
Abstract
State governments in the United States have been providing services for people with intellectual and developmental disabilities (IDDs) for more than 160 yr, the majority of which have been provided in large state-operated institutions (Braddock et al., 2015). Initially, Medicaid funding, which was launched in the 1960s, was available to people with disabilities, including those with IDDs, only when institutionalized, leading to a widespread expansion of large state-run institutional long-term care facilities. Through the work of advocates, amendments to Medicaid, and rulings such as Olmstead v. L.C. (1999), this institutional bias has slowly eroded, with states now able to provide Medicaid funding to people in community-based settings (Smith et al., 2000).
Before these changes, occupational therapy practitioners treating people with IDDs did so within the confines of medical facilities and in-unit settings (Nehring & Lindsey, 2016) with little to no intervention design addressing community integration and participation. With the shift to community living, occupational therapy practitioners are now using their clinical expertise to identify and develop the skills and abilities of people with IDDs and the supports and modifications necessary to promote optimal integration and participation in the community (Hammel, Lai, & Heller, 2002). Occupational therapy services that promote community living include the design and implementation of activity of daily living (ADL) and instrumental ADL training, pre- and vocational training, community integration programs, environmental interventions, and caregiver training programs (Hammel et al., 2008; Ideishi, D’Amico, & Jirikowic, 2013). The foundation for these services is grounded within the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; American Occupational Therapy Association [AOTA], 2014), which identifies that occupational therapy works to facilitate, promote, and achieve increased occupational engagement in client-centered meaningful ADLs (Mahoney, Roberts, Bryze, & Parker Kent, 2015).
Medicaid Home and Community-Based Services
Each state’s Medicaid state plan covers federally mandated basic immediate medical care, such as in-patient hospitalization services, short-term skilled nursing or rehabilitation, and doctor services by approved providers. However, many services can vary; for example, dental coverage is not included in many state plans (Friedman, Rizzolo, & Schindler, 2014). Basic occupational therapy services are provided by all states in their Medicaid state plans (AOTA, n.d.). States also have the option of providing additional occupational therapy services through Medicaid’s funding mechanisms for long-term services and supports (LTSS), which include care provided within institutional care settings—such as intermediate care facilities—and funding for Home and Community-Based Services (HCBS).
Established by Congress in 1981, the HCBS waiver program allows states to direct resources to vulnerable populations. HCBS waivers function by allowing states to waive the main provisions of the Social Security Act of 1935 that previously required institutional-based service provision; HCBS waivers instead allow states to provide specialized services permitting people to remain in their own home or live in a community setting (Smith et al., 2000).
The HCBS waiver aims to increase the potential for successful community living, rather than segregated institutional care, for people with IDDs through community-based services and supports (Rizzolo, Friedman, Lulinski-Norris, & Braddock, 2013). In large part because of the HCBS waiver program, the United States has seen a major shift to community living for people with IDDs, with a 70% decrease in institutional living between 1977 and 2007 (Spassiani, Parker Harris, & Hammel, 2016). Today, HCBS waivers are one of the largest providers of LTSS for people with IDDs because of their cost-effectiveness, their improved community outcomes, and the preferences of people with IDDs (Braddock et al., 2015; Rizzolo et al., 2013).
One intricacy of the HCBS waiver program is that states can tailor HCBS waivers as they see fit; as a result, there is often large variance across states and waivers in terms of what types of services are provided (Rizzolo et al., 2013). Therefore, how occupational therapy is incorporated into HCBS waivers may be dependent on the presumed value or benefit of occupational therapy interventions on the long-term health outcomes of people with IDDs. Yet, occupational therapy has many documented benefits for people with IDDs. For example, research has found that occupational therapy–designed interventions incorporating client motivation, choice, and meaningful activity result in increased community and social engagement for people with IDDs (Mahoney et al., 2015). Occupational therapy services can also facilitate and enable meaningful participation through interventions that enrich the environmental context and support adaptive behaviors increasing occupational engagement (Channon, 2014; Shikako-Thomas, Majnemer, Law, & Lach, 2008).
Little research has examined how occupational therapy is used through Medicaid LTSS HCBS programs. Comparison across states can inform the occupational therapy profession on potential areas for greater emphasis in research, need for program development, and future policy efforts. Thus, the aim of this study was to determine how Medicaid HCBS 1915(c) waivers for people with IDDs allocate occupational therapy services across the nation. To do so, we analyzed HCBS waivers for people with IDDs providing occupational therapy services in Fiscal Year (FY) 2015 to determine service utilization and projected expenditures. We also compared service definitions to determine trends.
Method
Medicaid HCBS 1915(c) waivers were obtained from the Centers for Medicare and Medicaid Services (CMS) Medicaid.gov website (https://www.medicaid.gov/) between June 2015 and April 2016. For waivers to be included in the analysis, they were required to be 1915(c) and to serve only people with IDDs—intellectual disability (ID), developmental disability (DD), mental retardation (MR), 1 and autism (no age limitations were imposed). Waivers also needed to include 2015; to do so, we used the waiver year that aligned closest with FY 2015 (July 1, 2014–June 30, 2015). Most often this was the state FY; however, a few states used the 2015 calendar year or the federal FY (October 1, 2014–September 30, 2015). The term FY is used for consistency. This process resulted in the collection of 111 FY 2015 HCBS waivers for people with IDDs from 46 states and the District of Columbia.
CMS requires waivers to describe CMS assurances and requirements; levels of care; waiver administration and operation; participant access and eligibility; participant services, including limitations and restrictions; service planning and delivery; participant direction of services; participant rights; participant safeguards; quality improvement strategies; financial accountability; and cost-neutrality demonstrations. We used this information to organize HCBS IDD waiver services into a taxonomy mirroring Rizzolo et al.’s (2013) FY 2010 HCBS IDD waiver taxonomy. Doing so allowed us to explore occupational therapy services in depth.
We used the waivers’ “Appendix J: Cost Neutrality Demonstration” sections to analyze occupational therapy service expenditures and utilization. In this section, states are required to demonstrate that waiver spending does not exceed institutional spending for similar levels of care. As such, states must note unduplicated number of participants using services, units of service provided to these participants, and expected average unit cost. Via Excel (Microsoft Corp., Redmond, WA), we used descriptive statistics to determine occupational therapy service allotment across waivers and states, including total projected spending, projected spending per participant, reimbursement rates, and annual service provisions per participant. (It should be noted that four services were excluded from the analysis of service expenditures because occupational therapy was provided within another service, such as “physical health” or “specialized consultative services.” Thus, it could not be determined how much spending was allocated for occupational therapy in these services.)
Service definitions were gathered from the “Appendix C: Participant Services” section of each waiver. Occupational therapy service definitions (see Supplemental Table 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) were then qualitatively analyzed by one of the researchers using content analysis (Patton, 2002) to determine trends across FY 2015 services.
Results
Forty-three waivers (38.7%) from 21 states and the District of Columbia provided 63 occupational therapy services in FY 2015.
Service Definitions
Occupational therapy services were generally described similarly to the Alabama ID waiver’s description of its occupational therapy service:
the application of occupation-oriented or goal-oriented activity to achieve optimum functioning, to prevent dysfunction, and to promote health. The term occupational as used in occupational therapy refers to any activity engaged in for evaluation, specifying, and treating problems interfering with functional performances. Services include assisting in the evaluation of an individual to determine level of functioning by applying diagnostic and prognostic tasks and guiding and treating individuals in the prescribed therapy to secure and/or obtain necessary functioning. Provision of this service will prevent institutional placement. (State of Alabama, n.d.)
Because states could customize their service definitions as they saw fit, the majority of services (n = 52) described the ways in which waiver services were different from the occupational therapy services provided in their Medicaid state plans. Approximately half of services (n = 31) explained that occupational therapy waiver services provided long-term care rather than the immediate care provided in state plans. For example, West Virginia’s MR/DD waiver explained that “services provided under the Waiver are for chronic conditions and maintenance while the occupational therapy services furnished under the State plan are short-term and restorative in nature” (State of West Virginia, n.d.).
Many states also used HCBS waivers to provide occupational therapy services in alternative settings, such as in the community or in the participant’s home (n = 29 waivers). For example, Washington’s Children’s Intensive In-Home Behavioral Support (CIIBS) Waiver detailed that
an example of the need for [occupational therapy] as a waiver service would be to allow the therapy to be provided in the family home. State plan services are provided in clinical settings, and few providers are willing to come into the home to provide service. Children on the CIIBS waiver often require or benefit more from therapy provided in the home with the inclusion of family members because of high anxiety and challenging behavior that prevents them from accessing the clinical setting. In-home services offer the additional benefits of the natural environment, which allows therapy to be incorporated into regular child and family routines. (State of Washington, n.d.)
Still other states provided occupational therapy services in their waivers more generally, stating that they provided services that were otherwise not covered by state plans (n = 11). Some states also provided occupational therapy services in their waivers for when state plan occupational therapy coverage was exhausted (n = 9). Montana used its three waiver programs to provide occupational therapy services to adults who were older than age 21 because their state plan only covered those under 21.
Finally, several states used waiver occupational therapy services to train direct care staff and caregivers to best support the participant with IDDs in addition to providing services to the participant with IDDs (n = 25). For example, Kentucky’s Supports for Community Living waiver (which has been replaced with a new waiver since this article was written) noted that
these services address the occupational therapy needs of the participant that result from his or her developmental disability as well as development of a home treatment/support plan with training and technical assistance provided onsite to improve the ability of paid and unpaid caregivers to carry out therapeutic interventions. (State of Kentucky, n.d.)
Service Expenditures
In FY 2015, a total of $14.13 million was projected for occupational therapy services for approximately 7,500 participants (see Supplemental Table 2). Whereas the average waiver projected spending $227,968 (median = $39,453), total projected spending varied widely across services, ranging from $18.62 for Indiana Family Supports waiver’s “OT” service (1 participant) to $2,964,748 for New Mexico Developmental Disabilities Waiver Program’s “OT, Standard (New)” service (1,231 participants). The average spending per capita was $0.18. Table 1 details projected spending and spending per capita by state.
Occupational Therapy Services for People With IDDs in Medicaid HCBS Waivers (Fiscal Year 2015) by State
Note. HCBS = Home and Community-Based Services; IDDs = intellectual and developmental disabilities.
An average of $1,558 was projected per participant for occupational therapy services in FY 2015. The median was $1,344. Projected spending per participant ranged from $18.62 (Indiana Family Supports waiver’s “OT” service) to $5,107 (Texas Deaf Blind with Multiple Disabilities waiver’s “OT” service; Figure 1).
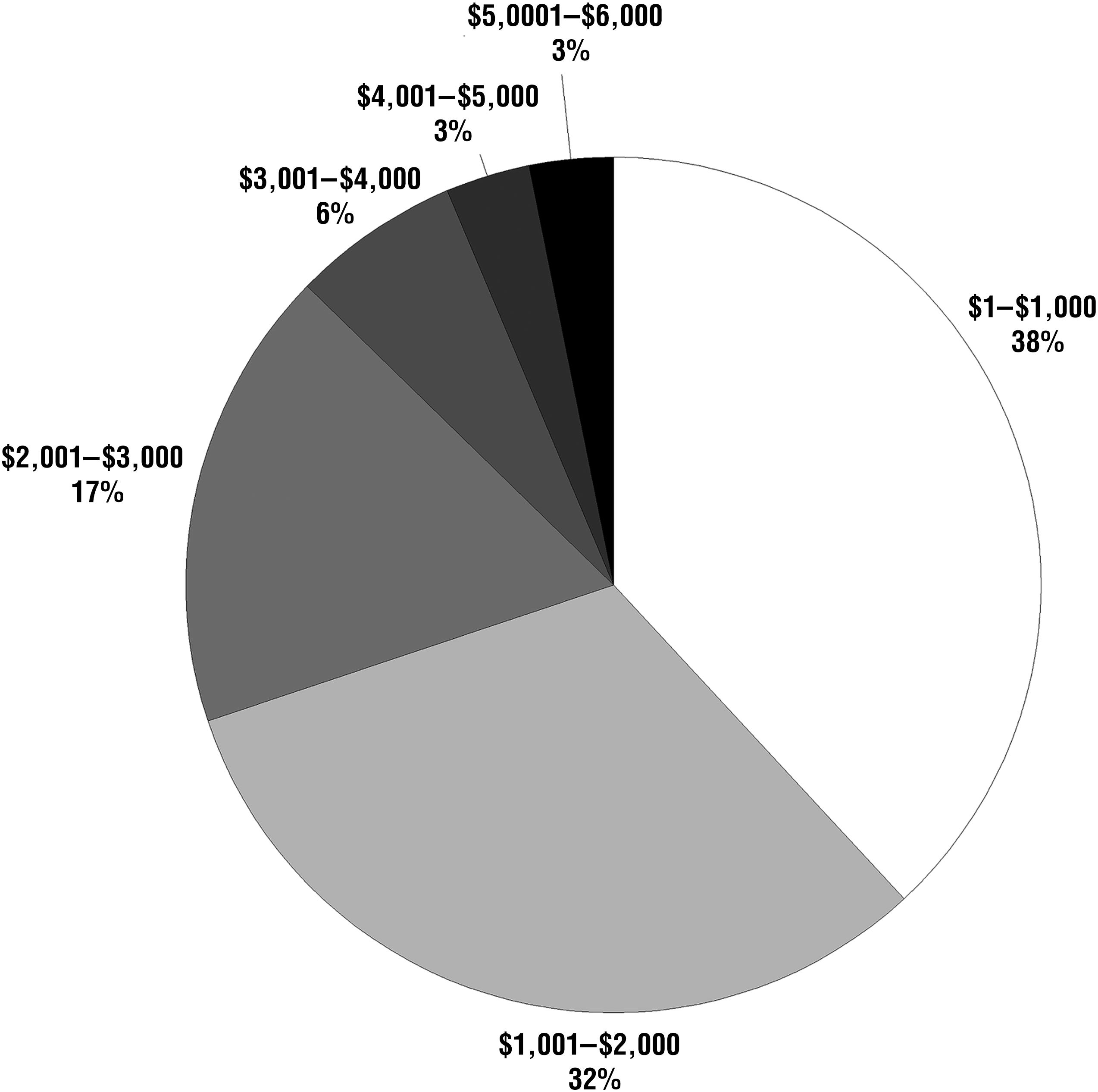
Average projected spending per participant.
Reimbursement Rates.
Occupational therapy services were reimbursed by several different rates, including 15-min, hourly, daily, and session (i.e., each visit, session, procedure). Thirty-eight services provided occupational therapy by a 15-min reimbursement rate. Whereas the average 15-min reimbursement rate was $18.29 with a median of $18.13, it ranged from $9.54 per 15 min (New Mexico Developmental Disabilities Waiver Program’s “OT, Incentive [New]” service) to $30.68 per 15 min (New Mexico Developmental Disabilities Waiver Program’s “OT Assistant [Certified], Exception [Old]” service). Figure 2 details trends across 15-min rates in more detail.
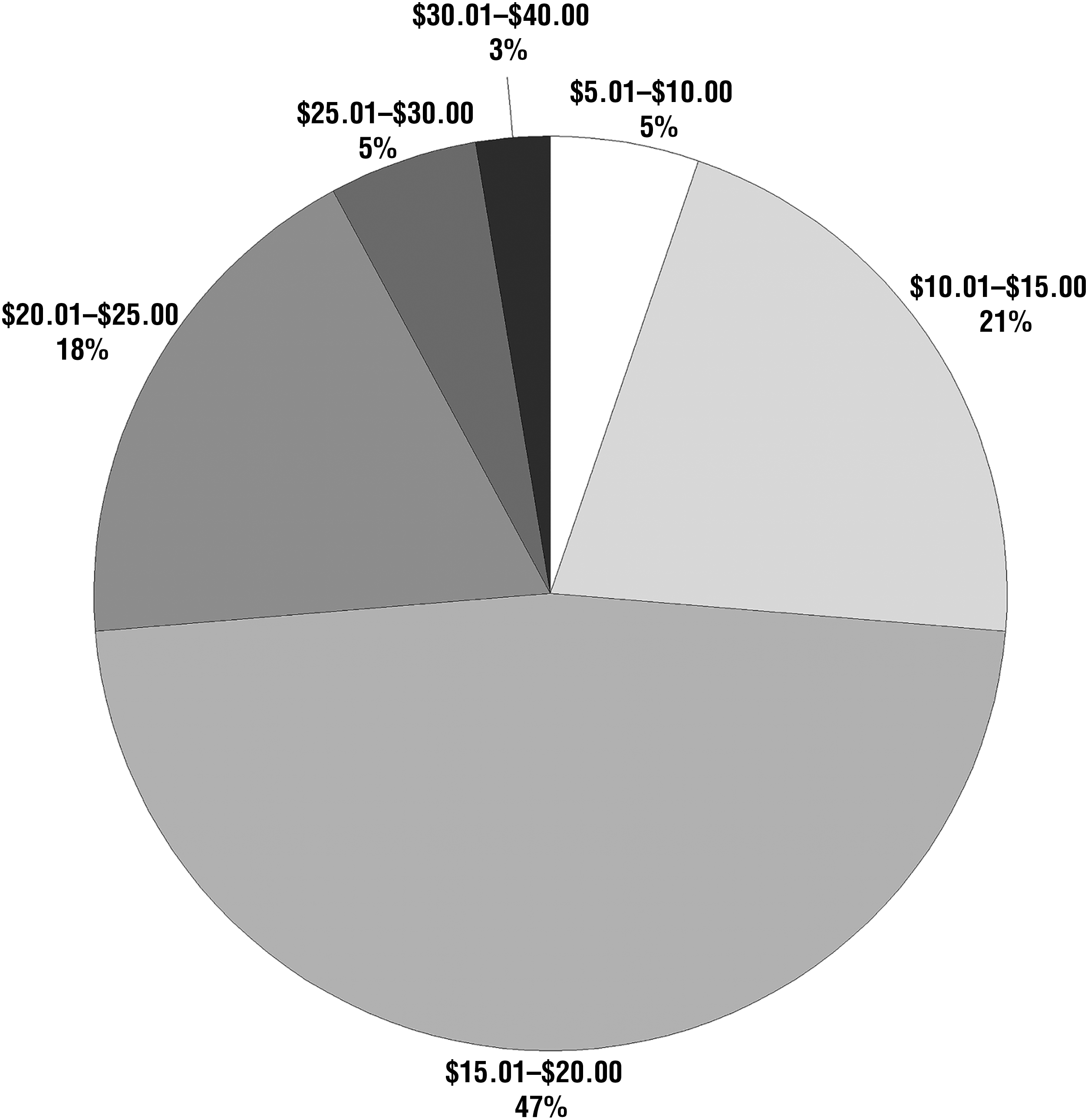
Reimbursement rates for 15-min rate services.
Of those services reimbursed by an hourly rate (n = 13), the hourly rate ranged from $15.61 (Washington Core Waiver’s “OT” service) to $85.75 (Montana Children’s Autism Waiver’s “OT” service) per hour. The average hourly rate was $59.52, and the median was $71.95. Of hourly rate services, 15.4% (n = 2) reimbursed at a rate between $0 and $25, 15.4% (n = 2) between $26 and $50, 53.8% (n = 7) between $51 and $75, and 15.4% (n = 2) between $76 and $100.
For those services that reimbursed by session (n = 8), the average rate was $104.88 per session, median of $73.41, ranging from $15.96 per session (Wyoming Comprehensive Waiver’s “OT” service) to $453.48 per session (New Mexico Developmental Disabilities Waiver Program’s “OT, Evaluation [New]” service). Of session rate services, 12.5% (n = 1) reimbursed at a rate between $0 and $25, 25% (n = 2) between $26 and $50, 37.5% (n = 3) between $51 and $75, 12.5% (n = 1) between $76 and $100, and 12.5% (n = 1) more than $101.
Three services were provided by daily rate, averaging $307.47 per day with a median of $312.00. Tennessee Self-Determination Waiver Program’s “OT: Assessment and Plan Development” service reimbursed at $292.32 per day, Tennessee Comprehensive Aggregate Cap Waiver’s “OT: Assessment and Plan Development” service reimbursed at $312.00 per day, and Tennessee Statewide Waiver’s “OT: Assessment and Plan Development” service reimbursed at $318.10 per day.
Annual Service Provision.
The amount of occupational therapy services that participants received in a year also ranged depending on the services and reimbursement types. The 15-min rate services provided an average of 101.51 15-min blocks of occupational therapy services per year to each participant (median = 97.95), ranging from one 15-min block (Indiana Family Supports waiver’s “OT” service) to 304 15-min blocks (Florida DD Individual Budgeting Waiver’s “OT: Service”; Figure 3).
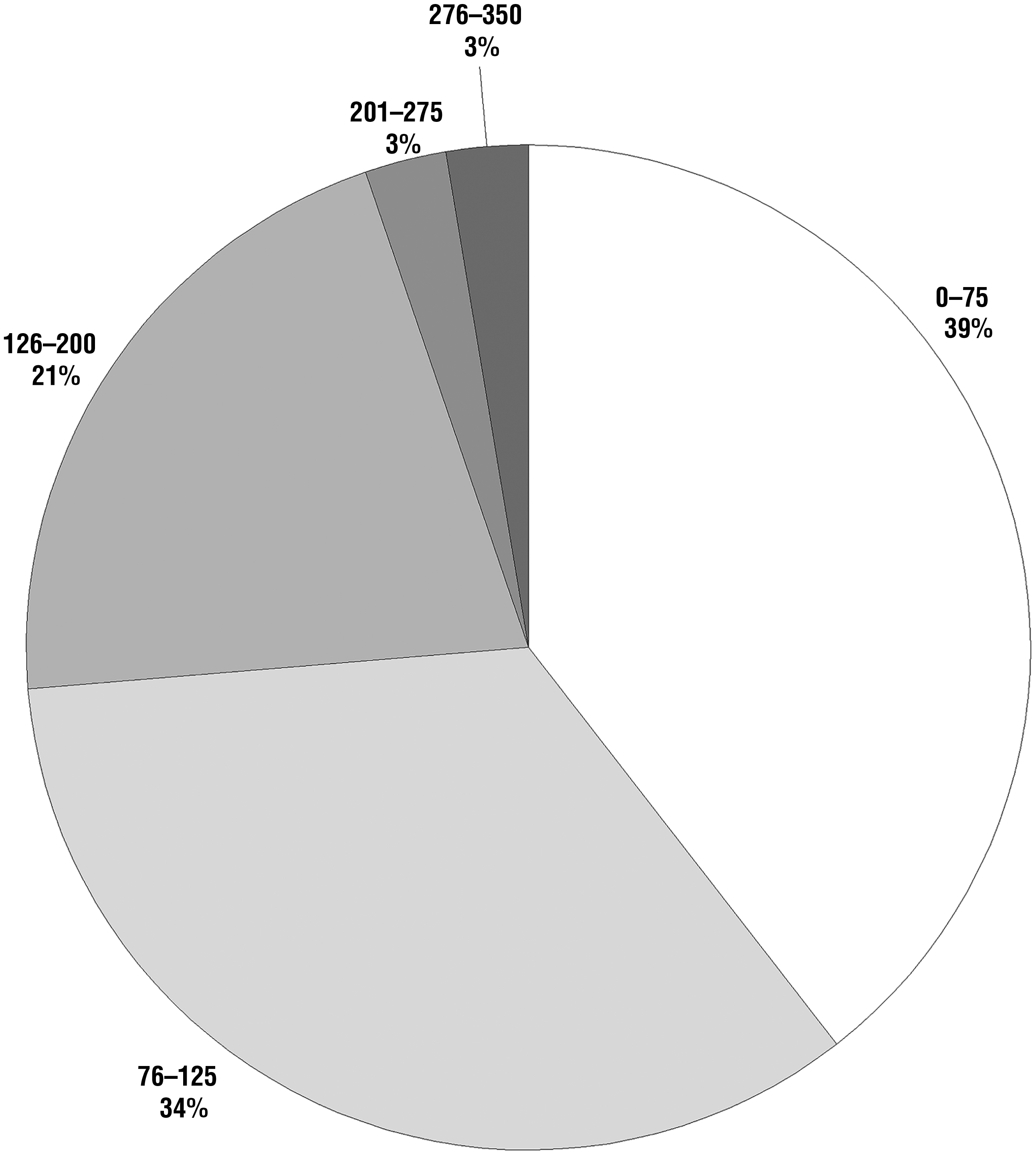
Average annual service provision per participant for 15-min rate services.
Hourly rate services provided on average 25.78 hr of occupational therapy services per year (median = 18), ranging from 1 hr per year (Oregon ICF/IDD Comprehensive Waiver’s “OT Services”) to 70 hr per year (Texas Developmental Disabilities waiver’s “OT” service). Of hourly rate services, 38.5% (n = 5) provided the average participant between 0 and 10 hr of occupational therapy per year, 15.4% (n = 2) between 11 and 20, 7.7% (n = 1) between 21 and 30, 7.7% (n = 1) between 31 and 40, 7.7% (n = 1) between 51 and 60, and 23.1% (n = 3) between 61 and 70.
On average, participants receiving services provided by session were projected to receive 26 sessions of services per year (median = 13.50), ranging from 1 session (New Mexico Developmental Disabilities Waiver Program’s “OT, Evaluation [New]” service) to 70 sessions (Wyoming Comprehensive Waiver’s “OT Group”). Of session rate services, 37.5% (n = 3) provided the average participant between 0 and 10 sessions per year, 25% (n = 2) between 11 and 20 sessions, 25% (n = 2) between 41 and 50 sessions, and 12.5% (n = 1) between 61 and 70 sessions. Finally, all three daily rate services—“OT: Assessment and Plan Development”—provided 1 day of occupational therapy services per year.
Discussion
Analysis of 111 Medicaid HCBS 1915(c) waivers for people with IDDs revealed that 43 waivers provided occupational therapy services in FY 2015. States used HCBS waivers to provide occupational therapy services in different ways from their Medicaid state plans. Often states included occupational therapy in waivers to provide continuous long-term care and to improve participants’ abilities to complete ADLs, rather than the short-term immediate care provided by state plans. HCBS waiver occupational therapy coverage was also used to extend exhausted state plan services and to provide occupational therapy services outside of traditional clinical settings, such as in the community and participants’ homes.
In FY 2015, $14.13 million of spending was projected for occupational therapy services, which is less than 0.1% of FY 2015 spending (Friedman, 2017). HCBS waivers provided less than 1.2% of its 630,000 recipients with occupational therapy services in FY 2015 (Friedman, 2017). Moreover, our findings also revealed large variability across states and services in terms of occupational therapy service provision. In addition to total projected spending, projected spending per participant, service provisions per participants per year, and reimbursement rates all ranged significantly across waivers. For example, spending per participant ranged from $18.62 to $5,107. There were also significant differences across reimbursement rates, which ranged from $9.54 to $30.68 for 15-min rates, from $15.61 to $85.75 for hourly rates, and from $15.96 to $453.48 for session rates. Although striking, and potentially problematic, this wide variance is not uncommon among HCBS IDD waivers (Friedman, 2017; Rizzolo et al., 2013). The ability to customize HCBS waivers allows states large flexibility in terms of how they provide occupational therapy services.
Future Research
Our findings of wide variance across states and services suggest many fruitful avenues for future study. For example, what factors influenced the decisions to limit service provision? How had local or national occupational therapy associations worked to influence those states that provided the highest rates and service provision? Are states including occupational therapy professionals in the development and implementation of processes for referral, assessment, and interventions? Waiver decisions affect clients’ ability to access services vital to achieving and maintaining full participation in society. With state fiscal challenges, future researchers should also evaluate occupational therapy maintenance care waiver services because of their impact on reducing acute hospitalization, preventing and reducing the onset of secondary conditions, and lessening the incidence of costly institutionalized care.
Occupational therapy practitioners working with clients on IDD waivers have reported reimbursement rates less than half of usual fees and systemic procedural complexities that significantly delay reimbursement (D. Davidson, personal communication, August 13, 2016). Research is needed to identify barriers and supports regarding occupational therapy practitioners’ experiences with waivers to streamline this process. For example, how do occupational therapy practitioners working with limited service time target their interventions? Most important, how and in what way do occupational therapy services affect the lives of people with IDDs in achieving the goals of the waiver—successful living in the community? Comparisons across states can be used to examine these questions, which can then strengthen the profession’s ability to assert the value of its services.
Limitations
One limitation of our study should be noted. Medicaid HCBS waivers are state projections made to the federal government instead of utilization data. However, previous research by Rizzolo et al. (2013) found them to be reasonably accurate proxies of waiver services because they are based on previous years’ waiver utilization. In fact, Rizzolo et al.’s waiver projections were congruent with previous utilization analyses by Braddock et al. (2015). Another limitation was that only one researcher coded the qualitative data; therefore, there was not a second coder for reliability.
Implications for Occupational Therapy Practice
Examining occupational therapy services within the Medicaid HCBS 1915(c) waiver data provides an opportunity to generate new knowledge for the profession in its current and future role in community-living waiver programs for people with IDD. The findings of this study have the following implications for occupational therapy practice:
Providing an opportunity for analysis of shifts and trends in occupational therapy services in LTSS within community settings as a platform for needs assessment research
Providing quantitative data to support professional state lobbying efforts to retain or implement occupational therapy services within HCBS 1915(c) waivers
Exploring successful state models of service provision for best practices of occupational therapy in HCBS waivers.
Conclusion
It is critical for the profession to be able to document how occupational therapy services contribute to lower long-term care spending and improved client and caregiver outcomes (Grabowski, 2006). To describe the profession’s overall value in health care provision, occupational therapy practitioners must focus outcome research on occupational therapy’s role in increasing efficiency within the system of care as they reduce overall costs (Lamb & Metzler, 2014). It is imperative that the profession continues research that contributes to the value-base of the services provided to support advocacy for a viable continuance of community services for people with IDDs. Occupational therapy research indicates that LTSS positively influence the lives of people with IDDs (Siporin & Lysack, 2004). However, the profession must also provide evidence of occupational therapy’s role in reducing health care costs despite initial upstream increases in payment because this research may influence policy decisions to exclude or reduce occupational therapy services (Grabowski, 2006). We believe that the findings of this study can be used to help identify best practices and to advocate for the development and refinement of state occupational therapy programs.
The HCBS 1915(c) waiver program and the profession of occupational therapy share common goals for the clients they serve—preventing and overcoming obstacles to living and participating in the community through increasing services and supports (Collins & Strzelecki, 2006). Despite the needs of people with IDDs, only 39% of state waivers provided occupational therapy services in FY 2015. The occupational therapy profession needs to translate the value of occupational therapy services to waivers by demonstrating that inclusion of occupational therapy improves outcomes and reduces costs. Doing so requires simultaneously advocating for the profession and clients so that they may optimize community participation.
Supplemental Material
Supplementary material for Occupational Therapy in Medicaid Home and Community-Based Services Waivers
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.024273.pdf for Occupational Therapy in Medicaid Home and Community-Based Services Waivers by Carli Friedman and Laura VanPuymbrouck in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This article was sponsored in part by U.S. Department of Health and Human Services, Administration for Community Living (ACL) Grant 90DN0296 and ACL National Institute on Disability, Independent Living, and Rehabilitation Research Grant 90RT5007-02-02. The content is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. Department of Health and Human Services; endorsement by the federal government should not be assumed.
1
Although outdated, this term continues to be used by some waivers and therefore was a necessary search term (Friedman, 2016).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.