
Abstract
Similar to many areas of clinical research (National Institutes of Health, 2010), addiction research has traditionally focused on men, who have been the primary consumers of substance abuse (SA) treatment (Greenfield et al., 2007). Recently, the rate of women seeking treatment for SA has increased, and the numbers of male and female heroin and cocaine users are nearly equal (Substance Abuse and Mental Health Services Administration [SAMHSA], 2012). Although the rate of substance dependence among men is almost twice that among adult women, the rate among youth is the same (Center for Behavioral Health Statistics and Quality, 2012). Women typically enter SA treatment with increased medical, psychological, and social needs (Greenfield, Back, Lawson, & Brady, 2010) and have been found to be more susceptible to cravings than men (Hitschfeld et al., 2015; Kennedy, Epstein, Phillips, & Preston, 2013). Although women are less likely than men to report marijuana or alcohol use, they are more likely to report nonmedicinal use of prescription drugs (Cotto et al., 2010; Greenfield et al., 2010), with women ages 65 yr and older reporting primary abuse of prescription pain relievers nearly 3 times as often as men on admission to treatment (SAMHSA, 2014).
Since the 1990s, emerging women-only treatment programs have featured well-baby services, job training, and housing assistance (Grella, Polinsky, Hser, & Perry, 1999). However, comprehensive details about the specific characteristics and features of these interventions have not been compiled in the literature. In this article, we present the findings of a scoping review undertaken to describe the characteristics and features of SA interventions for women found in the peer-reviewed literature and discuss the implications from an occupational perspective.
Background
Unique Needs of Women With Substance Abuse Issues
The increase in the number of women’s SA programs since the 1990s can be attributed to gender differences in SA issues, including initiation of substance use, progression to dependence, and social factors influencing engagement in treatment (Greenfield & Grella, 2009). Women are also more likely to have other mental health concerns (Green, 2006; Greenfield et al., 2010). The National Institute on Drug Abuse (NIDA; n.d.) has estimated that as many as 80% of women seeking treatment report experiences of sexual assault, physical assault, or both, with more than half presenting with symptoms of posttraumatic stress disorder (Najavits, Weiss, & Shaw, 1997). Furthermore, women often demonstrate telescoping, which is described as a rapid progression from initiation of use through dependence leading to treatment (Hernandez-Avila, Rounsaville, & Kranzler, 2004; Randall et al., 1999). Women may also be at a physiological disadvantage, because those who initiate use of methamphetamine at a younger age also have a greater vulnerability to dependence than men (Dluzen & Liu, 2008).
Women face unique psychosocial barriers that can prevent them from seeking treatment for SA, such as inadequate finances, transportation issues, and caregiver roles and responsibilities (Brady & Ashley, 2005). Pregnancy, caring for children, and anxiety about losing child custody can also discourage or prevent women from entering treatment programs (SAMHSA, 2006). Women are also more susceptible to experiencing stigma (Brady & Ashley, 2005), shame, and embarrassment when seeking treatment for SA (Thom, 1987). Despite the unique attributes of women’s SA issues, the essential features of women-specific SA interventions have not been identified.
Substance Use as Occupation
Occupation refers to “activities of everyday life, named, organized, and given value and meaning by individuals and a culture” (Canadian Association of Occupational Therapists, 1997, p. 34). Historically in the occupational therapy and occupational science literature, occupation is typically associated with health and well-being, without recognition that occupations may be illness producing or risky (Stewart, Fischer, Hirji, & Davis, 2016). Despite negative consequences, the occupation of substance use may provide people with a sense of identity and meaning, as well as social connection and a way to organize their time and daily activities (Helbig & McKay, 2003; Stewart & Fischer, 2015; Wasmuth et al., 2015).
The importance of occupations in relation to substance use was illustrated in a Swedish cross-sectional study that explored the relationship between patterns of everyday occupations and alcohol consumption in women ages 20–55 yr. Women who engaged in leisure activities less frequently and had more spare time were more likely to engage in problematic drinking, a relationship stronger than all other factors including income, marital status, or education (Andersson, Eklund, Sundh, Thundal, & Spak, 2012). A lack of meaningful activities can trigger relapse (Helbig & McKay, 2003), indicating that finding other occupations to engage in after one ceases or decreases substance use may play a role in recovery.
Study Rationale
Although the provision of secondary services, such as child care or transportation services, for women-only programs has been documented, details about the specific characteristics and features of the interventions are limited in the literature, especially as understood from an occupational perspective. We found seven systematic reviews of women-only SA programs, most of which focused on specific populations such as mothers (Niccols, Milligan, Sword, Thabane, & Henderson, 2012), Aboriginal women (Montag, Clapp, Calac, Gorman, & Chambers, 2012), pregnant women (Stade et al., 2009), inmates (Adams, Leukefeld, & Peden, 2008), or those attending court-sanctioned SA treatment (Finfgeld-Connett & Johnson, 2011). Another review searched NIDA’s database for women-only studies from the National Drug Abuse Treatment Clinical Trials Network (Greenfield et al., 2011). More recently, a review of brief interventions for alcohol use was completed, some of which included women-only studies (Gebara, Bhona, Rozani, Lourenço, & Noto, 2013). Although these reviews reported on participants’ success in reaching specific outcomes, none provided a comprehensive review of the characteristics and features of the interventions.
Method
Because a comprehensive understanding of the topic is lacking, we conducted a scoping review, following the five-step method of Arksey and O’Malley (2005), to examine the characteristics and features of women-only SA interventions. The research question was, “What is known from existing North American peer-reviewed literature about the characteristics and features of SA interventions for women?”
Two librarians were consulted to choose the databases and develop a search strategy. Four databases—PubMed, CINAHL, PsycINFO, and Scopus—were chosen on the basis of geography (i.e., North American) and discipline. The search strategy consisted of related terms in three groups: intervention, substance abuse, and women only. English-language articles published from 2001 to 2014 inclusive were included because Health Canada (2001) first published a best practices guideline for treatment and rehabilitation of women with substance use problems in 2001. Articles were included if the majority of the research was completed after 2000, they described women-only North American programming targeting SA, and they provided information on the SA program’s characteristics and features. Studies were excluded if they described an intervention for tobacco cessation or an intervention that was exclusively pharmacological or if they were systematic reviews or secondary analyses. Although systematic reviews were excluded, their reference lists were reviewed, and articles meeting the inclusion and exclusion criteria were added to the identified data sources.
The first two researchers (Leppard and Ramsay) conducted a title and abstract review of the articles they found in the final search of their respective databases, discussing concerns as they arose throughout the process. In addition, peer cross-checking of the first 100 and last 50 articles in each database was completed to ensure that the two researchers were applying the criteria consistently in choosing the final articles. No significant discrepancies were found in the selection of articles across the two researchers; thus, all selected articles were saved in RefWorks (Version 2.0; ProQuest, Bethesda, MD). A full-text review of the remaining articles was completed, resulting in 42 articles that met the criteria for the study, including articles found in the reference lists of 7 systematic reviews.
A data extraction chart containing several initial categories was created with input from all researchers to guide the extraction process. Categories were added, removed, and combined during data extraction in an iterative fashion on the basis of their apparent relevance to the research question, resulting in the following categories: harm reduction and abstinence, intervention type, outcomes measured, and intervention targets. Harm reduction and abstinence are two main organizing philosophies for SA interventions. Harm reduction emphasizes efforts to minimize damage caused by the behavior, incorporating strategies ranging from safer use to managed use to abstinence (Harm Reduction Coalition, n.d.); abstinence aims to eliminate substance use entirely. Alcoholics Anonymous and other 12-step programs are examples of abstinence programs that measure success by consecutive days of abstinence (Lunau, 2014).
To ensure that the researchers were extracting the information from articles reliably, consensus on data extraction was reached through crossover for the first 3 and last 3 articles. For the category of harm reduction and abstinence, the articles reviewed did not state explicitly what broad approach or philosophy was used. Thus, a team consensus was reached to classify articles as abstinence if they described complete stoppage of alcohol or drug use or specifically cited Alcoholics Anonymous or another 12-step program, court-ordered programs, or those with urinalysis. Articles were considered harm reduction if a decrease in use was deemed successful or if there was no evidence of abstinence programs.
After data extraction was complete, the data listed under “intervention targets” were grouped on the basis of similar features, resulting in 13 themes, such as substance use, intrapersonal functioning, health education, skill development, parenting skills, and occupation and productivity. The intrapersonal functioning category consisted of program targets of self-efficacy, readiness to change, self-management, self-esteem, grief or loss, and self-advocacy, and the mental health category consisted of program targets specific to mental health diagnoses such as depression and anxiety.
Data listed under intervention types and outcomes measured were also grouped, although this process was more straightforward and did not involve identification of categories. After collating the data as described, descriptive statistics and frequency counts were used to describe the data sources and characteristics and features of the interventions.
Results
The search resulted in 2,199 articles. Application of the inclusion and exclusion criteria resulted in 31 articles. Seven systematic reviews were also used to identify 11 more studies. This scoping review analyzed 42 articles that discussed 37 different programs. Forty-one of the articles were from the United States, and 1 was from Canada.
Although each study targeted women with SA issues, the specific group of concern varied. Two articles addressed women with trauma symptoms and SA issues, 9 targeted female inmates, and 6 targeted women with SA and another risk factor, such as being a sex worker or living with HIV. Seven studies targeted pregnant women, another 7 targeted mothers, and the remaining 11 targeted women with SA issues alone.
The articles reviewed analyzed programs that occurred in a variety of settings: inpatient programs (n = 13) in locations such as prisons, inpatient rehabilitation facilities, and therapeutic communities; outpatient programs (n = 22), such as online programs and informal brief interventions; and combined inpatient–outpatient programs (n = 7). The majority of articles described programs that used group-based formats (n = 18); 14 articles featured individual treatment sessions only, and 10 articles offered both group and individual sessions. The average attrition rate for the programs studied in the articles was 37% from the beginning of the program to follow-up (range = 0%–80%).
Of the 37 unique programs, 32 used a harm-reduction approach and 5 used an abstinence approach. Substance use (n = 26) was the most common target of the interventions described. However, many of the interventions aimed to decrease participants’ substance use by targeting other areas of their lives that were perceived as contributing to increased use. For example, 16 programs targeted intrapersonal (or internal) functioning, such as self-management skills and readiness to change (see Figure 1 for the targets of interventions). Only 5 of the programs reviewed featured occupational targets for change (i.e., interventions that directly targeted occupations, activities, or tasks). These programs aimed to change activity that “is performed with some consistency and regularity, . . . brings structure, and is given value and meaning by individuals and a culture” (Polatajko et al., 2013, p. 19). Examples of occupational targets are work, education, and exercise.
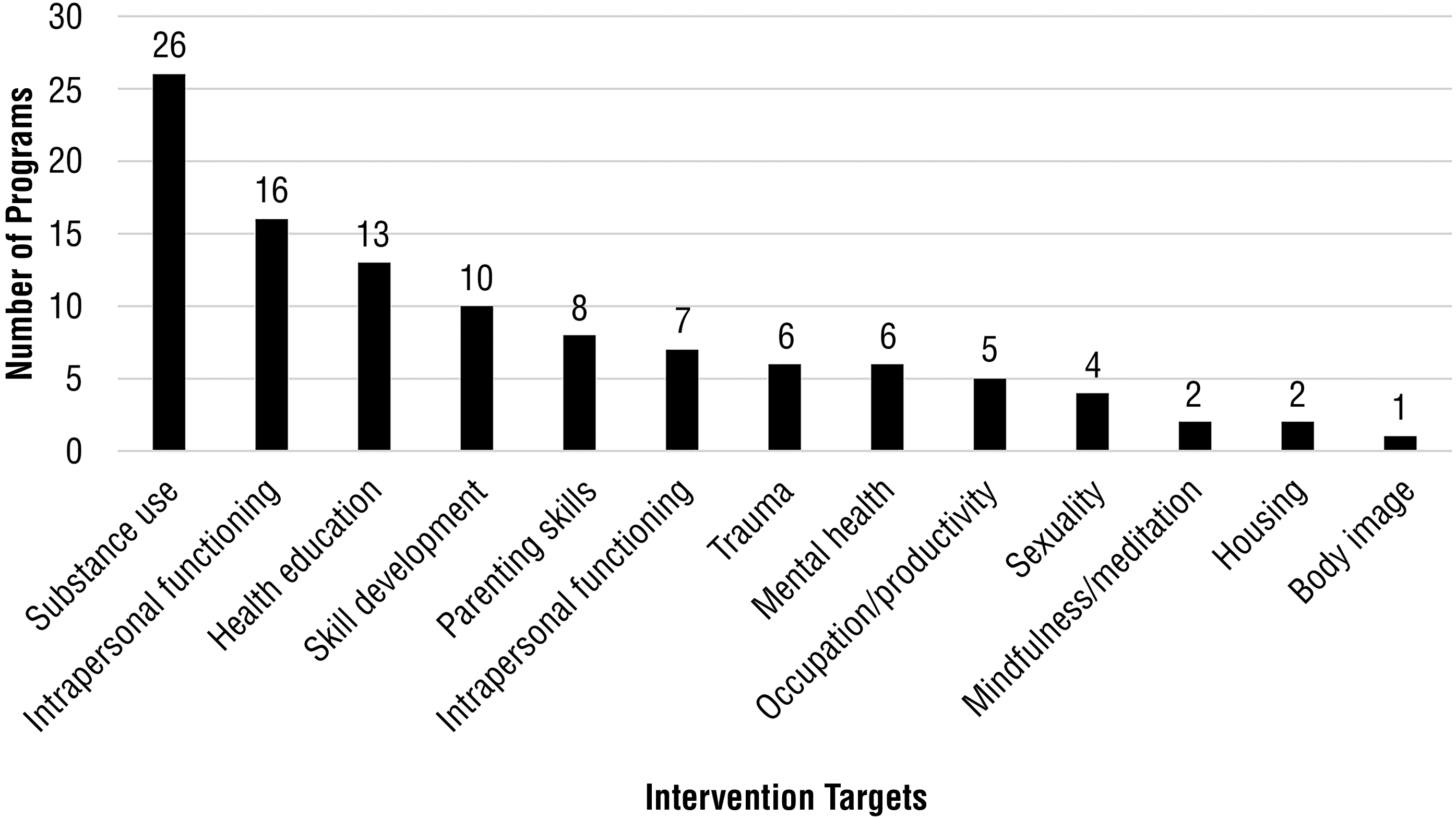
Intervention targets of the programs reviewed.
The majority of programs (25 of 37) used a combination of components in the interventions (Figure 2). The most common program component used was education (n = 18), with topics including education on race and class structures, healthy relationships and sexuality, and triggers for relapse. Motivational interviewing (n = 15), skills-based interventions (including coping skills and social skills; n = 12), cognitive–behavioral therapy (n = 11), and psychotherapy (n = 8) were also popular features of SA interventions.
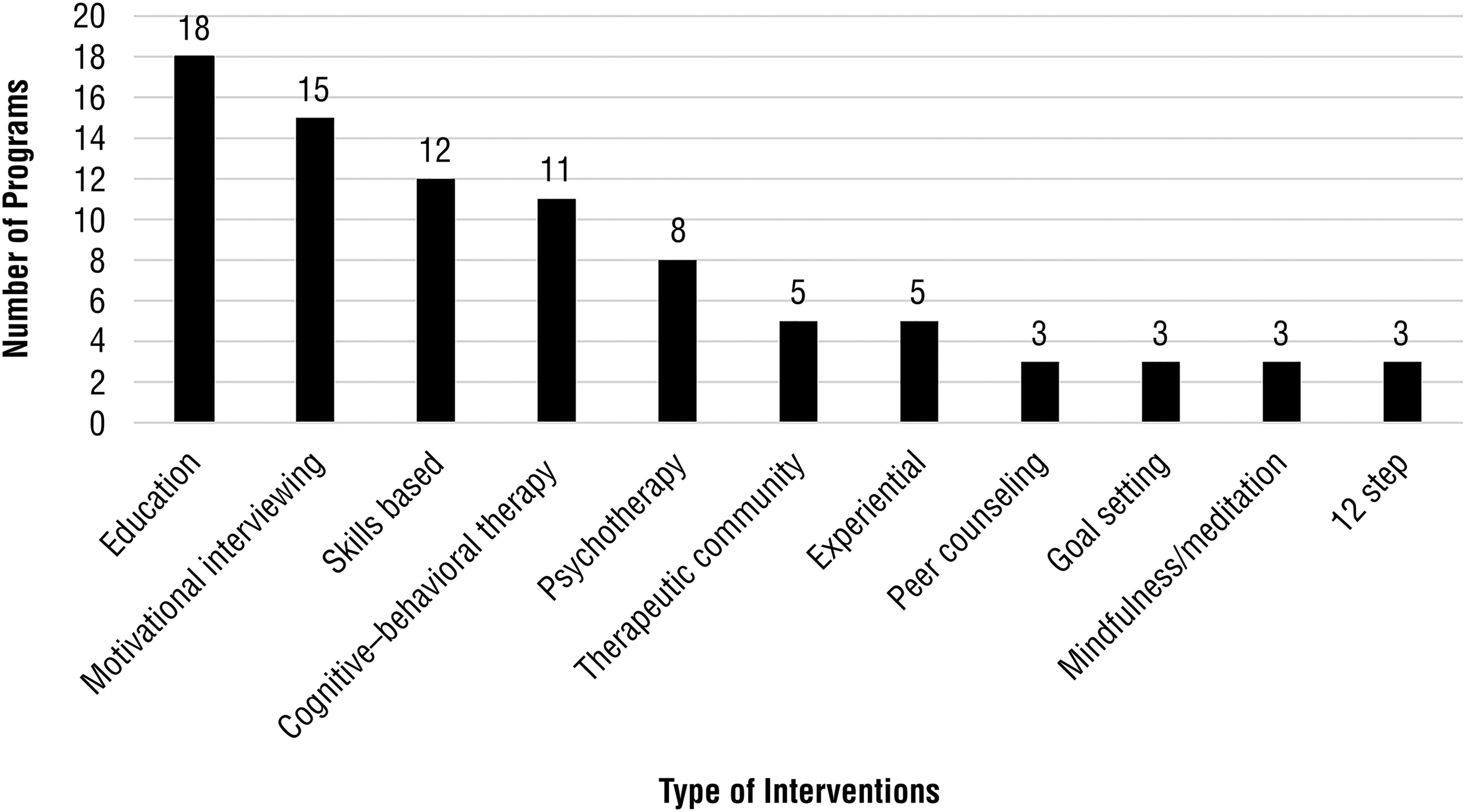
Intervention types in the programs reviewed.
Program effectiveness was measured in the 42 articles by means of a variety of outcome measures, with most articles (n = 33) describing use of more than one outcome measure. The majority of articles looked at the level of reported substance use as an outcome, with 31 articles using a self-report measure and 5 using urinalysis to determine whether participants had recently used substances. Many studies also measured the frequency and extent of mental health symptoms (n = 18), such as depression and anxiety, and trauma symptoms (posttraumatic stress disorder; n = 9). Six studies measured occupation and productivity (school or work engagement) as outcomes (Figure 3).
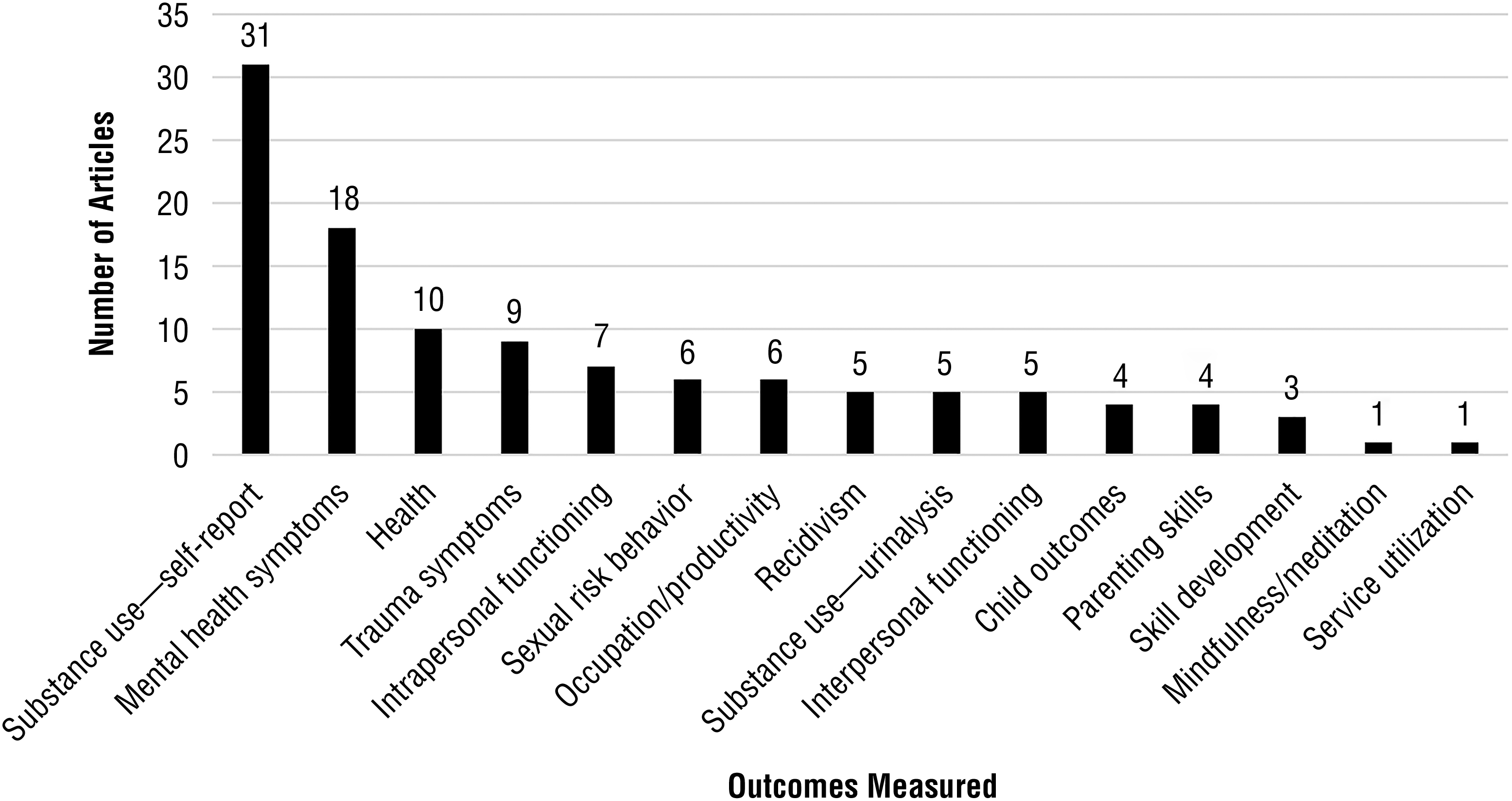
Outcomes measured in the articles reviewed.
Discussion
The findings of this study suggest, first, that programs have multiple targets for change and, second, that the majority of programs use a harm-reduction approach. The multifaceted nature of the interventions identified in this scoping review reflects a trend in contemporary intervention programs. Factors associated with SA, such as trauma, housing, and economic issues, have historically been neglected in SA treatment (Stewart, 2007). Services were fragmented, and clients had to attend multiple treatments for the different issues they were experiencing. Only since the 1990s has a more integrated treatment approach emerged (Stewart, 2007).
Although analysis of study outcomes was beyond the scope of this review, Stewart (2007) and Pinkham, Stoicescu, and Myers (2012) suggested that multifaceted interventions lead to better outcomes. Pinkham et al. emphasized the importance of addressing employment, housing, relationship dynamics, and needs related to children. Few programs in this review had occupational or productivity targets, such as restoring old or engaging in new occupations or promoting formal education, employment, or exercise. This is concerning because research has illustrated the relationship between a lack of leisure activities and an increased level of free time with problematic drinking (Andersson et al., 2012). Further investigation is warranted into how targeting one’s occupational repertoire with previously performed or new health-promoting occupations, roles, and meaningful and satisfying ways to spend time can play a role in a multidisciplinary approach to promote recovery from SA.
The majority of the 37 programs used a harm-reduction approach. This approach has been promoted as a client-centered approach because it seeks to “meet the individual where . . . she is at” (Marlatt & Witkiewitz, 2002, p. 867). First identified in the 1980s, this approach offers an alternative to abstinence approaches, which exclude people who are interested in reducing—but not completely abstaining from—substance use (Bonomo & Bowes, 2001). Harm reduction is used to describe a number of policies, programs, and practices such as needle distribution programs and supervised injection sites (HealthLink BC, 2015), as well as housing-first initiatives (Collins et al., 2012). Harm-reduction approaches measure social and economic as well as health outcomes and not merely presence or absence of substance use (Bellis, Hughes, & Lowey, 2002), which was consistent with some of the outcome measures found in this review, including child outcomes, sexual risk behavior, mental health symptoms, and overall health. This is promising because harm-reduction activities have been shown to decrease the transmission of hepatitis and HIV, decrease crime, increase employment, and increase referrals to treatment programs and health services (HealthLink BC, 2015).
Study Limitations and Acknowledgment of Biases
Critically appraising the evidence found in the 42 identified articles was beyond the scope of this review. Many of the studies targeted multiple outcomes using a variety of measures of success, so comparison of the measures was not possible. Although the majority of the studies reported moderate successes in some outcomes measured, we cannot comment on the rigor and congruence between outcomes measured and improvement in functioning levels and changes in addictive behavior.
Because of our background, we used a specific occupational perspective (Njelesani, Tang, Jonsson, & Polatajko, 2014) as the foundation for making sense of the features and characteristics of these SA programs. The goal in categorizing the data extracted from the literature was to remain as descriptive as possible; however, with all research, that requires a consensus-building process, and other researchers may have organized the data differently. Attempts were made to be transparent about the purpose and process of data collection, categorization, and presentation.
This research was limited because we reviewed only English-language articles. Inclusion of French- and Spanish-language articles would have provided a more accurate description of the interventions used for women in SA treatment in North America.
Future Research
A complete review of the North American gray literature and the stakeholder information on programs will help to expand this study’s findings and further inform researchers of the characteristics and features of women-only SA treatment programs and the gaps that exist between research and practice. Further research to compare the effectiveness of SA treatment programs focused on performance component skills with programs that have broader functional or occupational goals, such as employment, education, and leisure, will provide clinicians with more insight to guide program development. In addition, research on the effectiveness of SA treatment programs that target the client’s occupational repertoire, alone and in combination with other modalities, is needed.
Implications for Occupational Therapy Practice
The findings of this study indicate that there is an emerging but limited volume of literature describing the characteristics and features of women-only SA interventions and programs. Of the articles that were analyzed, few described programs that target occupational engagement in health-promoting occupations. These findings have the following implications for occupation-based practice:
The limited literature on this topic may hinder practitioners’ efforts to base their practice on evidence.
Little is known about the outcomes of SA programs that target occupational engagement in comparison with or in addition to other treatment modalities.
Occupational therapists should determine the efficacy of interventions that target occupation and productivity in SA treatment.
Conclusion
This scoping review describes the current trends in women-only SA treatment programs in North America. Most programs emphasized harm-reduction approaches that target multiple areas through education, psychotherapy, and development of component skills in vulnerable populations. Few interventions targeted increasing or improving clients’ occupational repertoires by finding other ways to fill time meaningfully. Engaging in new occupations may help women develop new roles and interests and can play an important role in their recovery and prevention of future relapse.
Footnotes
Acknowledgments
The findings of this study were presented at the Canadian Association of Occupational Therapists Conference, Winnipeg, Manitoba, Canada, on May 28, 2015.