
Abstract
Studies have suggested that customized lighting can improve the function of people with visual deficits in the home setting (Brunnström, Sörensen, Alsterstad, & Sjöstrand, 2004; Liu, Brost, Horton, Kenyon, & Mears, 2013). In addition, research involving home lighting has suggested that function can be impeded by a lack of luminance (Perlmutter et al., 2013). Although this research has demonstrated the efficacy of changing the home environment for people with low vision, the evidence is limited for use of those same techniques during the acute rehabilitation stage after a cerebrovascular accident (CVA) in an inpatient rehabilitation facility (IRF; Grider, Yuen, Vogtle, & Warren, 2014). The need to address visual disturbances after CVA was emphasized by a recent study specific to the IRF setting that reported that 33% of all patients admitted had at least one area of visual concern that interfered with activity of daily living (ADL) performance (Grider et al., 2014). This same study reported that 55% of patients diagnosed with a CVA demonstrated visual concerns. The high incidence of visual concerns affecting patients with CVA in an IRF leads one to question whether function would improve using the same interventions, increased illumination and light source positioning, that have been used in other settings.
Visual disturbances are common after a CVA. A study of 326 persons with CVA showed that 68% had eye alignment or movement impairment, 49% had visual field impairment, 27% had low vision, and 21% had perceptual difficulties (Rowe et al., 2009). These visual deficits interfere with ADL performance and independence (Grider et al., 2014). However, occupational therapists and other inpatient interdisciplinary team members do not routinely screen for visual impairments (Roche, Vogtle, Warren, & O’Connor, 2014). These professionals should consider clients’ visual function in inpatient settings to improve the efficacy of their treatment interventions (Cimarolli, Morse, Horowitz, & Reinhardt, 2012).
The purpose of this article was to explore the effects of enhanced lighting on the function of people with an acquired visual deficit resulting from CVA in an IRF. We did not explore the difference between types of light sources, only the amount of light available to the client as measured by a light meter.
Method
This article describes two cases using a short-term intervention to assess how lighting changes affect clients’ grooming performance in an IRF. The FIM® (Uniform Data System for Medical Rehabilitation, 1997) was used for assessment purposes. The FIM defines the grooming category as oral care, hair grooming, washing and drying the hands, washing and drying the face, and either shaving or applying makeup. An ABAB design was used: an evaluation of the grooming task without an intervention (A1), the grooming task with an intervention (B1), another grooming task without an intervention (A2), and finally the grooming task with the intervention present once again (B2). The data were graphed for preintervention, postintervention, and between-cases comparisons. All assessments and interventions took place in participants’ rooms at Eastern Idaho Regional Medical Center. We obtained approval from the institutional review board at Eastern Idaho Regional Medical Center for this study and obtained informed consent from the participants.
Participants
Participants were recruited from Eastern Idaho Regional Medical Center. The sample was recruited from among patients being considered for admission to an IRF. Inclusion criteria consisted of (1) a diagnosis of stroke or traumatic brain injury with a visual deficit that was determined by means of specific subtests of the Brain Injury Visual Assessment Battery for Adults (biVABA; Warren, 1998) and (2) the ability to communicate sufficiently to convey preference concerning lighting. The question of being able to sufficiently communicate with the evaluator was ascertained by means of interactions with the client during the screening process and results of the Short Portable Mental Status Questionnaire (SPMSQ; Pfeiffer, 1975). Five individuals with CVA were screened for possible inclusion in the study; 2 met the inclusion criteria.
Measures
The FIM is the most common tool used in IRFs to assess client performance of ADLs (Ottenbacher, Hsu, Granger, & Fiedler, 1996). One of the FIM categories is grooming. The task of grooming was selected for this project because of the need for interaction between the environment and the visual, physical, and cognitive aspects of the task to complete it. Grooming was also selected because it requires a workstation at which the tools and lighting conditions can be reproduced and adjusted from day to day with simple equipment.
Intervention
For this study, we used illumination tools that are affordable and available for purchase to reproduce the results. Studies have suggested that people with low vision may prefer halogen light bulbs (Holton, Christiansen, Albeck, & Johnsen, 2011), but the amount of light may be more important than the type of light bulb (Eperjesi, Maiz-Fernandez, & Bartlett, 2007). We focused on the variable of how much light was available to the patient (measured in lux by a light meter) and the positioning of the lighting for the participant’s needs. Lux is a standard measure of illuminance, defined as the amount of light from a uniform source on a surface 1 m in radius (Merriam-Webster, n.d.). We used a GE Reveal 100-W halogen light bulb (General Electric, Boston) that is readily available. A dimmer was used to adjust the amount of light to meet each participant’s needs (Lutron TT-300H-WH Electronics plug-in lamp dimmer [Lutron, Coopersburg, PA] or a GE 55431 indoor light-socket dimmer with light-level control knob). A light meter was used to measure the luminance of the work area (HDE LX-1010B digital Luxmeter light meter with LCD display [HDE, Allentown, PA], range ≤ 50,000 lux).
Light positioning was accomplished by means of a lamp that provided improved ambient lighting and task-lighting options (Home Design 150-W floor lamp with side reading light; Décor Works, Mandeville, LA). We used a light boom when the participant required an improved overhead light source (LimoStudio AGG809 photo video studio overhead hair boom light stand, 86 in. tall and 74.5 in. extended; LimoStudio, Rancho Cucamonga, CA). The light boom is not a usual therapy item, but in this case it was useful because the grooming station did not have a light over the mirror, and it provided an inexpensive option for determining whether structural changes would be valuable.
Procedure
An occupational therapist assessed grooming and performed lighting adjustments. The participant was seated at the sink in his or her room each day at 7:00 a.m., which meant that there was no day-to-day sunlight variation because it was still dark at that time of year. In both cases, the grooming tools were placed on a table on the side of the client’s visual inattention to evaluate the effect of the lighting during the visual search phase of the task. During the initial evaluation, available room lighting was used during grooming assessment as outlined by the FIM guidelines. Individual grooming tasks were timed on each of the 4 days. A light meter was used to measure the luminance of the work area each day. The light meter was held at chest level over the sink, which was directly in front of the participant.
On the second day, the client performed the same grooming task with the lighting adjusted and positioned to the client’s preference using the items as noted in the “Intervention” section. The light boom was positioned to provide light directly over the sink. A floor lamp with two light sources, one providing ambient lighting and the second adjustable task lighting, was positioned on the side of inattention to provide extra light in the area of the sink and table with the grooming tools. The amount of light began at the lowest level and increased slowly until the patient requested that it stop. After a short adjustment period, the light was again increased until the patient requested that it stop. This process continued until the patient indicated that the light was at his or her preferred level. On the third day, the grooming tasks were performed again using only the standard room lighting. On the fourth day, the grooming tasks were carried out again, with the lighting adaptations adjusted for the client’s preference by means of the same process as on Day 2. Comments made by participants during the task that related to the lighting were recorded.
Data Analysis
Analysis consisted of comparing scores on the grooming section of the FIM, time taken for each grooming task, and light meter readings for each participant. The time taken for each grooming task was analyzed as a percentage of the time it took to perform the task on Day 1.
Results
Participant A
Participant A was a 68-yr-old woman who had a CVA in the bilateral posterior cerebral arteries during a revision of an aortic valve replacement. She was diagnosed with cortical visual impairment. During the visual screening, she could identify how many fingers were being held up in a range of 10°–30° in the left visual field. In this range, she could track objects and see shapes, but awareness of the orientation of the shape, what the object was, and its relationship to her position was impaired. She would turn her head to the left when asked but would not turn her head past midline to the right side. She was unable to perform any of the biVABA subtests except the scan board, on which she could identify only the numbers 1 and 5. Motor function was intact. Her memory was severely impaired, and she did not have carryover of learning from one session to another. Although her SPMSQ score was 2 of 10, she was able to verbally communicate her immediate needs and preferences accurately during the evaluation process. She had previously been independent in all of her daily occupations and used reading glasses for fine print with no other visual deficits or diagnosis.
Day 1.
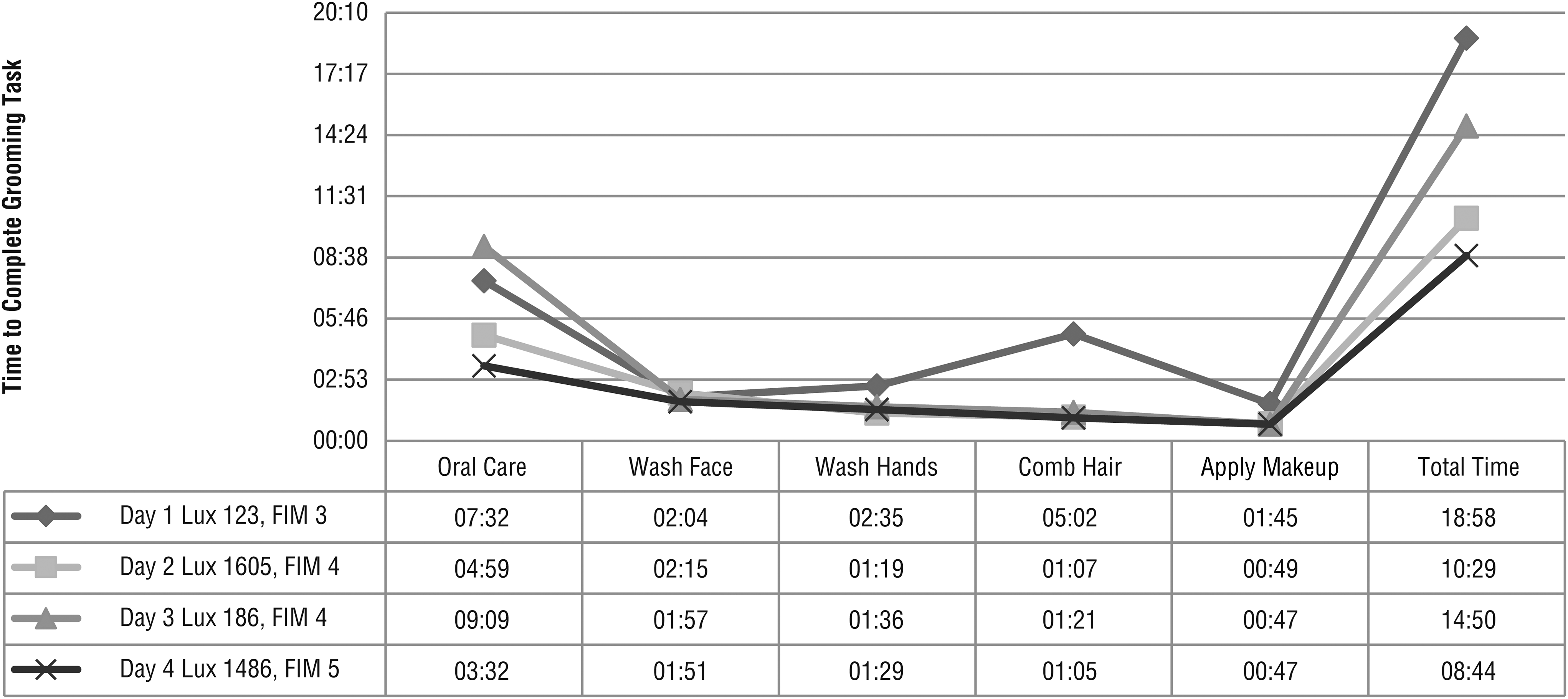
The participant was seated in a standard armchair at the sink with all grooming items placed on a table to the right side of the sink. The grooming items included a toothbrush, toothpaste, rinse cup, washcloth, hairbrush, and lip balm. The soap dispenser was in a permanent position attached to the wall on her left side. This configuration was used all 4 days. The standard room lighting consisted of a fluorescent light mounted on the ceiling and positioned 2 ft behind her chair and another fluorescent light that did not have a direct line of sight to her grooming station but provided some ambient light. She was unable to locate the grooming items and was unable to scan to the right. Hand-over-hand assistance coupled with verbal cues was needed to retrieve each item. The participant required a physical cue to apply toothpaste to the toothbrush, but she was able to physically brush her teeth with cues for thoroughness. Each part of the task was timed (Figure 1). The total time for completion of all grooming tasks on Day 1 was 18:58 min with 123 lux of light luminance, and her FIM score was 3.
Participant A’s results.
Day 2.
Additional supplemental lighting, which included an overhead light and a floor light with an attached adjustable reading light, was positioned to Participant A’s preferred right side, with the adjustable reading light positioned over her right shoulder, illuminating the sink and the grooming items on the table. Participant A was initially skeptical that increased lighting would be helpful. The amount of brightness was slowly increased to her preference using the dimmer function. The light was increased to the highest level of intensity available, and the participant was comfortable. With the increased light on the right as a cue, she was able to turn her head toward the table slightly and examine it. She was able to locate approximately half of the items with verbal cues only; the other items required physical cues to guide her hand. The total time for Day 2 was 10:29 min with 1,605 lux of light luminance, and her FIM score was 4 (Figure 1).
Day 3.
The standard room lighting was on, and the participant asked for more light, similar to the previous day. Up to this point, the participant had not demonstrated carryover of learning from day to day. The participant would not proceed with the grooming task until the occupational therapist turned on a light in addition to the standard overhead lights. In response to her request, a fluorescent light positioned on the wall above the head of her bed that shone downward was added. This light provided minimally more light than on the Day 1 trial (123–186 lux) but satisfied her request for more lighting, and the grooming process began.
It was notable that she did not demonstrate carryover of memory from one day to the next in any other instance during her IRF stay besides this event, in which she was provided additional light for the task of grooming. Although this meant the protocol was not followed exactly on this day, it helped the participant to engage with only a minimal light difference from Day 1 to Day 3 without an emotional disruption that could have changed the evaluation process. Day 3 results were total time of 14:50 min with 186 lux of light luminance, and the participant’s FIM score was 4 (Figure 1). On this day, she was able to find her grooming items with primarily verbal cues and an occasional physical cue.
Day 4.
The enhanced lighting was again provided, and Participant A was able to independently initiate some head movement past midline to the right to find her grooming tools with moderate verbal cuing. Her total time was 8:44 min with 1,486 lux of light luminance, and her FIM score was 5 (Figure 1).
Participant B
Participant B was a 57-yr-old man who sustained a right middle cerebral artery CVA. During screening, he presented with left visual field inattention, poor awareness of his deficits, and left flaccid hemiparesis. During the biVABA, he identified all numbers to the right of midline and none to the left on the scan board and letter-search activities. He would not track or turn his head to the left past midline, even with verbal cues. He had previously been independent in all of his daily occupations and used reading glasses for small print. He demonstrated the ability to communicate effectively, and his SPMSQ score was 8 of 10.
Day 1.
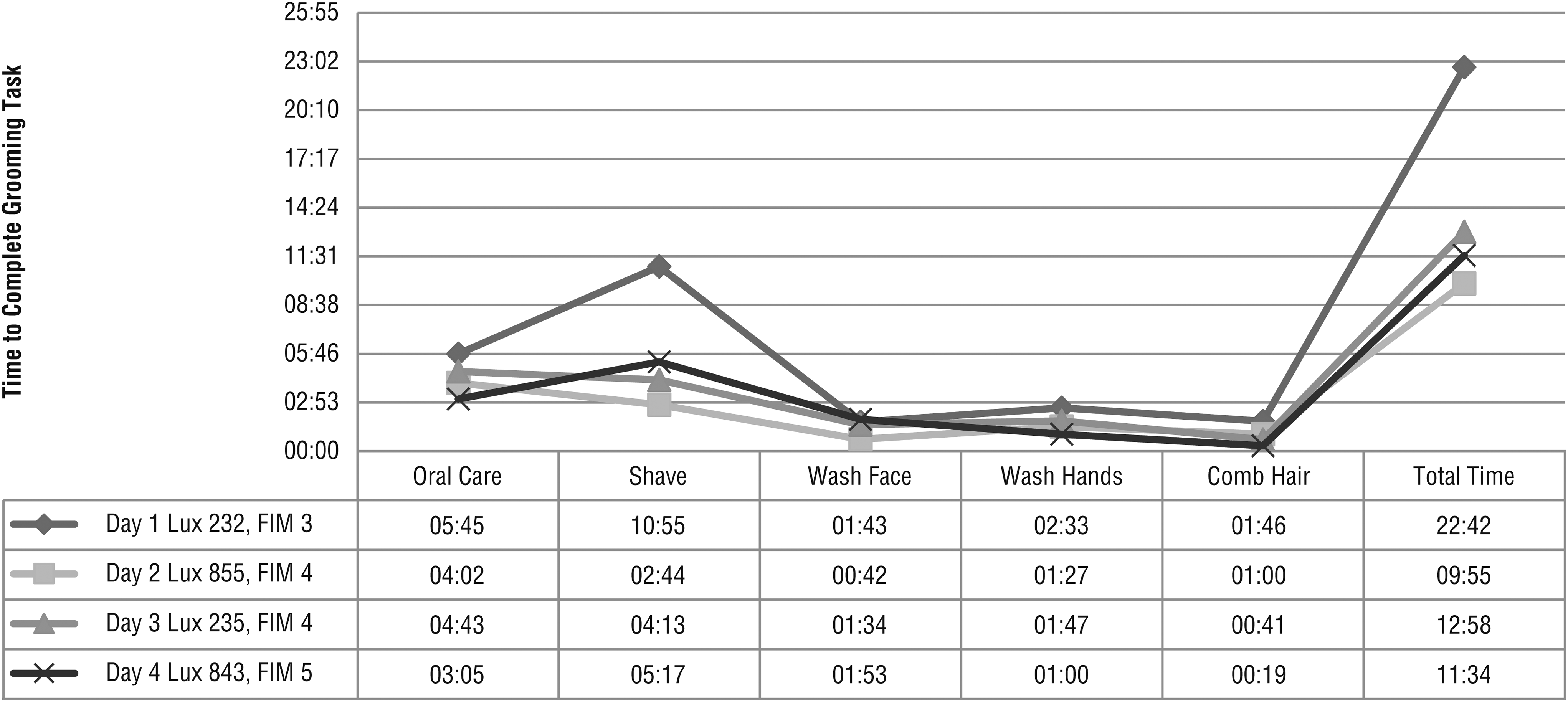
The participant was seated in a wheelchair at the sink with all grooming items placed on a table to the left side of the sink. The items on the table consisted of his toothbrush, toothpaste, rinse cup, washcloth, comb, razor, and shaving cream. This configuration was used all 4 days. The standard lighting in the room consisted of fluorescent lighting positioned somewhat behind him and to his left. He was unable to locate any of the items on the table. He required a physical cue to attend to and retrieve the grooming supplies using his nonaffected right hand. He required verbal and physical cues and some physical assist to complete the grooming task. The total time for completion of all grooming tasks was 22:42 min with 232 lux of light luminance, and his FIM score was 3 (Figure 2).
Participant B’s results.
Day 2.
Additional supplemental lighting included an overhead light and floor lamp with an adjustable reading light shining over the participant’s left shoulder at the sink and table on which the grooming items were placed. He initially stated that he did not think the additional lighting would improve his performance. The amount of brightness was slowly increased to his preference using the dimmer function. With the supplemental lighting in place, only verbal cues encouraging him to look in the direction of the light toward his grooming tools were needed. Physical assistance was required to shave the left side of his face because of hemiparesis and left visual inattention, as on Day 1. His total time decreased to 9:55 min with 855 lux of lighting luminance, and his FIM score was 4 (Figure 2).
Day 3.
The standard room lights were on, and the participant requested that the same lighting be used as on the day before. Study requirements were reviewed and accepted; thus, the lighting was left at the standard level. Participant B required verbal cues to look left and some physical assistance with shaving the left side of his face. Total time was 12:58 min with 235 lux of light luminance, and his FIM score was 4 (Figure 2).
Day 4.
The enhanced lighting was used with the same positioning and procedure as on Day 2. The participant was able to complete all the tasks using his right arm and one-handed techniques. Total time was 11:34 min with 843 lux of light luminance, and his FIM score was 5 (Figure 2). The fourth day was the first time that he was able to wash, apply shaving cream, and shave the left side of his face without cues. Although there was not a large improvement in time compared with Day 3, his performance of the task was at a much higher level, with improved task performance and thoroughness.
Discussion
The timed data and FIM scores indicate that with increased lighting sources, grooming was completed in less time at a higher functional level. This result suggests that increasing the amount of light may improve performance of the occupation of grooming.
It is not clear whether positioning the light sources on the side of hemi-inattention or the increased illumination to participant preference affected performance. Both participants initially believed that enhanced lighting would not be beneficial for grooming. Yet once having experienced enhanced lighting for grooming, both requested increased lighting on Day 3 and identified that it improved their performance. It was significant that Participant A asked for extra lighting on Day 2 because she was unable to recall events from day to day. Participant B kept referring to the need for increased light during other therapeutic activities. For example, during a letter cancellation task, he asked why the morning lights were not used. He believed that his performance on this task would have improved with enhanced lighting. Without enhanced lighting, he did not cancel items on his left past midline of the paper. At his request, a gooseneck lamp was positioned on his left. He then repeated the cancellation task and attended to items on the left side.
Results of this study indicate the importance of individual preference for the amount of lighting in relation to function. Practitioners should have the ability to both increase and decrease the level of illumination in treatment environments depending on clients’ needs. Although the participants in this study demonstrated improved function with increased illumination, it is expected that individuals with other diagnoses may desire less illumination as a result of glare or light sensitivity.
This study is limited by several factors, including the case study design. Also, change in participants’ performance may have been attributable to factors other than enhanced lighting (i.e., task practice, improved orientation). Although the FIM is the most widely used measure in IRFs, it has limitations for the purpose of this study. It is not sensitive enough to appreciate the smaller changes in function that occur from one observation to the next. Future research should incorporate the use and positioning of lighting as a therapeutic modality with various populations and settings. In addition, research could include different bulb types and color temperatures to assess client preference and performance. In addition, studies could further investigate the use of lighting as a cue for hemi-inattention during functional activities.
Implications for Occupational Therapy Practice
This study’s findings have the following implications for occupational therapy practice:
Visual function should be routinely assessed in acute care settings.
Lighting preferences (type, position, power) should be considered as an adjunct to therapeutic intervention.
Occupational therapy practitioners should consider lighting as a visual cue for visual–spatial neglect and visual field deficits.
Conclusion
The results of this study suggest that individualized lighting can lead to improved grooming function in people with CVA. Because vision is essential to the performance of daily occupations, occupational therapists should assess visual function and consider the use of lighting as a therapeutic tool. Clinical observations during this study suggest that lighting may be helpful for cuing individuals with visual–spatial neglect or visual field deficit during occupational performance.