
Abstract
School participation encompasses achieving individual needs and personal goals related to academia and fulfilling social expectations (Coster, 1998). Students with intellectual and developmental disability (IDD) have been found to participate less in educational settings compared with their peers without disabilities (Coster et al., 2013).
IDD is “characterized by significant limitations in both intellectual functioning and adaptive behavior in many everyday social and practical skills” (Schalock et al., 2010, p. 3). It originates before age 18 yr in about 1% of the general population (American Psychiatric Association, 2013). IDD is further categorized by its severity level on the basis of the degree of functional limitations or by the intensity and diversity of supports required. In this study, we focus on people with moderate IDD who require supports characterized by regular (e.g., daily) involvement in at least several environments, such as school or home, that are not time limited (American Psychiatric Association, 2013).
Participation of Students With Disabilities
Participation is often defined as “involvement in a life situation” (World Health Organization [WHO], 2007, p. 9) and is a key indicator of health and well-being; thus, it is a critical intervention goal for people with disabilities (Chang & Coster, 2014). Previous research indicates decreased participation among students with disabilities in school-related settings (for a review, see Coster et al., 2013). In addition, students with IDD are often characterized by limited ability to transfer skills and behaviors learned in one situation to another (Jansen, De Lange, & Van der Molen, 2013).
Intervention for Enhancing Students’ Participation
Over the years, a few intervention programs have been developed to enhance the participation of students with disabilities in various domains, and participation in out-of-school activities is enhanced by direct intervention programs (e.g., Tonkin, Ogilvie, Greenwood, Law, & Anaby, 2014). However, most reports are descriptive and focus on providing detailed participation profiles of these students (e.g., Coster et al., 2013). Intervention studies regarding participation in classroom-related activities of students with IDD are sparse. In some case studies, researchers have reported improved participation in specific school-related activities. For example, Villeneuve and Hutchinson (2012) developed an intervention program, based on a collaborative consultation model, to examine a school-based occupational therapy consultation program and found that the following measures supported outcomes: (1) focus for educational programming, (2) communication practices, and (3) leadership practices of educators. The authors presented this model as possibly enhancing student participation.
Collaborative Consultation Model
Collaborative consultation refers to the interactive process involving professionals with diverse expertise working together as equal partners to enhance the academic achievements and functional performance of students (Hanft & Shepherd, 2008). This process includes voluntarily sharing team members’ knowledge and experience with the team, jointly setting the intervention goals and program, and sharing the responsibility for intervention outcomes (Hanft & Swinth, 2011). Collaborative consultation is a specific form of an indirect service delivery model. Currently, the most commonly implemented of these models within the educational system is the in-service model (Malone, Straka, & Logan, 2000).
In-service refers to experts providing specific knowledge or training to professionals in their area of expertise. It is a key component of continuing education for teachers and often enables discussion and hands-on practice of a specific skill (European Training Foundation, 2013). However, there is a growing body of evidence suggesting that in-service alone may not be sufficiently effective (e.g., Golos, Sarid, Weill, & Weintraub, 2011). Therefore, we developed a combined model of in-service and collaborative consultation—Collaborative Consultation for Participation of Students With Intellectual Disability (Co-PID; Selanikyo, Yalon-Chamovitz, & Weintraub, 2017)—with the assumption that the intervention would be most effective if planned and implemented within the students’ classroom by a multidisciplinary team.
Collaborative Consultation for Participation of Students With Intellectual Disability Program
The Co-PID is a theoretically driven intervention that is based on the bio-psychosocial model of the International Classification of Functioning, Disability and Health—Children and Youth (ICF–CY; WHO, 2007) and on the conceptual framework of the Human Functioning Model of the American Association on Intellectual and Developmental Disabilities (Schalock et al., 2010). These models recognize that participation is a vital part of human development and lived experience (Law, 2002) and emphasize the significance of individualized support systems in improving and enhancing participation and functional skills (Schalock et al., 2010).
Participation Components of the Consultation for Participation of Students With Intellectual Disability Program
In accordance with the collaborative consultation principles, after a 6-mo brainstorming and learning process (for an elaboration of the process, see Selanikyo et al., 2017), the Co-PID development team identified three vital participation skills for students’ participation in classroom-related activities: (1) communicating, (2) choosing, and (c) initiating. This conceptualization was supported by a literature search (Baurain & Nader-Grosbois, 2013; Blain-Moraes & Chau, 2012) showing that students with IDD often exhibit difficulties in these three components of the Activities and Participation section of the ICF–CY (WHO, 2007).
On the basis of the ICF–CY (WHO, 2007), communicating ranges from attending to verbal and nonverbal messages (§§ d310–d329) to expressing oneself in spoken, written, or sign language (§ b167). In addition, it includes hand gestures, noises, and alternative supporting means of communication, such as a communication board (§§ d330–d332, d335). Choosing involves the ability to choose from various options, implement the choice, and evaluate its impact. This component may include choosing objects and activities (§ d177). Initiating is defined as “causing or facilitating the beginning of (something)” or “set going” (“Initiate,” n.d.), and it is an underlying component of acquiring skills (§ d355) or undertaking multiple tasks (§ d220). Because ICF–CY definitions are congruent with the models underling the Co-PID, it was decided that the components of participation would be measured on the basis of a performance perspective (WHO, 2007), namely, the students’ involvement in their daily classroom routine.
Previous Findings
A preliminary study (Selanikyo et al., 2017) was conducted to examine the effectiveness of the Co-PID intervention program for enhancing participation among students with moderate IDD (n = 69). When comparing between two convenient sample groups, we found a significant improvement in students’ participation in the Co-PID group (n = 35), whereas the participation of the In-Service (IS) group (n = 34) decreased. However, this preliminary study had several methodological limitations. The Co-PID was implemented by the Co-PID development team members, who may have been enthusiastic or invested in its success. The IS program consisted of a one-time meeting, and thus the difference in the programs’ duration may have constituted a flaw in the design. Finally, participation was assessed by a single outcome measure that did not enable triangulation.
Objectives and Hypothesis
The purpose of the current study was to further develop and corroborate the effectiveness of the Co-PID by replicating the initial study after addressing the aforementioned limitations. Therefore, the current study was implemented in two educational settings in which (1) the team members were not part of the development team, (2) in-service duration was prolonged, and (3) two additional outcome measures were used. Our main research question was as follows: Is the Co-PID an effective program for enhancing participation in classroom-related activities in students with IDD? In addition, we asked the following question: Would the Co-PID have a transfer effect to participation in other school environments beyond the classroom?
Method
Research Design
The study followed a pretest–posttest case-control design (Thiese, 2014) and compared two school-based intervention programs: the Co-PID (intervention group) and the IS (control group). Of the 10 potential schools, 3 agreed to participate in the study, of which 2 were chosen on the basis of their similar socioeconomic and cultural backgrounds. The two schools were randomly assigned to the Co-PID or the IS group. Within the schools, a convenient sampling method was applied to recruit participants from all classrooms. Ethical approval was obtained from the Ministry of Education, followed by a preliminary meeting with each school, where the administrators and homeroom teachers received an explanation about the study and were asked to sign consent forms. Next, written consent was obtained from the students’ parents. The students themselves did not sign consent forms because of the complexity of this study and their inability to fully understand it.
Participants
The homeroom teachers (Co-PID, n = 4; IS, n = 7) met the following inclusion criteria: (1) worked at the school at least 3 days per week and (2) taught at the school for at least 1 yr before data collection. The students (Co-PID, n = 28; IS, n = 32) were included if they met the following criteria: (1) a diagnosis of moderate IDD (see the introduction section) as defined by the Municipal Psychology Service; (2) mobility independence (i.e., the ability to move within the classroom without staff assistance); (3) no secondary diagnosis of autism or sensory disabilities, such as blindness or deafness; and (4) had been studying at the school for at least 1 yr before data collection.
Instruments
Structured Observations of Students’ Participation in Classroom.
The Structured Observations of Students’ Participation in Classroom (SOSPiC; Selanikyo et al., 2017) was developed along with the Co-PID as a structured observation for examining participation of students with moderate IDDs in the classroom. It includes 25 items focusing on three skills relating to participation in classroom-related activities: (1) communicating (listening and expressing; 7 statements; e.g., “Responds physically [gesture] when his or her name is directly called on [looks up, reaches out, turns his head . . .]”); (2) choosing (8 statements; e.g., “Selects one object out of objects presented in accordance to the context of the lesson”), and (3) initiating (10 statements; e.g., “Initiates a request of a personal need such as ‘I want to eat’”).
To collect the data for the measure, the observer conducts an observation throughout an entire lesson (∼45 min). The observer rates the active participation of students for each item on a scale ranging from 0 (does not participate) to 4 (fully participates). In addition, each statement includes a “not relevant” option—applicable when the student is not given the opportunity to perform the task. A mean score is calculated for each participation area.
The SOSPiC had fair interrater reliability (intraclass correlation coefficient = .78, 95% confidence interval [.585–.925]). Test–retest reliability was found to be medium to good: communicating, r = .64; choosing, r = .81; and initiating, r = .82 (all ps < .05). Internal consistency of the entire observation was very good (α = .93), and the three areas varied from good to low: communicating, α = .78; choosing, α = .86; and initiating, α = .62 (for elaboration on the development and psychometric properties of the SOSPiC, see Selanikyo et al., 2017).
School Function Assessment.
The School Function Assessment (SFA; Coster, Deeney, Haltiwanger, & Haley, 1998) is a criterion-referenced, standardized assessment that measures students’ performance in functional tasks supporting their participation in the school program. The SFA includes three parts: (1) participation, (2) task supports, and (3) activity performance. It is completed by one or more school professionals who are highly familiar with the students being observed.
Only the participation section was used in the current study because this section was the main focus of our work. The rater assesses participation of each student in six major school settings: (1) special education classroom, (2) playground or recess, (3) traveling to and from school, (4) bathroom and toileting activities, (5) transitions to and from class, and (6) mealtime or snack time. Rating is based on a scale ranging from 1 (participation is extremely limited) to 6 (full participation). The raw score (one participation score is obtained) is converted to a criterion score ranging from 0 to 100. With the authorization of the publishers, the SFA was translated into Hebrew and was found to be valid and reliable among Israeli children (Schenker, Coster, & Parush, 2005): The internal consistency ranged from .92 to .98, and test–retest was .82 < r < .98.
Goal Attainment Scaling.
Goal attainment scaling (GAS; Kiresuk, Smith, & Cardillo, 1994) is a method for scoring the extent to which the client’s goals are achieved during the course of an intervention. Functional goals are determined through a collaborative process between clinician and client or caregiver before intervention. Scoring is based on each goal’s performance on a scale ranging from −2 to 2, where −2 represents current status, 0 represents the expected goal, and 2 represents greater-than-expected outcomes. Raw scores are transformed to a standardized t score (mean [M] = 50, standard deviation [SD] = 10; Vu & Law, 2012). The GAS has been found to have good interrater reliability (0.73–0.92), variable validity, and excellent responsiveness (Krasny-Pacini, Hiebel, Pauly, Godon, & Chevignard, 2013; Vu & Law, 2012).
Procedure and Data Collection
The study was conducted in three phases: (1) pretest (8 wk), (2) intervention (16 wk), and (3) posttest (8 wk).
Pretest.
Using the SOSPiC, we observed both groups four times during different lessons (with a 1-wk interval between observations) to establish a baseline for level of participation. All pretest observations were conducted between the 2nd and 3rd mo of the school year by an occupational therapist with 8 yr of experience working with children with developmental delays. The observer was trained in using the SOSPiC and was not blinded to the schools’ assignment (Co-PID or IS). During this period, the teachers, who were blinded to the school assignment, were asked to teach in a regular manner without changing the content or design of their lessons. Next, the teachers filled out the SFA questionnaire for each student. Finally, on the basis of the SOSPiC’s scores and the teachers’ familiarity with the students’ function, the occupational therapist and each of the participating teachers jointly used the GAS to create student goals. Each student had three goals, one for each of the participation skills: communicating, choosing, and initiating.
Intervention.
The Co-PID and IS intervention programs were carried out in parallel; in each school, the team included an occupational therapist who was guided by the first author and a team of homeroom teachers.
The Co-PID was carried out between the 3rd and 7th mo of the school year. The Co-PID had two phases. The first phase was (1) a 1.5-hr in-service meeting introducing the concept of “participation” (WHO, 2007) as it relates to students with intellectual disabilities in the classroom and (2) a workshop. The teachers were asked to choose a lesson that they had already taught and to explore potential activities or forms of expression that they could add to this lesson plan to enhance students’ participation. Next, each teacher presented their ideas to the group, followed by a group discussion.
In the second phase of the Co-PID intervention, a collaborative consultation model was used. It included eight 45-min consultation meetings, which took place every other week over a 4-mo period between the occupational therapist and each teacher. The brainstormed activities could be implemented by the teacher to enhance participation among the students, for example, asking the students to choose one of two activities during the lesson. In each meeting, activity ideas were generated that could be integrated into the existing curriculum. The collaborative meetings were systematically documented (for meeting layout, see Figure 1).
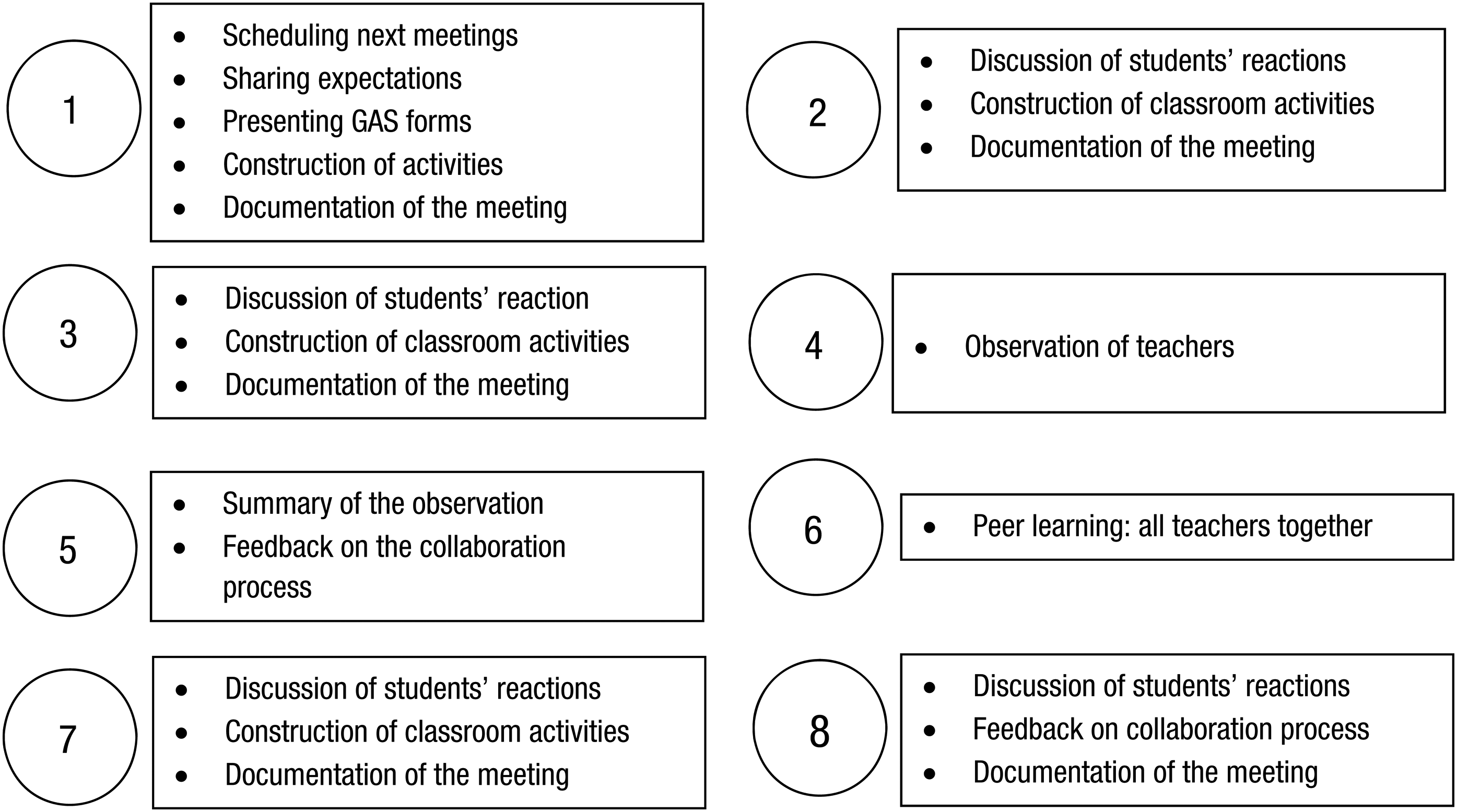
Consultation meetings layout.
The teacher documented the students’ reaction and behavior to the activities implemented in the classroom on a daily basis using a structured form describing the activity or interaction and the students’ response. On the basis of these records, new activities were integrated into the following week’s curriculum. Both the consultation sessions and the teachers’ documentation were used to determine fidelity of treatment.
In the IS (control) group, three meetings were conducted. The first meeting was a 1.5-hr in-service meeting, similar to the Co-PID group. Teachers were asked to implement the ideas shared during the classroom meeting. This meeting was followed by two additional 45-min meetings that took place during the 5th and 7th mo of the school year. Each teacher was asked to present activities executed during different lessons, which led to the participation of a specific student or a group of students. This was followed by a group discussion.
Posttest.
This phase was conducted during the 9th and 10th mo of the school year, identical to both process and measures used in the pretest.
Data Analysis
We performed statistical analysis using IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY). Significance level was set at p < .05. Descriptive statistics were used to describe the participants’ characteristics and the attainment of their individual goals as measured by the GAS. Although all measures were based on ordinal scale, parametric statistics analyses were used because the final scores of the measures were based on mean or sums of all items (Davison & Sherman, 1988).
We used t tests to compare the groups’ demographic characteristics, and we used Pearson’s correlation coefficients to investigate correlations between age and number of years at school and SOSPiC scores. A repeated-measures multivariate analysis of covariance of Time (pre- and posttests) × Intervention (Co-PID vs. IS) controlling for years at school (see the Results section) was conducted to estimate the effect of the two intervention programs both within and between groups for the SOSPiC and SFA. We performed post hoc analysis using paired t tests to compare pre- and posttest scores within each group, separately for the SOSPiC and SFA measures. Finally, a repeated-measures multivariate analysis of variance was used to examine Time × Group effects with respect to the three GAS scores. This was followed by paired t tests.
Results
Sample Description
In the Co-PID intervention group, all the homeroom teachers of students with moderate IDD chose to participate (n = 4). Their mean years of experience with IDD was 7.75 (SD = 1.71). In the IS intervention group, 7 of 8 homeroom teachers chose to participate. Their mean years of experience working with students with IDD was 6.71 (SD = 3.55). In the Co-PID group, 28 out of the 32 students met the inclusion criteria (M age = 14.68 yr, SD = 3.88), of whom 17 (60.7%) were boys. The range of their years at school was 1–12 (M = 5.79, SD = 3.28). In the IS group, 32 out of the 56 students met the inclusion criteria (M age = 13.50 yr, SD = 4.70), of which 16 (50%) were boys. The range of their years at school was 1–14 (M = 6.66, SD = 4.30).
All participants, students and teachers, completed the entire study. No significant differences (p > .05) were found among the groups with respect to age and years at school. Sample size was calculated (Cohen, 1988; Uitenbroek, 1997) on the basis of the results of an earlier study (Selanikyo et al., 2017; described in the introduction section) that consisted of two groups of a similar student population (experimental group, n = 35; control group, n = 34). Analysis showed that on the basis of a desired power of .90 at a significance level of .05, a minimum sample size of 19 was required for each group.
Because of the wide range of age and years at school, we explored the potential intervening effect of these factors. Similar to previous reports (e.g., Yalon-Chamovitz, Mano, Jarus, & Weinblatt, 2005), our results showed that years at school were significantly correlated with two of the SOSPiC skills measured at pretest (communicating, r = .33, p < .01; initiating, r = .27, p < .05) and with the SFA mean score (r = .22, p < .05) but not with the GAS scores. Consequently, years at school was considered an intervening variable.
Intervention Effect
We examined the intervention effect on the basis of the SOSPiC and the GAS scores. Means and standard deviations of the pre- and posttest scores are presented in Table 1. With respect to the SOSPiC, the results of the repeated-measures multivariate analysis of covariance (controlling for years in school) showed neither an overall significant time effect nor an effect for each of the participation components. However, post hoc analyses, which used paired t tests (see Table 1) for each group separately, showed that in both study groups there was a significant decrease in the communicating scores. In contrast, we found a significant improvement in the choosing scores of the Co-PID group. No significant difference was found with respect to initiating.
Means, Standard Deviations, and Pretest–Posttest Comparisons on the SOSPiC, GAS, and SFA by Group
Note. GAS and SFA pretest and posttest scores represent initial status before intervention and status after intervention, respectively. Co-PID = Collaborative Consultation for Participation of Students With Intellectual Disability; GAS = goal attainment scaling; IS = In-Service; SFA = School Function Assessment; SOSPiC = Structured Observations of Students’ Participation in Classroom.
p < .05.
In addition, we found an overall significant large group effect, F(3, 55) = 44.11, p < .001, 


As opposed to the SOSPiC, the GAS showed a large significant overall time effect, F(3, 56) = 50.67, p < .001, 


Time and Time × Group Interactions Effects on the Three GAS Participation Goals



Note. GAS = goal attainment scaling.
p < .05.
We examined how many students in each group attained their individual goals on the GAS. Table 3 shows that in the Co-PID group, more than 28% of the students reached or exceeded each of their intended goals; in the IS group, only 6% of the students reached or exceeded their communicating and initiating goals, and 20% reached their choosing goals.
Frequencies of the Three GAS Participation Goals by Study Group
Note. Co-PID = Collaborative Consultation for Participation of Students With Intellectual Disability; GAS = goal attainment scaling; IS = In-Service.
Transfer Effect
The SFA questionnaire was used to examine the transfer effect of the intervention from the classroom to other school environments. Results showed a significant large time effect, F(1, 57) = 4.73, p < .03, 
Discussion
Students with IDD often depend on others to maximize participation in school settings. On the basis of a SOSPiC analysis of participation, the Co-PID group showed significantly greater improvement in choosing compared with the IS group. Choosing strongly depends on a person’s opportunities, and teams working with children and adults with IDD have often limited their opportunities to choose on the basis of the common misconception that people with IDD lack the ability to make informed decisions or choices (Baurain & Nader-Grosbois, 2013). Moreover, Agran, Storey, and Krupp (2010) investigated choice making and self-determination among young adults with IDD in work settings and found that teachers tended to facilitate the least choice opportunities in comparison with job coaches, parents, and others.
The greater ability to choose in the Co-PID group can be attributed to the collaborative consultation process, which not only enhanced the homeroom teachers’ awareness of the importance of providing choice-making opportunities but enabled brainstorming specific means for embedding choice-making opportunities in the classroom. Indeed, findings from previous studies conducted in special education and inclusive schools with other populations (e.g., students with fine motor difficulties, learning disabilities) have suggested that collaborative consultation between therapists and teachers may improve students’ performance (Golos et al., 2011; Reid, Chiu, Sinclair, Wehrmann, & Naseer, 2006; Villeneuve, 2009).
In contrast, both groups exhibited a decrease in communicating when comparing pre- and posttests, whereas no difference was found in initiating. These results resemble those obtained in a preliminary study (Selanikyo et al., 2017) and may stem from the nature and complexity of these participation components. As stated earlier, the ability to choose depends, to a great degree, on the available opportunities for choice making. Communicating and initiating, however, may rely more on personal abilities (bodily functions) and developmental profile in addition to the quantity and quality of intervention (Woynaroski, Yoder, Fey, & Warren, 2014). Hence, improvement in these components may require a longer intervention.
Analyses of the GAS individualized participation goals suggested an overall significant improvement for both groups. However, in the Co-PID group, at least 20% of the participants achieved their expected goals, whereas 31% students exceeded their expected goals, as opposed to the IS group, in which 10% of the students exceeded their expected goal but only in the choosing component. Current literature has asserted that children and adults with IDD have extremely diverse developmental profiles with unique abilities and difficulties (e.g., Daunhauer, Fidler, & Will, 2014). As concluded by previous studies (e.g., Mailloux et al., 2007) and as indicated by our current work, GAS provides a unique research tool that has the ability to tap into various concerns related to treatment effectiveness. These properties of GAS are especially important when outcomes are variable and standardized tests are not available (Perdices & Tate, 2009).
The measures that we used complement each other. Whereas the SOSPiC detected an overall trend that is important for overall planning, the personalized nature of the GAS and its sensitivity to change enabled us to accurately understand the difference between groups.
We were also interested in the transfer effect of the Co-PID intervention. On the basis of the SFA scores, the Co-PID group showed significant improvement in participation in five other school environments (beyond the classroom), whereas the IS group showed no such improvement. It appears that the students in the Co-PID group transferred their newly acquired skills. This finding is especially significant given the literature indicting difficulties in transfer abilities in this population (Hua, Woods-Groves, Kaldenberg, Lucas, & Therrien, 2015). Generalization or transfer is one of three important cognitive skill deficits exhibited by students with IDD (along with attention and memory). Teaching strategies that may be used to address difficulties in transfer with students with IDD include teaching material in relevant contexts, reinforcing students for generalizing information across material or settings, reminding students to apply information they have learned in one setting to another, and teaching information in multiple settings (Kerig & Wenar, 2006). Our findings indicate that the Co-PID program, which applied reinforcement for generalization and was taught in the classroom, had a significant internal effect on the students, expressed in a change of behavior (enhanced participation) outside the classroom.
In summary, the current study further corroborated the Co-PID program as an effective model for enhancing participation of students with moderate IDD. Students demonstrated enhanced participation not only during lessons but also in additional environments outside the classroom.
Limitations
The main limitation of this study was the gap in intervention duration between groups. The IS program was structured to resemble a common IS program in the school system. An additional limitation is the relatively low internal consistency of the subcomponents of the SOSPiC, although the entire measure has very good reliability. This outcome may have somewhat affected the division of the three areas of participation. However, because no other outcome measures for the examination of participation in classroom-related activities were found, these initial measures provide moderately accurate information. Yet, it is clear that further studies relating to the SOSPiC are required. Finally, in future studies, researchers should triangulate the findings by using additional measures such as observations.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
The collaborative consultation model combined with in-service was found to be effective in facilitating participation in classroom-related activities among students with moderate IDD.
Service delivery by occupational therapists using collaborative consultation within a school setting supported teachers in execution of strategies to enhance students’ participation.
After the Co-PID intervention, students’ improved participation transferred to other environments beyond the classroom.
Conclusion
Participation plays an important role in one’s personal well-being and quality of life. Our study adds to the limited body of knowledge on participation among students with moderate IDD. The collaboration between homeroom teachers and an occupational therapist, within this ecological model, was successfully implemented. The Co-PID will enhance participation in these students in the classroom and in all environments. In future studies, researchers should further examine implementation of the program in large-scale settings.
Footnotes
Acknowledgments
This work was supported by the Chief Scientist’s Office, Ministry of Education, Jerusalem, Israel. The authors thank all the teachers and students who participated in the study.