
Abstract
Disability is a well-established risk factor for victimization during childhood (Jones et al., 2012). Studies estimate that youth with disabilities (YWD) are between 1.5 and 3.4 times more likely to experience victimization than their peers without disabilities (Murphy, 2011; Sullivan & Knutson, 2000). Victimization is unwanted physical, sexual, or emotional injury or harm or threat of injury or harm, including death (Lewit & Baker, 1996). Victimizations range in type and severity and include both overtly criminal acts (e.g., child homicide) and relatively common behaviors such as corporal punishment (Lewit & Baker, 1996).
Among youth in the general population, victimization has recurrently been linked to poor mental health outcomes, including both internalizing and externalizing disorders (Finkelhor et al., 2011; Perry & Pollard, 1998; Turner et al., 2006). Although less research has examined the mental health of victimized YWD, preliminary data support the important role that victimization plays in their mental health (Berg et al., 2015; Koenen et al., 2003; Walker et al., 2007). Initial findings from the second National Survey of Child and Adolescent Well-Being (NSCAW II; Berg et al., 2015) documented a disproportionately high prevalence of victimization among adolescents with disabilities in the child welfare system (CWS) and a link between self-reported experiences of victimization and clinically significant symptoms of depression. Specifically, victimized YWD in the CWS were 2.5 times more likely to report clinical symptoms of depression than victimized peers without disabilities (Berg et al., 2015).
The value of engaging clients in participation to promote positive health outcomes is not new to occupational therapy practitioners. In studies on interventions for clients with spinal cord injury (Whiteneck et al., 2004) and brain injury (Huebner et al., 2003), for example, participation in meaningful activities has regularly and consistently been paired with positive health outcomes. For youth who have experienced victimization, research has highlighted the important role of participation in their psychological resilience (Bartko & Eccles, 2003). For example, participation in structured activities has been found to buffer youth without disabilities against the negative mental health outcomes of child maltreatment and exposure to family domestic violence (Conn et al., 2014; Gardner et al., 2012). Evidence suggests that involvement in a variety of structured activities may have more developmental significance for vulnerable youth than intensive participation in one or two activities (Busseri et al., 2006; Rose-Krasnor et al., 2006). The positive effects of varied participation may stem from greater exposure to a range of skills, opportunities, relationships, and experiences (Busseri et al., 2006).
Although the relationship between breadth of involvement and well-being has not been examined among YWD who experienced victimization, it is reasonable to assume that victimized YWD, many of whom have been deprived of growth-promoting opportunities, would reap the positive developmental effects of varied participation. Engagement in structured activities, therefore, may be particularly relevant to the well-being of YWD, who, as a population, are more likely not only to be victimized but also to report social isolation (Coster et al., 2012; Jones et al., 2012; Siperstein et al., 1997).
Promoting and supporting participation in activities, particularly for YWD, is an essential goal of occupational therapy (Arbesman et al., 2013; King et al., 2002; Shikako-Thomas et al., 2008). Although occupational therapy practitioners routinely use specialized skills to maximize youth engagement in activities, the mental health impact of these activities for victimized YWD remains unknown. This gap in knowledge significantly limits practitioners’ ability to reduce and prevent the occupational impacts of mental health distress among YWD and inhibits the inclusion of participation factors as part of a more comprehensive approach to addressing multiple victimization in this population.
Although the current study was not intended to unravel the mechanisms of effect, it is an exploratory effort to identify the contribution of breadth of participation in structured activities to the mental health of victimized YWD. The objective of this study was to test the hypothesis in a nationally representative child welfare sample that greater breadth of participation in structured activities can moderate symptoms of clinical depression among YWD who experience victimization.
Method
Participants
This study is based on data from the NSCAW II, a nationally representative survey of children and adolescents in contact with the CWS. The NSCAW II used a stratified cluster sampling design to recruit 5,873 children and adolescents ages 0–17 yr across 83 counties nationwide. All youth had some form of contact with the CWS over a 15-mo period beginning in 2008 (Dolan et al., 2011). We selected our sample from among adolescents ages 11–17 yr who remained at home with their biological parents (N = 675; Dolan et al., 2011). Youth in out-of-home placements were excluded given the evidence base suggesting that such youth, and their families, are systematically different from those who remain at home (Barth et al., 2006).
Data were collected by means of in-person interviews and survey assessments with adolescents and parents between March 2008 and September 2009 (Dolan et al., 2011). All study procedures were approved by the RTI International internal review board, and all analyses were approved by the University of Chicago internal review board.
Measures
Disability.
In the NSCAW II, parents reported whether their child had a disability using a list of chronic and temporary diagnostic medical conditions (Stein et al., 2013). Youth were identified as having a disability if their parents reported they had one or more of the following conditions: autism or autism spectrum disorder, Down syndrome, developmental delay or intellectual disability, visual impairment or blindness, hearing impairment or deafness, cerebral palsy, muscular dystrophy, epilepsy or seizure disorder, diabetes, heart problems, cystic fibrosis, chronic and severe asthma, blood problems, arthritis or joint problems, HIV/AIDS, or other complex health disability. Cognizant of the clinical overlap between physical and neurodevelopmental disabilities, we used the primary diagnosis to classify disability type.
Youth identified as having a learning, attention, or behavioral health disability without report of a secondary disability were excluded from our operationalization of YWD because of the high prevalence of learning and emotional–behavioral disabilities among adolescents involved with the CWS and the significant evidence base that identifies learning, emotional, and behavioral disabilities as common sequelae of child maltreatment (Conroy & Brown, 2004). Furthermore, regression analyses including an additional dummy variable containing youth with emotional, learning, or behavioral disabilities did not result in significant differences in outcomes. Using these criteria resulted in a subsample of 247 YWD ages 11–17 yr.
Victimization.
Our study used NSCAW II data to investigate self-reported victimization among the youth during the previous 12 mo. Prior-year victimization was the most appropriate choice for three reasons: (1) Research indicates that bounding the recall period decreases error in self-reported victimization; (2) reported victimizations would have occurred within a relatively short window of time for this cohort, indicating a high level of extant vulnerability; and (3) lifetime tallies of victimization are skewed toward older youth who, by virtue of their age and greater exposure, have accrued a greater number of victimizations (Finkelhor et al., 2007).
In this study, measurement of prior-year victimization was based on youth self-report. Reported victimizations were categorized as physical abuse in the home, emotional abuse in the home, physical victimization outside the home, and threat or assault with a weapon. Physical abuse in the home was indicated by YWD report of one or more of the following events from the Severe Assault subscale of the revised Parent–Child Conflict Tactics Scales (CTS2; α = .55): A parent or adult in the home choked, beat or repeatedly hit, or scalded or burned him or her (Straus et al., 1998). Emotional abuse in the home was indicated by YWD report of one or more of the following events during the previous 12 mo, as assessed by the CTS2 Psychological Aggression subscale: a parent or adult in the home called the YWD “dumb,” “lazy,” or some other name or swore at the youth (Straus et al., 1998).
Victimization that occurred outside the home was measured using the Child Health and Illness Profile–Adolescent Edition (CHIP–AE; α > .70; Starfield et al., 1995). The CHIP–AE measures injury and disease in children and adolescents ages 11–17 yr. YWD were considered physically victimized outside the home if they reported physical injury as a result of violence that occurred in a school, neighborhood, mall, friend’s home, or other setting. YWD who were assaulted or threatened with a weapon were identified on the basis of reported experience of a gunshot or stab wound or a threat with a knife or gun by an adult in the home.
Prior-year victimization experiences were summed for each YWD, with total scores ranging from 0 to 4. YWD who reported at least one form of victimization over the previous year were considered victimized for the purposes of this study. This operationalization of victimization corresponds with research on the negative mental health effects of diverse types of victimization, including emotional abuse (Finkelhor et al., 2007; Perry & Pollard, 1998).
Participation.
Participation in structured activities was assessed using the Youth Self Report of the Child Behavior Checklist (CBCL; mean test–retest reliability of the Social Competence subscale, .87; activity section, .70; and social section, .92; Achenbach, 1991). The Social Competence subscale of the CBCL is commonly used to assess activity participation among children and adolescents with and without disabilities (Conn et al., 2014), and a significant body of empirical research supports its content and construct validity (Achenbach, 1991).
In concordance with prior studies, items from the subscale pertaining to activity participation were selected for analysis (Conn et al., 2014). Participation was indicated by YWD involvement in one or more of four types of structured activity: (1) clubs, organizations, or teams; (2) hobbies, activities, or games; (3) sports; and (4) chores or jobs. Yes–no responses to each of the 4 categories of activity were recoded (1 = yes, 0 = no) and aggregated for each YWD to construct total participation scores. Reported participation in three or more structured activities was classified as higher breadth of participation, and engagement in two or fewer activities (including no participation) was classified as lower breadth of participation. This classification is based on previous studies of participation in which engagement in three or more activities was linked to positive developmental outcomes (Fletcher & Shaw, 2000). Dose of participation in each type of structured activity was not measured.
Mental Health.
For this study, we were primarily interested in identifying youth who experienced clinical depression, given its relevance for health practitioners. In the NSCAW II, clinical depression was measured using youth responses to the Children’s Depression Inventory (CDI; Kovacs, 1985). Respondents were classified as clinically depressed if they scored at or above the 91st percentile on the basis of the normative sample’s depression rates (Kovacs, 1985). Studies of the CDI have indicated that it has good internal consistency (Cronbach’s αs = .71–.86) and concurrent validity with other depression scales (Kovacs, 1985).
Covariates.
Covariates in the NSCAW II included key family and community demographic factors (i.e., age, race, gender, parent education, marital status, family poverty, and urban or rural residence). Additional variables included family domestic violence, family substance abuse, parent mental and physical health status, participant loneliness, and parent–child closeness. Often used in victimization and developmental psychopathology research studies, these variables have been identified as common correlates of both victimization and maladaptive outcomes after exposure to violence (Emerson & Brigham, 2015; Turner et al., 2006).
Analysis
Statistical procedures in Stata 13 (StataCorp, College Station, TX) were used to account for the complex survey design. Given that the sample was restricted to YWD residing with their biological parents, domain analysis was used to readjust for sample weights facilitating generalization to the national sample of CWS-involved YWD who resided at home.
Multivariable probit regression analysis was used to investigate the effects of victimization and participation on clinical depression symptoms among YWD. Probit regression is a commonly used strategy to model dichotomous outcome variables that are based on an underlying continuous variable. Unlike logistic regression, which uses logit link function, in probit regression the inverse standard normal distribution of the probability of the outcome is modeled as a linear combination of the predictor variables (Aldrich & Nelson, 1984). Because of this model setup, the report of β coefficients in a probit model contains the z scores that can be compared on the underlying normal distribution. The interpretation is that when the z score increases, the probability of the outcome increases. The exact probability changes would be computed by marginal probabilities from the model.
Given that we derived the binary clinical depression outcome by dichotomizing the continuous CDI T scores, it is reasonable to assume that an underlying continuous variable was driving the observed binary. Thus, the probit model was the preferred approach for our study. Inclusion of the interaction term in the probit model permitted an investigation of the moderating effect of participation on the relationship between victimization and clinical depression. The Huber–White estimator was used to calculate standard errors.
Although the variable selection during model building was driven primarily by theory and empirical research, to avoid potential issues of overfitting we conducted additional analysis in which we limited our explanatory variables to four, as recommended by Stoltzfus (2011). Because the model-fitting results remained similar and there was no change in our conclusions, we decided to report the original model (goodness of fit, p = .9219). We also investigated the potential threat of multicollinearity. The average variance inflation factor across the explanatory variables was 1.11 (range = 1.06–1.19). Finally, to examine the predicting power of the model, we computed the area under the curve (AUC). The AUC of the current model was .82, suggesting that the model had very good predictive utility.
Results
Approximately 37% (n = 247) of respondents in the NSCAW II sample had disabilities, as reported by their parents. The average age of our sample of CWS-involved YWD who remained at home (N = 247) was 13.6 yr (Table 1). More than half were female (57%), fewer than half identified as White (43%), more than half (54%) lived in households with incomes at or below the federal poverty line, and nearly 70% lived in an urban area. The majority (65%) had experienced at least one form of victimization over the previous 12 mo. About one-third (38%) reported lower breadth of participation, and nearly two-thirds (62%) reported higher breadth of participation (i.e., involvement in three or more types of structured activities). A significant minority (14%) reported symptoms of clinical depression.
Sample Characteristics and Bivariate Analysis
Note. Missing values for participation variables resulted in a smaller sample size for analyses (N = 242). M = mean; SD = standard deviation.
Recently victimized YWD did not differ significantly from YWD who did not report prior-year victimization in terms of demographic or family variables; however, as a group, victimized YWD had a higher prevalence of clinical depression (19% vs. 5%; p < .01). YWD who reported higher breadth of participation differed from those who reported lower breadth of participation on several characteristics; those who reported participating in three or more activities were more likely to be younger (13.2 yr vs. 14.2 yr; p < .01) and male (p < .01) and to reside in nonurban settings (p < .05; Table 1).
The results of our multivariable probit regression model are based on the z score classification system. In our full regression model, age and gender of YWD were independently associated with clinical depression outcomes (Table 2; Model 1). Higher age (z = −0.24, p = .011) was correlated with a lower probability of clinical depression, whereas female gender (z = 1.06, p < .001) was correlated with a higher probability of clinical depression. Parent gender was also associated with clinical depression; female primary caregivers (z = −1.54, p = .002) were associated with a lower probability of clinical depression in the YWD. Finally, prior-year victimization (z = 0.92, p = .004) was linked with a higher probability of clinical depression.
Results of Multivariable Probit Regression Models With Clinical Depression as the Outcome Variable
Note. Clinical depression is defined as Children’s Depression Inventory T score ≥65. Area under receiver operating characteristic curve = .82; correct classification = 85.29%; average variance inflation factor = 1.11 (range = 1.06–1.19); goodness of fit, p = .9219; passed the linktest. AIC = Akaike information criterion; BIC = Bayesian information criterion, CI = confidence interval.
Table 2 summarizes the results of our moderation test (Model 2). The size and significance of the interaction term indicates that breadth of participation in structured activities moderated the relationship between prior-year victimization and clinical depression. Victimized YWD who reported higher breadth of participation (z = −1.76, p = .003) had a lower probability of clinical depression. Translated into probability estimates, the probability of reporting clinical depression was >4 times lower for victimized YWD who reported higher breadth of participation than for those who reported lower breadth of participation (6% vs. 26%, p = .03; Figure 1).
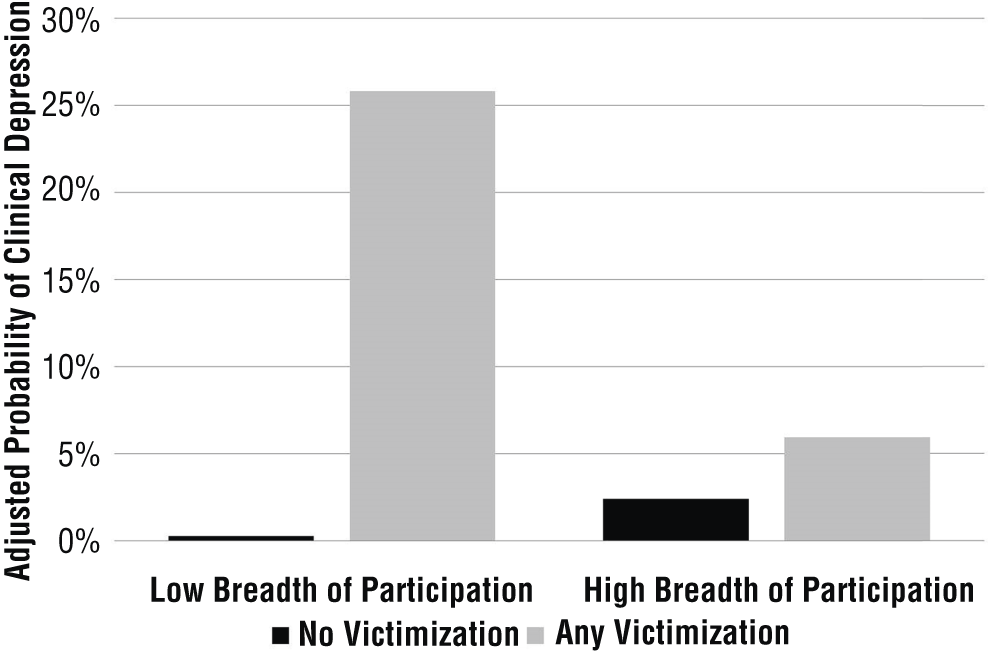
Adjusted probability of clinical depression, by breadth of participation and victimization.
Discussion
Breadth of participation in structured activities emerged as a significant factor in the mental health of victimized YWD. Recently victimized YWD who reported lower breadth of participation experienced significantly higher rates of clinical depression. The relationship between breadth of participation and clinical depression among victimized YWD remained robust even with the inclusion of child and family factors. Regardless of poverty, parental depression, or other known risk factors, the probability of clinical depression among YWD who actively participated in three or more types of activities was 4 times lower than among peers who reported lower breadth of participation. Although results describing a relationship between participation and mental health for YWD have not previously been documented in the literature, this finding is consistent with research on the positive mental health effects of structured participation on vulnerable youth (Busseri et al., 2006; Conn et al., 2014; Gardner et al., 2012; King et al., 2002).
Notably, in our study, participation in two or fewer structured activities was not sufficient to offset the negative mental health effects of recent victimization among YWD. Like those of Gardner et al. (2012), our findings suggest that YWD must meet a particular threshold of involvement to reap positive mental health effects. In the calculus of mental health, higher levels of participation are required to outweigh the negative costs of victimization. This finding is echoed in several studies that linked either intensity or breadth of participation to more beneficial outcomes in academic and behavioral functioning (Busseri et al., 2006; Gardner et al., 2012; Rose-Krasnor et al., 2006).
Also of significance was the relationship among youth gender, urban residence, and breadth of participation. Consistent with prior studies, male YWD in our study were more likely to report higher breadth of participation in structured activities than female YWD (Fletcher & Shaw, 2000). This disparity in breadth of involvement may reflect gender differences in activity preferences (structured vs. unstructured) as opposed to disparities in overall levels of participation (Fletcher & Shaw, 2000). Place of residence also emerged as a significant correlate of breadth of participation. Lower breadth of participation among urban YWD may be linked to the joint effects of neighborhood disadvantage and family poverty. In our study, household poverty was substantially higher than the national average; more than half (54%) of YWD in our sample came from households in poverty compared with 20% of youth nationally (DeNavas-Walt & Proctor, 2014). For urban families, the adverse effects of low socioeconomic status may be compounded by a dearth of community-based support mechanisms, resulting in significant obstacles to participation for YWD (Randall & Bohnert, 2009).
Our findings, although promising, must be interpreted in light of several limitations. This study used a cross-sectional design, which makes it difficult to establish direction of causality. In anticipation of this challenge, we examined YWD participation levels at baseline and CDI scores at 18-mo follow-up. The relationship between participation and clinical depression remained unaltered, although our findings were less robust given the significant number of missing values at follow-up. Nevertheless, consistency across waves in the size and strength of the relationship between breadth of participation and clinical depression among recently victimized YWD gave us greater confidence in the veracity of our conclusions. This study also relied on self-reported victimization and participation data. Although self-reported data are advantageous, particularly in the absence of observational data, youth with more profound impairments may be underrepresented in this sample. Because this study’s operationalization of victimization was constrained by data set limitations, our variable may not have captured the full range of recent victimizations experienced by YWD in the CWS.
Despite these limitations, the relatively high prevalence of prior-year victimization and clinical depression noted in our sample indicates that the short- and long-term functioning of YWD in the CWS may be at significant risk. Mental health challenges compound the obstacles YWD face in meeting the developmental tasks of adolescence and can further impede their transition to adult independence. Future research on breadth of participation could yield important findings on cost-effective interventions to promote mental health in at-risk YWD. Identifying optimum types, dosages, and combinations of structured activities could assist occupational therapy practitioners in designing and facilitating effective interventions to promote participation among YWD who experience victimization.
Implications for Occupational Therapy Research and Practice
Despite these limitations, our findings have the following implications for research and practice in occupational therapy:
Our study builds on a mounting body of evidence in occupational therapy and other disciplines supporting the value of diverse participation for vulnerable youth (Arbesman et al., 2013; Jirikowic & Kerfeld, 2016; Shikako-Thomas et al., 2008).
Occupational therapy practitioners frequently work with children who experience victimization and its physical and mental health sequelae. From both an evaluation and intervention standpoint, practitioners could benefit from increased knowledge of victimization and the skills to identify YWD who experience victimization, implement skill-building activities to boost resilience among victimized YWD, and facilitate engagement in three or more structured activities for victimized YWD.
This study suggests an expanded role for occupational therapy in recognizing the value of participation for youth who experience victimization. Occupational therapy practitioners can apply their specialized skills in task analysis and environmental modification to optimize participation in meaningful activities for victimized YWD, thereby facilitating greater social inclusion and resilience.
Footnotes
Acknowledgments
This study used data from the second National Survey of Child and Adolescent Well-Being, a longitudinal study sponsored by the Office of Planning, Research, and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services. The authors were supported in part by T 73 Grant MC11047 from the Human Resources and Services Administration.