
Abstract
Handwriting difficulties can have serious ramifications on children’s academic achievement, school participation, self-esteem, and overall well-being (Engel-Yegeret et al., 2009; Feder & Majnemer, 2007). The prevalence of schoolchildren with dysgraphia is high, with estimates varying from 10% to 30% (Cermak & Bissell, 2014; Karlsdottir & Stefansson, 2002). These children often experience repeated failures, may perceive themselves as unable to improve their skills, and simply give up (Rosenblum et al., 2003). As a result, they may develop an avoidance of writing, coupled with numerous negative academic and psychosocial consequences, such as getting poorer grades, being mislabeled as lazy, and having reduced self-esteem (Weintraub et al., 2009). Therefore, it is not surprising that handwriting remediation is a common area of pediatric occupational therapy practice (Giroux et al., 2012; Hoy et al., 2011).
Client-Centered Practice
The client-centered occupational therapy approach supports the active involvement of clients in the therapy process by considering their personal assessment of their abilities and encouraging their participation in selecting therapy goals (Hammell, 2013). The use of client-centered approaches and tools to enhance clients’ role in their care has been advocated by professionals in a variety of health care disciplines as a means of contributing to the effectiveness and quality of intervention outcomes (Verma et al., 2006). However, when the client is a child, intervention goals are often prescribed by their occupational therapists, parents, caregivers, or teachers. This approach is problematic because goals established for children by others are much less motivating than those selected by children themselves (Josman & Rosenblum, 2011; Majnemer, 2011; Missiuna et al., 2006; Tatla, 2014). Hence, children with handwriting difficulties are not always sufficiently engaged in the intervention process.
Engagement in the intervention process encourages children to work, reflect, and talk about their learning at cognitive, affective, and operative levels (Woodward & Munns, 2003). Therefore, they feel more in control of their learning, have opportunities to direct their own learning process (Kobus et al., 2007), and become more invested in their occupational role as students. Fearing and colleagues (1997) described clients’ active engagement in identifying their problems and collaborating in intervention as a fundamental part of the client-centered approach. However, occupational therapists often find it difficult to elicit self-appraisals and client-centered goals from young clients (Pollock et al., 2010). Thus, tools that facilitate children’s self-assessment and goal setting may elicit powerful and enduring levels of their engagement in the learning environment (HaLevi, 2009; Missiuna et al., 2006; Schunk, 1985).
Self-Awareness
Self-awareness is an important component of metacognition that is positively linked to learning outcomes. Not only does it involve cognition, but it also interweaves cognitive and affective components, including motivation, to stimulate effort and persistence toward fulfilling one’s goals in the face of obstacles (Efklides, 2009). Self-awareness of their strengths and limitations enables people to manage their difficulties by setting attainable goals, monitoring their progress, and reflecting on their increasing effectiveness and achievements. This process elicits enhanced self-esteem and the motivation needed to work toward improving their skills (Zimmerman, 2002). Self-perception of one’s abilities may also foster the use of learning strategies, contributing to one’s efficacy in striving toward learning goals (Pajares, 2009).
Comparing clients’ self-ratings with clinicians’ ratings of their abilities or performance on objective performance measures is a commonly used method of assessing self-awareness in occupational therapy (Lahav et al., 2014). Disparity between self-ratings and ratings by others or test performance is considered to be a measure of unawareness (Hoza et al., 2012). An instrument that can inform occupational therapy practitioners about children’s perceptions regarding their handwriting abilities would be valuable in helping practitioners develop intervention approaches that are meaningful to their clients (Cermak & Bissell, 2014; Keller & Kielhofner, 2005). This type of instrument could also be used in research to expand the available body of knowledge on the awareness of children with and without dysgraphia regarding their handwriting abilities. However, this component is often missing in formal handwriting assessments and intervention (Cermak & Bissell, 2014).
Engel-Yeger and colleagues (2009) recognized the need for and developed a self-report handwriting questionnaire (i.e., Children’s Questionnaire for Handwriting Proficiency). They found that second- and third-grade children with proficient handwriting perceived their writing competence to be better than their peers with handwriting difficulties. Josman and Rosenblum (2011) also developed a handwriting awareness questionnaire for children, adapted from the Contextual Memory Test (Toglia, 1993). They found that improvement in children’s handwriting awareness was related to improvement in their handwriting skills after intervention.
Here’s How I Write–Hebrew (HHIW–HE; Goldstand et al., 2013), originally published as Kach Ani Kotev (Goldstand & Gevir, 2009, 2012), is an innovative pictorially based Hebrew-language self-assessment and goal-setting tool for children in Grades 2–5 created to promote client-centered intervention for schoolchildren with dysgraphia. A pilot study by HaLevi (2009) on the HHIW–HE was conducted, and the findings supported its utility and feasibility. HaLevi also reported that the tool facilitated children’s engagement in the therapeutic process and reported it to be a “fun” process. Goldstand and colleagues (2013) developed and adapted an English-language version of the tool modeled after the original Hebrew-language tool. Both versions are designed to help children identify their handwriting strengths and weaknesses and select treatment goals in a child-friendly and motivating manner (Cermak & Bissell, 2014; Goldstand & Gevir, 2012). The content validity of the English version was supported through an expert-validation process (i.e., all items achieved ≥80% agreement among handwriting experts; see Ayre & Scally, 2014). Known-groups validity was supported by the statistically significant differences found between the self-ratings of children with proficient and poor handwriting (Cermak & Bissell, 2014). The objectives of our study were to investigate the psychometric properties of the HHIW–HE and to compare the self-awareness of handwriting abilities between schoolchildren with and without dysgraphia.
Method
Participants
Participants comprised a convenience sample of 58 Israeli children in Grades 2–5 attending a mainstream educational program in central Israel. They included 44 boys (75.9%) and 14 girls (24.1%) between the ages of 7.1 and 10.10 yr (mean [M] age = 8.4 yr, standard deviation [SD] = 0.87). Participants with dysgraphia were recruited by 10 pediatric occupational therapists experienced in handwriting intervention from their area of residence. The therapists evaluated the handwriting of children referred to them by teachers or parents. They identified 29 children with dysgraphia based on scores ≥15 on the Brief Assessment Tool for Handwriting (BATH; Lifshitz & Parush, 1999) and scores ≥1 SD below the mean scores on the Hebrew Handwriting Evaluation (HHE; Erez & Parush, 1999), an objective, standardized Hebrew handwriting evaluation. The control group (n = 29) was matched on age range and gender and determined to be proficient at handwriting (BATH scores below the cutoff [M = 7.41, SD = 3.17], and normative performance on the HHE) by the third author (Renana Yefet). Exclusion criteria for both groups were significant neurological and primary sensory impairments or chronic diseases.
Instruments
The BATH is a 16-item questionnaire designed by expert occupational therapists to identify schoolchildren with handwriting difficulties. It is completed by an occupational therapist familiar with the child or by the child’s teacher. It encompasses aspects of handwriting function including legibility, the writing process and performance, and questions targeting the emotional aspects of writing. Each item is rated on a 4-point Likert scale ranging from 0 (never) to 3 (always), with higher scores indicating poorer performance. The total score ranges from 0 to 64, and the cutoff score for the existence of handwriting problems is 15. The tool underwent an expert-validation process, and the final items were selected based on ≥80% agreement between 14 handwriting experts. Internal reliability is high (α = .9). The validation process included significant correlations between scores on the BATH and the HHE (r = .46–.65, p < .01), and significant differences between the scores of children with and without dysgraphia (n = 189), t(58) = 20.78, p = .00, supporting its known-group validity (Lifshitz & Parush, 1999).
HHIW–HE is a pictorial self-assessment and goal-setting tool for children in Grades 2–5 designed to help children evaluate their handwriting strengths and weaknesses and to determine, together with an occupational therapist, their handwriting intervention goals. The tool consists of 24 item cards plus 1 demonstration card (i.e., totaling 25 cards) and a goal-setting form. One side of each card contains a statement and matching picture depicting a child with proficiency regarding a certain aspect of handwriting. The card’s flip side contains a statement and a picture depicting a child with difficulty regarding that same aspect of handwriting (Figure 1). For each of the 24 cards, the examiner shows the child both sides and then asks the child, “Which is more like you?” The child responds by selecting a side (positive vs. negative handwriting attribute) and then qualifies his or her response as “all of the time” or “some of the time.” A negative handwriting attribute is scored as either 4 points (all of the time) or 3 points (some of the time). A positive handwriting attribute is scored as either 2 points (some of the time) or 1 point (all of the time). The total scores range from 24 to 96, with lower total scores indicating more positive self-perceptions of handwriting abilities than higher total scores.
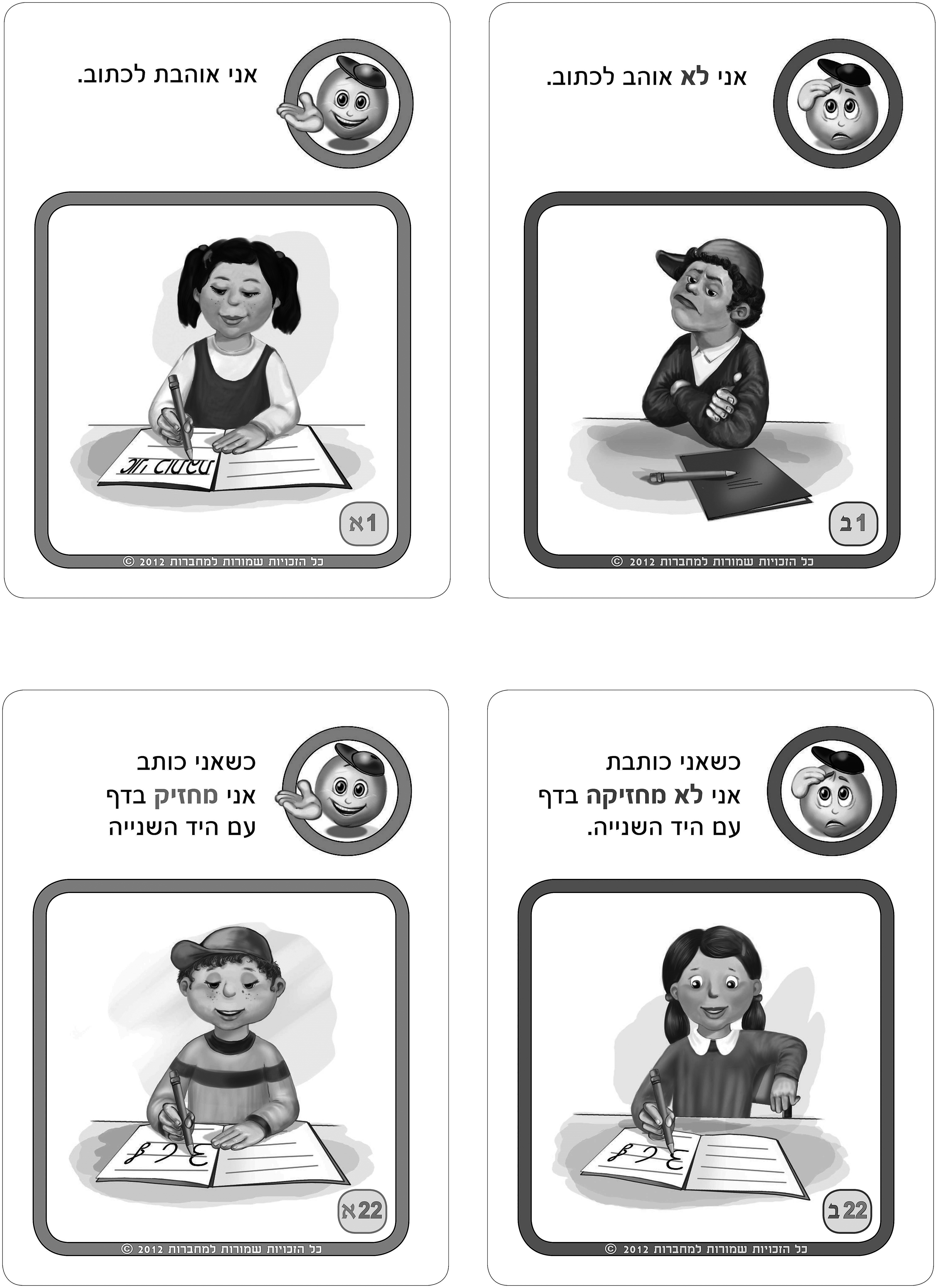
Sample cards from Here’s How I Write–Hebrew: A Child’s Self-Assessment of Handwriting and Goal Setting Tool.
The HHIW–HE is administered after the child and therapist have established a therapeutic relationship, the child’s teacher reports on his or her perceptions of the child’s handwriting, and a formal handwriting evaluation is administered. After the self-assessment stage of the HHIW–HE process, the therapist helps the child define his or her treatment goals in a child-centered manner (Goldstand & Gevir, 2012).
Content validity was supported by the results of an expert-validation process involving nine experienced pediatric occupational therapists with a minimum of 10 yr of expertise in handwriting intervention. The final items were selected on the basis of 80%–90% agreement among the experts (Ayre & Scally, 2014). In a pilot study, HaLevi (2009) found 75%–80% agreement between children’s responses on the HHIW–HE and therapist scores on the HHE (Erez & Parush, 1999) among 10 Israeli children (ages 7.5–10.3 yr, M = 8.5) with handwriting difficulties attending a regular education program. These findings support the ability of typical children in this age range to self-report on their handwriting ability. In addition, the HHIW–HE test–retest reliability was performed over a 2-wk interval with 14 members of the control group and was been found to be acceptable (r = .65–1.00, p < .05; Yefet, 2012).
Procedure
After obtaining approval from the Hebrew University ethics committee, the researchers contacted 10 pediatric occupational therapists (≥8 yr of experience) from central Israel to recruit participants for the research group. Control group participants were recruited with a snowball procedure and matched to the research group according to age range and gender. Consenting parents of both study groups signed an informed consent, and the children provided assent. The BATH and the HHE copy task were administered to the control group to confirm handwriting proficiency, and the children were then rated on the HHIW–HE items on the basis of the objective assessment results. The recruiting therapists identified children with dysgraphia based on the BATH and HHE scores. The third author (Renana Yefet) reviewed the administration protocol delineated in the HHIW–HE manual (Goldstand & Gevir, 2009) with the therapists, after which they scored 21 of 24 of the HHIW–HE items (excluding 3 items relating to children’s feelings about handwriting, such as “I like to write”). Next, all participants completed the HHIW–HE, and the scores of the research and control groups were compared to determine the tool’s known-group validity.
Data Analyses
Statistical analyses were conducted using IBM SPSS Statistics (Version 19; IBM Corp., Armonk, NY). Given the non-normal distribution of the HHIW–HE scores, nonparametric statistical analyses were conducted. Independent samples Mann–Whitney U test was used to compare the total score and the 24 item scores of the HHIW–HE between the study groups; the Bonferroni correction for multiple comparisons was then used (p = .05 for the 24 cards). Internal consistency was computed using Cronbach’s α. Nonparametric effect size r was computed for between-group comparisons (Fritz et al., 2012).
The construct of self-awareness was operationally defined as the percentage of child–therapist agreement in HHIW–HE ratings. Each rating was first categorized dichotomously; that is, items scored as 4 (always) or 3 (some of the time), reflecting negative perceptions, were categorized as negative statements, whereas items scored as 2 (some of the time) or 1 (all of the time), reflecting positive perceptions, were grouped as positive statements. If both the child’s and the therapist’s ratings were in the positive or negative statement category, agreement was surmised. Items that children rated positively and that the therapist rated negatively were categorized as overrated by the child, and in the opposite condition, as underrated by the child. Spearman’s correlations were computed to examine the correlation between the children’s and the therapists’ ratings on the HHIW–HE items and between the therapist’s scores on the BATH and the child’s HHIW–HE total scores. The percentage of child–therapist agreement on the tool’s items between the groups was compared using t tests.
Results
The children in the research group scored in the dysgraphic range on the BATH (16–32; M = 22.69, SD = 3.91), whereas children in the control group received scores indicating no dysgraphia (1–14; M = 7.41, SD = 3.17). Internal consistency, determined using Cronbach’s α for all 24 items, was good (α = .884), and removal of any of the items was not found to substantially change the size of the coefficient (range = .875–.884). For known-group comparisons, the calculation of between-group HHIW–HE scores revealed that children with dysgraphia rated themselves as significantly more impaired than children without dysgraphia on the total HHIW–HW scores and on 6 of the 24 items. Analysis of group differences in self-ratings revealed moderate to large effect sizes (Table 1).
Comparison of Median Self-Rating Scores of Children With and Without Dysgraphia for HHIW–HE Items
Note. HHIW–HE = Here’s How I Write–Hebrew.
0.1 = small effect, 0.3 = medium effect, 0.5 = large effect.
Significant at .002 after Bonferroni correction for multiple comparisons.
For between-group child–therapist agreement and disagreement (i.e., self-awareness), the mean percentage of items that children and therapists agreed on was significantly higher for the control group (M = 84.88, SD = 10.72) than for the research group (M = 71.25, SD = 13.43), as confirmed by an independent sample t test, t(56) = 4.268, p = .000. However, when comparing the percentage of disagreement between child and therapist, Table 2 shows a clear pattern whereby overrating was far more frequent among children with dysgraphia than among the controls. In addition, a significant moderate correlation was found between the total HHIW–HE and total BATH scores of the control group (r = .457, p = .013), whereas no significant correlation was found in the research group (r = .171, p = .374).
Comparison Between Ratings of Therapists and of Participants With and Without Dysgraphia on HHIW–HE Items
Note. HHIW–HE = Here’s How I Write–Hebrew. Therapists did not rate 3 items. Agreement = child and therapist both rated positively, or both rated negatively; overrated = child rated positively, and therapist rated negatively; underrated = child rated negatively, and therapist rated positively.
Discussion
The current study was performed to examine the psychometric properties of a new client-centered handwriting self-assessment tool for schoolchildren in Grades 2–5. The tool was also used to examine the degree of handwriting skill self-awareness among children with and without dysgraphia.
Psychometric Properties
Data analysis of the tool revealed a Cronbach’s α of .884, indicating that the tool’s items are related to each other and support its internal consistency. Significant differences were found between the groups on the total HHIW–HE scores, with moderate to large effect sizes, reflecting the tool’s ability to distinguish between known groups. These findings provide support for the validity of the HHIW–HE as a tool that measures schoolchildren’s perceptions of their handwriting abilities.
Interestingly, similar low median scores (not identified as a problem) were found in both groups on several items. For example, Item 7 addresses mixing print and cursive letters, and Item 12 addresses correctly writing letters that extend above the lines. The low scores on these items may reflect that indeed there is no problem (child–therapist agreement on Item 7 was 94%) or that children with dysgraphia may be overestimating their handwriting abilities (48%–69% disagreement on Item 12; see Table 2).
Self-Awareness
In this study, children’s overall self-awareness regarding their handwriting abilities was supported by the moderate to high percentages of child–therapist agreement in HHIW–HE ratings among all the study participants. This finding is supported by that of Engel-Yeger and colleagues (2009), attesting to the growing evidence that children’s self-report is reliable when planning client-centered occupational therapy intervention (Keller & Kielhofner, 2005; Missiuna et al., 2006).
Notwithstanding, as reported by Engel-Yeger et al. (2009), the level of self-awareness was lower in the dysgraphic group than in the control group. Moreover, in contrast to the control group, no significant correlation was found between their total HHIW–HE scores and those of occupational therapists on the BATH questionnaire. These findings suggest that although children with dysgraphia are aware of some of their handwriting abilities, they tend to overrate their abilities when compared with therapists’ evaluations. Previous studies have shown that overestimation correlates significantly with a lack of awareness (Krueger et al., 2011; Stone & May 2002), suggesting that children with dysgraphia may be less aware of the extent and severity of their handwriting difficulties.
The finding of frequent overrating among children with dysgraphia is similar to the reported positive illusory bias reported among children with developmental difficulties such as learning disabilities and attention deficit hyperactivity disorder (Heath & Glen, 2005; Hoza et al., 2012). The literature focusing on the relationship between self-awareness and dysgraphia is scarce. However, several possible explanations can be posited regarding these results. One explanation may relate to study findings linking dysgraphia to impairments in executive functions (Altemeier et al., 2006; Volman et al., 2006). Pursuant to this explanation, the HHIW–HE may be beneficial in enhancing the awareness of children with dysgraphia regarding their handwriting abilities to improve handwriting intervention outcomes.
Another possible explanation regarding the difference in child–therapist agreement between the study groups relates to psychogenic factors. Hoza and colleagues (2012) found that overestimation in children can result in part from their attempts to cope with their problems through self-protective mechanisms. Thus, children with dysgraphia may find it emotionally threatening to report on their deficits, whereas children without dysgraphia have less difficulty (Cermak & Bissell, 2014; Stone & May, 2002). This explanation also points to the potential advantage of the HHIW–HE: Its child-friendly presentation and collaborative format strengthen the child’s perceived self-efficacy as an active partner in the therapeutic relationship.
Limitations and Future Research
As a result of the small sample size and use of convenience sampling of children from central Israel, caution should be used in generalizing the study findings. In addition, the majority of participants were in Grades 2–3 (n = 51; 87.9%). We also did not control for dyslexia and other developmental disabilities, which may influence writing. Therefore, studies should control for these factors in larger more representative samples. Finally, the performance-based HHE raw scores were not recorded because only cutoff scores were used to confirm the group criteria. This study examined the self-assessment aspect of the tool but not the goal-setting aspect, which should be explored in future research.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
Studies have shown that enhancing children’s awareness and engagement in intervention is related to better therapy outcomes (Josman & Rosenblum, 2011), which may affect their effort, persistence, and commitment toward attaining their intervention goals (Zheng et al., 2014), and occupational therapists using the HHIW–HE have reported that children eagerly respond to the tool’s pictorial format and to participating in determining therapy goals.
This study suggests that the HHIW–HE is a valid, child-friendly tool developed to enable all team members (therapists, teachers, and parents) to understand children’s perspectives regarding their needs and preferences in improving their handwriting deficits.
The HHIW–HE may promote children’s reflection on their handwriting and their awareness of their handwriting performance.
Occupational therapists have reported that the HHIW–HE process encourages children’s active participation in handwriting intervention, potentially enhancing their feelings of self-efficacy and therapy outcomes.
Conclusion
The current study supports the HHIW–HE’s validity and internal consistency. In addition, although children with dysgraphia could detect many of their handwriting strengths and weaknesses, they also demonstrated more frequent overestimation of their abilities than children with proficient handwriting. This finding may relate to neurogenic or psychogenic factors or to a combination of both. Further studies are recommended to investigate this phenomenon to improve therapeutic intervention approaches.