deficit in executive attention).
A more in-depth inquiry regarding the physical characteristics of diverse sounds is necessary. Features studied in such an inquiry should include the type, intensity, and frequency of sounds; whether there is a task involved and what type of task; the contexts of sounds; and the duration of exposure. An exhaustive characterization of SOR should include, of course, all sensory modalities. A step in the direction of characterizing the somatosensory profile of adults with SMD demonstrated that adults, similarly to children, have normal sensory thresholds but altered nociceptive suprathreshold sensations (Bar-Shalita et al., 2012). These findings make an important contribution to the pathophysiology of SMD, but the inability to differentiate between SMD and ADHD in the study sample impedes study conclusions.
This study has several limitations. The primary limitation is gender homogeneity. In retrospect, this gender bias is supported by the few articles published on SMD in adults, as discussed previously. The second limitation is the small sample size in the ADHD without SMD group. Note, however, that numerous studies have shown that most children, adolescents, and adults who meet diagnostic criteria for ADHD also meet criteria for at least one additional psychiatric disorder. Some meet criteria for several different disorders at the same time (Brown, 2013). A third limitation is that participants were university students; therefore, the study sample may not be representative of people with ADHD or SMD in the general population.
Implications for Occupational Therapy Practice
Future research should address the urgent need for a standardized direct psychophysical assessment tool for the diagnosis of SMD in adults and compare it to existing self-report measures. Both assessment types provide distinct types of information. Combining respondent and performance data has the potential to add predictive accuracy to the diagnosis of SMD. It is recommended that a direct psychophysical measure consider findings from the current research, that is, the physical aspects of sounds contribute to a differential perception of aversiveness, in the selection of auditory sounds. In conclusion, the major implications for occupational therapy practice and research are
The BAS may be useful as part of a direct psychophysical clinical assessment targeting the auditory system.
The BAS is a psychophysical tool that may be useful in differentiating SMD from other disorders in adults.
The BAS may be useful in helping to formulate appropriate interventions.
Low-intensity auditory stimuli have a potential to aid in the differential clinical diagnosis of SMD from ADHD.
Research involving the BAS may assist in studying the relationship between distinct auditory processing patterns of adults and participation and quality of life.
Conclusion
The perception of aversive auditory stimuli in adults with SMD appears to be unique and opposed to the profile of adults with ADHD. The BAS demonstrates that only low-intensity sounds have a significant effect on people with SMD, whereas high-intensity ones have a significant effect on people with ADHD. These findings further support our previous findings that differentiate SMD from ADHD on an executive attention task (Mazor-Karsenty et al., 2015). More research is needed to characterize the specific pathophysiology of people with SMD in all sensory modalities, aiding the development of direct measurement tools and subsequently enriching the assessment process of SMD. Direct psychophysical tests may provide information aiding the clinician’s understanding of each individual’s specific sensory challenges, whereas subjective self-reports might offer a glimpse into the client’s quality of life. This information, in turn, may eventually lead to the development of precisely tailored interventions that support participation.