
Abstract
Patients with Duchenne muscular dystrophy in their second decade of life present with decreased upper extremity strength and active range of motion (AROM) that limit activities of daily living (ADLs). We evaluated the ability of the Wilmington Robotic Exoskeleton (WREX) to improve AROM and independence with ADLs. A retrospective chart review of 9 patients who trialed the WREX was performed. Patients were classified on the basis of the Brooke Upper Extremity Scale. AROM, strength, and independence with ADLs were assessed before and after a WREX trial. Patients demonstrated increased shoulder flexion and abduction (25°–100°, median = 55°) and elbow flexion (10°–110°, median = 60°). Increased independence with self-feeding, item retrieval, use of phones and tablets, and facial grooming were noted. The WREX allowed for gravity-reduced movement via elastic bands to unweight the upper extremity, enabling increased upper extremity active movement that supported increased independence with ADLs.
Duchenne muscular dystrophy (DMD) is a genetically based, rapidly progressive muscular dystrophy that begins in childhood, primarily affecting proximal upper and lower extremity muscular function. The disease progresses in a proximal to distal manner, initially with loss of active movement and muscle atrophy, fibrous fatty tissue replacement, and eventually contracture of the joints and inability to functionally use the arms. Activity limitations of the upper extremity occur early in the ambulatory phase and increase in the advanced stages of the disease (Janssen, Bergsma, Geurts, & de Groot, 2014).
In the second decade of life, patients with DMD often require power mobility in the home and community. As the disease progresses and upper extremity strength declines, there is a continual decrease in activity of daily living (ADL) independence (Fujiwara et al., 2009) and limited opportunities for education and employment (Maireese & Šteinbuka, 2009). The distal musculature is best preserved, relatively sparing the wrist and hand muscles until late in the disease process (Wagner, Vignos, Carlozzi, & Hull, 1993), leaving hand function grossly intact. These skills, however, are unable to be fully used for completion of ADLs because of proximal impairments.
Children rely on the use of compensatory movement patterns, posturing, and environmental modifications to preserve ADL independence. Often, children use momentum to swing the arm forward to complete tasks; however, this is an ineffective movement pattern because motor control is poor, and the child is unable to sustain the arm in space for proper task completion. Compensatory strategies for bringing the hand to the mouth for feeding and personal care include flexed posturing; bending forward at the trunk; and flexing the neck to bring the head closer to the table for self-feeding, facial grooming, or putting on or taking off eyeglasses. This method can help temporarily; however, it is unsustainable because of disease progression and is frequently negated by the necessity of a spinal fusion. Children also use lever arms to bring their hand to their face by resting one arm over the other and using it as a fulcrum. Finally, the use of an elevated table or surface can support the arm for gravity-reduced movement at the elbow joint for self-feeding or moving the hand to access technology. These adaptations, however, are often limited to the home and are not easily transferable to the community.
Mobile arm supports (MASs) were initially used in the 1950s for people with polio and soldiers who sustained upper extremity injuries. Traditional counterbalance MASs provide support at the forearm and the ability to move the elbow joint in a gravity-eliminated plane, or to shift the weight of the arm posteriorly on the fulcrum to elevate the hand against gravity to improve ADL function (Kumar & Phillips, 2013). However, the traditional MAS is limited in its utility for patients with progressive neuromuscular disorders because it has limited degrees of freedom and does not provide active assistance to support movement with disease progression.
Because of advances in technology, many exoskeletons are currently available on the market. The ARMin III (Swiss Federal Institute of Technology Zurich, Zurich, Switzerland), MGA (Georgetown University Medical Center, Washington, DC, and University of Maryland, College Park), and IntelliArm (Rehabtek, Chicago) are motor-powered exoskeletons used for upper extremity rehabilitation after stroke, and they all have shown efficacy (Lo & Xie, 2012); however, these units are very expensive, high-profile, nonportable exoskeletons that are designed for use in the hospital or rehabilitation setting, and they cannot be used continuously throughout the day in the home and community setting. Additionally, electromyography sensors in units such as the mPower arm brace (Myomo Inc., Cambridge, MA) accentuate elbow flexion and extension movements based off muscle activity, but they are limited to 1 degree of freedom. The purpose of this study is to evaluate the efficacy of a low-profile, portable, wheelchair-mounted, gravity-reducing exoskeleton designed for use in the home and community that provides three-dimensional movement of the upper extremity to (1) improve active range of motion (AROM) of the upper extremity and (2) improve ADL performance for patients with DMD.
Materials and Method
Wilmington Robotic Exoskeleton
The Wilmington Robotic Exoskeleton (WREX; Jaeco Orthopedics, Hot Springs, AZ) is a lightweight, passive, gravity-balanced exoskeleton arm orthosis (Rahman et al., 2006, 2007; Rahman, Sample, Seliktar, Alexander, & Scavina, 2000). It consists of four main components: forearm component, elbow joint with 2 degrees of freedom, upper arm component, and shoulder joint with 2 degrees of freedom. The WREX uses elastic-band elevation assists for both the shoulder and elbow to allow a person to move his or her arm with little effort. The bands provide a counterforce to gravity and allow the arm to attain balance in a static position and to move freely in three-dimensional space.
The WREX attaches to the wheelchair posterior to the shoulder. The axis of rotation for shoulder horizontal abduction and adduction resides above the shoulder joint that has a fixed relationship to a parallel axis lateral to the shoulder to allow scapular protraction and retraction. The humeral and radial components are arranged parallel to the upper and lower arm, with a trough to support the forearm. These components are a four-bar link design, essentially a parallelogram with articulating corners. This linkage allows flexion of the shoulder and elbow joints to be assisted by the addition of an elastic band.
The 4 degrees of freedom acquired from the joints allow positioning of the arm and hand in three-dimensional space. Gravity is eliminated by two sets of rubber bands that oppose the effect of downward motion of the upper arm and the forearm. These bands, with different levels of elasticity, are selected and adjusted to unweight the arm and to assist in moving against gravity.
Patient Selection and Classification
We reviewed 9 patients with DMD who completed a trial of the WREX as part of their multidisciplinary (i.e., neurology, occupational therapy, physical therapy, genetics, nursing, social work) neuromuscular program consultative visit from February 2012 to March 2013 (Table 1). Level of impairment was classified with the Brooke Upper Extremity Scale, a brief observation-based, 6-point scale that allows for classification of upper extremity function for DMD (Brooke et al., 1983). Inclusion criteria for a WREX trial in the clinical setting were a confirmed diagnosis of DMD; Brooke Upper Extremity Scale score of 2, 3, 4, or 5; and wheelchair dependence. Exclusion criteria were a Brooke Upper Extremity Scale score of 1 or 6, ambulatory functionality, cognitive impairments that would limit use of the WREX, and non-English speaking. Approval from the institutional review board was received, and a consent exemption was granted.
Patient Characteristics and Strength
Note. MMT = manual muscle testing.
Assessments
Initial assessment included AROM, strength testing, and ADLs. Goniometry was completed to assess active shoulder flexion, abduction, and elbow flexion AROM. Hand-held myometry (Beenakker, van der Hoeven, Fock, & Maurits, 2001; Florence et al., 1992) and manual muscle testing (MMT) were used to quantify strength of the shoulder flexors, abductors, elbow flexors, and extensors (Table 1). Functional tasks such as eating, drinking, simulated facial grooming, and item retrieval were assessed as part of the clinic evaluation. The patients were positioned in their power wheelchair with a height-adjustable table placed at arm rest height. The level of independence and use of compensatory techniques were documented. After donning of the WREX, AROM and ADL completion were immediately reassessed by the same clinician.
Evaluation Method
After initial data were collected, within the same visit, the WREX was mounted to the wheelchair, adjusted to fit the patient, and balanced to meet the patient’s unique needs. After the WREX was set to allow for the ability to elevate the arm at the shoulder and elbow joints and to bring the arm back down to the starting position, AROM measurements and ADL tasks were reassessed.
Data Analysis
The normality of the data was evaluated, and the levels of skewedness and kurtosis were assessed. Because of a nonnormal distribution, it was necessary to complete a Wilcoxon signed-rank test to compare pre- and postmeasurements for all ROM outcomes.
Results
All patients demonstrated increased AROM at the shoulder and elbow joints (Table 2) with WREX donned. Shoulder flexion increased by a median of 55° (25°–100°; p = .008), whereas shoulder abduction increased by a median of 60° (25°–100°; p = .008). Elbow flexion increased by a median of 60° (10°–110°; p = .008). Increased ADL performance was observed in self-feeding (9/9 patients; Figure 1) and drinking from a cup without straw (5/9 patients); patients were unable to bring food or a cup to their mouths without use of the WREX. When using the WREX, all 9 patients could access the wheelchair joystick; reach away from the body to retrieve items in the environment (Figure 1); and sustain the arm in space to use technology such as tablets, keyboards, and cell phones. Previously, all 9 patients were dependent on another person to retrieve objects or position the arm for them.
ROM Improvements With the WREX
Note. AROM = active range of motion; ROM = range of motion; WREX = Wilmington Robotic Exoskeleton.
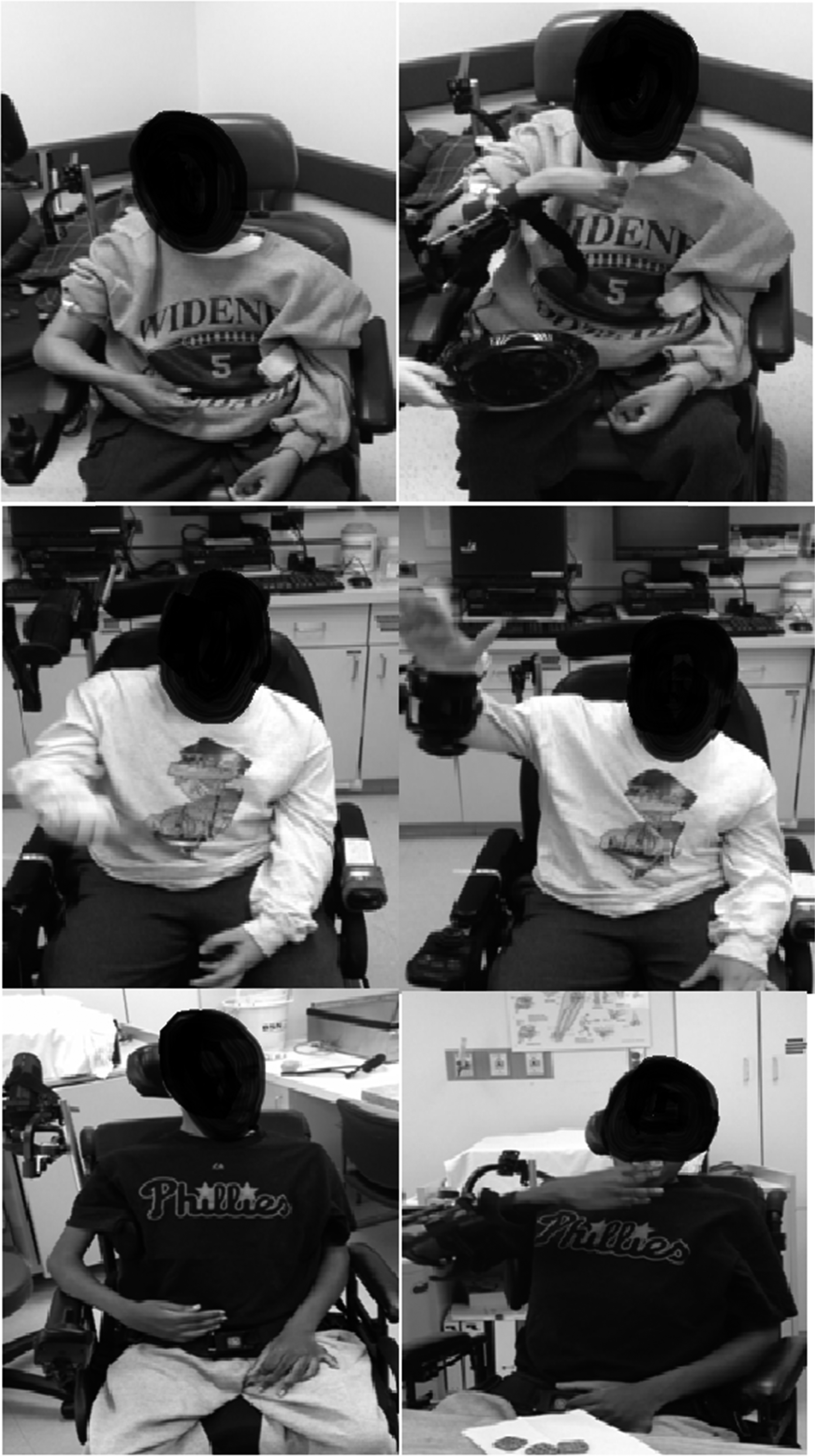
Improved ability to self-feed and reach away from body with the Wilmington Robotic Exoskeleton.
Discussion
Previous literature supports the use of MASs in the neuromuscular population to improve AROM and independence with ADLs (Kumar & Phillips, 2013; Mastenbroek, de Haan, van den Berg, & Herder, 2007; Rahman et al., 2007). However, there are significant limitations with traditional ball bearing and counterbalance arm supports. The patient must demonstrate sufficient (2+ MMT) strength to use the device (Yasuda, Bowman, & Hsu, 1986), and the MAS only allows for single-plane movement. Because of these limitations, traditional MASs are only effective in a small percentage of patients for a limited time. The WREX, however, allows for titration of the degree of assistance provided to accommodate disease progression, allowing a longer window of usage, and it has been shown to improve upper extremity performance on standardized evaluations in patients with neuromuscular disease (Rahman et al., 2000).
We investigated the ability of the WREX to increase AROM and to improve performance in ADLs. The WREX significantly (p = .008) increased AROM for 9 patients with DMD with little to no proximal shoulder and elbow movement by reducing the effect of gravity on movement. With the WREX, patients could reach outside their base of support, overhead, across their body, and to the face. This increased AROM and ability to sustain the arm in space may have led to observed improvements in independence in completion of ADLs. Several patients could feed themselves for the first time in years, complete facial grooming, and take off and put on glasses; moreover, all the patients were able to access a larger functional workspace for item retrieval and accessing technology devices. The WREX also provides a safety benefit because it assists with access to the child’s cellular phone for use in emergencies and provides the ability to reposition the hand on the joystick when it falls, thus improving independent function.
Aquatic therapy and ergometry have been used as interventions for strengthening and maintaining range of motion in the neuromuscular population (Alemdaroğlu, Karaduman, Yilmaz, & Topaloğlu, 2015) because they provide a reduced-gravity environment allowing for ease of movement. Similarly, the WREX supports gravity-reduced upper limb movement, allowing the child to use his or her residual strength and AROM.
Two potential barriers to use of the WREX are decreased muscle strength and the tendency to use compensatory motor strategies. The tension provided to elevate the arm also provides a resistive force for the antagonist muscle groups to overcome as the arm is brought back down. If the patient does not have sufficient latissimus dorsi or triceps strength to overcome the tension, the arm floats in space. The degree of tension must be carefully adjusted to allow for increased flexion while still allowing for extension of the arm back to the wheelchair joystick. This could possibly explain the wide variability (25°–100° of shoulder flexion and abduction and 10°–110° of elbow flexion) in gains of AROM noted with the WREX because the patients’ strength determined their ability to overcome the dynamic assistance provided for shoulder and elbow flexion to ensure that they could return the arm to the joystick. Note that for all patients in this sample, the triceps had equal or greater strength than the biceps (the muscle group that received the active assistance). Testing of the shoulder adductors and extensors was not completed, so we cannot verify that this relationship is consistent throughout the upper extremity. Further exploration is needed to better understand the relationship between agonist and antagonist strength ratios.
Secondarily, there appears to be a learning curve to using the device because of potentially prolonged disuse in the muscle groups that are being activated or a history of the use of those muscles only in compensatory movement patterns. The WREX, being an exoskeleton, works best when it is close to the arm with the axis of the device aligned with the joint axis; if the child moves away from the wheelchair or the device, the alignment of the axes is altered, diminishing effectiveness. It also appears that movements such as diagonal patterns that require synergistic muscle function are more complicated and require additional practice. The most effective method for teaching use of the WREX appears to be working on single-plane movements one joint at a time to gain motor control. For example, self-feeding requires shoulder flexion to elevate the arm, horizontal adduction to midline, and elbow flexion and forearm supination to bring the hand to the mouth. After these isolated movements are mastered, patients can be progressed toward a single fluid movement trajectory toward the mouth for self-feeding.
We acknowledge the small sample size and that our group does not represent all patients with DMD. Limitations in our case series include lack of standardized functional measures to evaluate improvement as a result of the increased AROM and the inability to evaluate the sustained performance and frequency of use in the home and community because the children only trialed the WREX at their clinic visits.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
The WREX provides an opportunity for exercising the arm and can improve active upper extremity movement for patients with neuromuscular disease.
The WREX can improve independence in ADLs.
Patients with decreased upper extremity range of motion and intact distal hand function are potential candidates for the WREX.
Conclusion
We have described 9 pediatric patients with significant upper extremity functional limitations because of DMD who benefited from the WREX to improve independence with ADLs. The WREX allows for increased ease of antigravity movement, significantly improved AROM at the shoulder (p = .008) and elbow joints (p = .008), and improved functional workspace and ability to sustain the arm in space for increased independence in ADLs. Further research is needed in a larger, more diverse patient population with a comparison control group to further validate the efficacy of the WREX. Future research should include the use of diagnosis-specific measures (e.g., a revised upper limb module for spinal muscular atrophy and a performance upper limb measure for Duchenne muscular dystrophy) and an ordinal ADL scale. In addition, research is needed to identify clinical measures that predict successful performance with the WREX to allow clinicians to appropriately evaluate and recommend the WREX for patients with neuromuscular diseases. Finally, a longitudinal study is necessary to evaluate the WREX’s ability to help preserve muscle strength and AROM for better upper extremity function into adulthood. A prospective clinical trial of the WREX, on the basis of these findings and addressing the aforementioned limitations, has been submitted for institutional review board approval.
Footnotes
Acknowledgment
The authors thank Cure SMA for their support in the publication of this research.