
Abstract
After hemiplegia, rehabilitation of the upper extremity (UE)—the hand, in particular—can be extremely challenging for occupational therapy practitioners. Because many people with chronic stroke (≥6 mo after onset) exhibit persistent and complex UE deficits (Tsu, Abrams, & Byl, 2014), practical interventions that result in improved performance of daily tasks for this population are needed. In addition, current neuroscience research reinforces that functional gains can still be made using targeted interventions several months and even years after stroke onset (Sun, Boots, & Zehr, 2015).
Neuromuscular electrical stimulation (hereinafter, ES) has been extensively studied to determine its effectiveness in increasing movement in the hand in people with chronic stroke (for a review, see Quandt & Hummel, 2014). Various forms of ES have been examined for reducing limitations due to UE hemiplegia, including constant repetitive on–off cycles of ES (cyclic ES; de Kroon & IJzerman, 2008), ES triggered when voluntary muscle activity is initiated volitionally by the patient and observed through electromyography (EMG; referred to here inafter as EMG-triggered ES; Singer, Vallence, Cleary, Cooper, & Loftus, 2013), or ES provided at low frequencies targeting sensory fibers only instead of motor fibers (sensory-level ES; Sullivan et al., 2015). Evidence suggests, however, that ES has its greatest effect when used as an adjunct to or in combination with other interventions. ES regimens have shown efficacy for improved movement in the hand when combined with mechanical strategies, including robotic training (Lee et al., 2015), when embedded within neuroprosthetics (Page, Levin, Hermann, Dunning, & Levine, 2012; Persch, Page, & Murray, 2012), or combined with other types of orthoses (for a review, see Aoyagi & Tsubahara, 2004).
A commercially available hand–wrist orthosis that is often used in the practice of occupational therapy is a dynamic, nonelectric, mechanical device, the SaeboFlex™, offered by Saebo Inc. (Charlotte, NC; Hoffman & Blakey, 2011). This dynamic hand orthosis (DHO) is used to perform repetitive task training (RTT) incorporating continuous grasp–release motions and can be used at home after instruction by a trained occupational therapist or under supervision at a clinic.
A few limited studies of effectiveness have examined use of the device in people with chronic stroke. Five people with chronic stroke showed improved UE movement and increased Fugl–Meyer (Fugl-Meyer, Jääskö, Leyman, Olsson, & Steglind, 1975) and Box & Block (Mathiowetz, Volland, Kashman, & Weber, 1985) scores after a 4-wk 5×/day DHO–RTT program (Woo, Jeon, Hwang, Choi, & Lee, 2013). Farrell, Hoffman, Snyder, Giuliani, and Bohannon (2007) showed gains in active range of motion (AROM) of the shoulder and arm and improved Fugl–Meyer scores using a shortened DHO–RTT regimen (6 hr/day for 1 wk) with 13 people with chronic stroke. Butler, Blanton, Rowe, and Wolf (2006) examined outcomes of the DHO regimen in a single-participant case report in which minimal gains in wrist AROM and use were noted. In contrast, Barry, Ross, and Woehrle (2012) found no significant difference between the SaeboFlex orthosis training group and a manual therapy group that had incorporated a similar number of repetitions.
Studies of intervention effectiveness for people with chronic stroke are needed that translate improvements in impairments to a person's ability to perform specific daily living tasks. These skills can be measured when using standardized validated tests such as the Assessment of Motor and Process Skills (AMPS; Fisher & Bray Jones, 2010) or other task-based measures to quantify function objectively. The purpose of this pilot study was to explore the performance of specific daily living tasks using the AMPS after a 6-wk combined regimen using ES and the SaeboFlex orthosis with RTT in 4 people with chronic stroke. We also included biomechanical EMG measures of grasp, a movement central to object manipulation that is strongly associated with activities of daily living (ADL) performance in people with chronic stroke (Bae et al., 2015). Feasibility and logistics for translation of these preliminary results to a larger, more comprehensive controlled trial were also explored.
Method
Study Design
In this small pilot study we examined biomechanical and functional outcomes using a single-group, pretest–posttest design over the course of a 6-wk combined treatment regimen incorporating the DHO–RTT program followed by application of ES in 4 people with chronic stroke.
Participants
Participants were recruited during a university-based free stroke clinic and were required to (1) have a diagnosis of ischemic or hemorrhagic stroke that had occurred at least 6 mo before the date of participation, (2) be between ages 20 and 85 yr, (3) exhibit a minimal amount of UE movement (approximately 10° active wrist or digit movement), (4) be able to communicate orally and provide informed consent, and (5) be able to comprehend the responsibilities and procedures related to the study. People who had contraindicating conditions for the application of ES (implanted electronics, pacemakers, etc.) were not enrolled. Four participants initially responded to the recruitment flyers, met inclusion criteria, and volunteered to participate. See Table 1 for participant demographics.
Participant Demographics
Note. L = left; M = male; R = right.
Outcome Measures
Grip strength and AROM of the wrist and third metacarpophalangeal (MCP) joint (flexion/extension) were assessed before and after completion of the training intervention. These AROM measures were selected as target outcomes because both play a role in the grasp–release motion, which is essential for functional task performance. EMG data were collected to quantify functional muscle deactivation of forearm extrinsic hand muscles during grasp release in the hemiplegic hand.
The AMPS battery was used as an outcome measure to quantify participants’ ability to perform functional daily tasks. The AMPS is a comprehensive, validated, reliable test that evaluates the performance quality of instrumental activities of daily living (Fisher & Bray Jones, 2010). The AMPS yields numerical scores of ADL ability (in units of logits) ranging from −3 to 4 for the motor domain and −4 to 3 for the process domain. Lower scores indicate the need for more physical assistance and a less efficient performance in the two areas, respectively. The minimal clinically important difference (MCID) on the AMPS determined by Fisher and Bray-Jones (2010) is 0.3 logits. Two tasks—folding a basket of clothes and making a peanut butter and jelly sandwich—were selected for all participants in this pilot study; this was done to establish a level of homogeneity and consistency of procedures between participants. These tasks were chosen because both could be performed in sitting or standing, required frequent postural adjustments, and incorporated gross motor movements in the arm and fine dexterous movements of the hand.
Equipment
A standard midsized goniometer was used for wrist AROM, and a small digit goniometer (both from Patterson Medical Inc., Warrenville, IL) was used for third MCP joint AROM. Grip strength was evaluated by means of a hydraulic analog hand dynamometer (Jamar Inc., Hatfield, PA). The dynamic orthosis used in this study was the SaeboFlex device, a custom-fitted nonelectric orthosis that allows active flexion of the MCP and interphalangeal joints, with the attached springs creating a passive functional release after grasping. ES was delivered using the Empi 300PV (Empi Inc., St. Paul, MN), a portable stimulation unit. Surface EMG data were collected using a bipolar parallel-bar (1 mm × 1 cm, spaced 1 cm apart) recording electrode and the Myomonitor IV EMG system (Delsys Inc., Boston).
Intervention Program
Participants donned the orthosis on the affected UE with therapist assistance and performed the RTT grasp–release practice daily for 30 min, 5×/wk for 6 wk (30 sessions). Participants grasped 4-in. foam balls placed at midline by the therapist and transferred them to a low-sided box on the table at an arm’s distance away, either to the right or to the left. Twenty-four balls were grasped, transported, and released into the box on one side before alternating to the other side. This sequence was followed for 30 min, and participants were instructed to complete as many boxes as possible during this period. They could rest for 2 min when needed, but the amount of time spent in actual RTT for all participants remained consistent at 30 min.
ES to the finger extensor muscles was provided for 15 min after the RTT. ES was delivered after the RTT for all participants because of the neuromuscular fatigue that typically results in hemiplegic muscle after delivery of constant-frequency stimulation patterns (Doucet & Griffin, 2009). Two bipolar surface electrodes were applied: One was placed over the extensor muscle group, centered over the extensor carpi ulnaris; the second, inactive electrode was placed just proximal to the ulnar styloid at the wrist. Biphasic sine wave pulses were delivered at 35 Hz, using a duty cycle of 1:1.5 (10 s on, 15 s off) and a pulse width of 350 μs. These parameters were selected as optimal on the basis of a comprehensive review of ES patterns and parameters for musculoskeletal function (Doucet, Lam, & Griffin, 2012). Intensity amperage was individualized at each session to elicit a full tetanic contraction of wrist extension within the participant’s tolerance. Participants were encouraged to actively extend their fingers and wrist during the “on” phase of ES.
Data Collection
Goniometry, dynamometry, and AMPS administration were performed before starting the intervention (baseline) and 1 day after the final training session by therapists blinded to the specific study procedures. Two EMG recording electrodes were placed over the bellies of the primary extensor muscles in the dorsal forearm and over the primary flexor muscles in the ventral forearm. Electrode sites were marked with permanent marker, and participants were instructed to redraw the marks before and after bathing or showering for the duration of the study. EMG recordings were taken during performance of a 5-s maximal voluntary isometric contraction grasp around the dynamometer handle using the hemiplegic hand; an auditory cue was provided at 5 s to initiate grasp and at 10 s to release. Study feasibility information regarding overall logistics, participant compliance with study procedures, tolerance of study activities, and adherence to protocol were also collected.
Data Analysis
AROM and grip strength, in degrees and pounds of pressure, respectively, were collected. To quantify grasp release, the root mean square of the EMG signal was analyzed during the time period immediately after the auditory cue to release grasp (at the 10-s time point). The EMG signal was high-pass filtered at 20 Hz, collected at a sample frequency of 2000 Hz, and then analyzed using EMGWorks software (Delsys Inc., Boston). EMG signals were full-wave rectified and normalized to the baseline recording signal obtained before muscle contraction. Time needed for a signal to return to baseline was also measured after the 5-s grasp until the EMG signal returned to baseline. Analysis of EMG data was performed by a trained specialist blinded to the specific procedures of the study.
Results
Strength, AROM, and AMPS motor and process scores collected before and after the implementation of the combined ES–DHO program in our 4 participants, as well as changes in muscle activation, are reported in Table 2. Modest gains in most outcome measures were demonstrated by all participants. See Figure 1 for representative EMG raw data.
Scores for Outcome Measures Before (Pre) and After (Post) Combined Electrical Stimulation–Orthosis Intervention for Each of the 4 Participants
Note. Strength and ROM measures are from the affected upper extremity; ROM reflects total range of available movement from flexed or resting position to maximal extension position. Change scores are indicated by Δ. AMPS = Assessment of Motor and Process Skills; BL = initial/pretest EMG RMS baseline value; deg. = degrees; EMG = electromyography; MCP = metacarpophalangeal; RMS = root mean square; ROM = range of motion.
For EMG data, post score reflects the percentage change of the baseline pretest RMS value. Negative change scores indicate a reduction in the EMG signal, indicating reduction or deactivation of muscular activity.
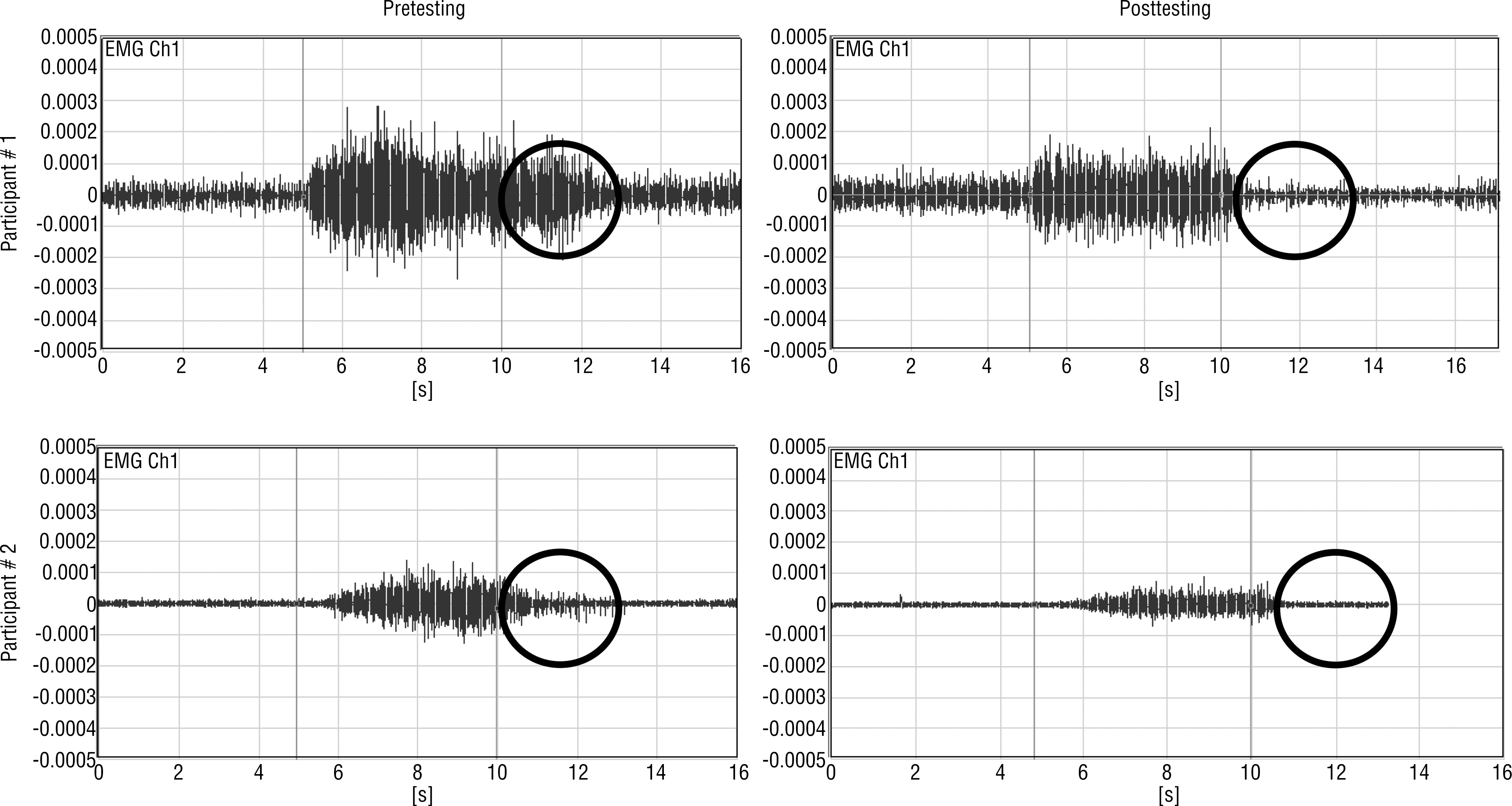
Raw EMG signal reflecting flexor muscle electrical activity of a grasp initiated at the 5-s time point and released at the 10-s time point (between vertical lines) using auditory cues.
By conducting this pilot work, we established that implementation of this treatment regimen with a small group of people with chronic stroke is logistically feasible. All participants tolerated the combined intervention without any adverse events. On average, each participant required rescheduling of a training session on 3.75 occasions across the duration of the project. We believe that overall compliance with study procedures was excellent because these individuals were not currently receiving any therapy services; therefore, all were motivated to engage in the training.
Discussion
These preliminary results suggest that gains may be made in hand strength, AROM, and grasp release with a combined ES–DHO program in people with chronic stroke. The results also indicate that this type of training may translate to improvement in specific task performance for some people. The improved performance on the tasks selected may be related to the improved strength and ability to release grasp after the treatment intervention.
A previous study used the DHO regimen with 26 people with chronic stroke who showed improvement in motor function and cortical activation when the regimen was combined with bilateral training (McCombe Waller et al., 2014). A recent feasibility study focused on 9 inpatients with stroke approximately 6 wk poststroke using the DHO, but no differences were seen in UE function between the experimental and control groups (Lannin et al., 2016). Few large-scale, rigorous controlled studies that support the effectiveness of this DHO–RTT program for improving functional task performance in people with chronic stroke have been published in peer-reviewed journals.
Three of our participants had sustained ischemic strokes, and Participant 4 had a hemorrhagic stroke, which could account for the variability in outcomes. Participant 4 demonstrated severe hypertonicity in the affected UE compared with the other participants; this resulted in frequent readjusting of the orthosis; therefore, we hypothesized that his improvement was limited because of the tonal abnormalities in place. We will explore this finding further in the larger follow-up trial to analyze whether excessive spasticity inhibits optimal use of this device. Participant 2 had bronchitis and a severe cold on the day of posttesting, which could have affected his outcomes. We suspect that these issues resulted in Participants 2 and 4 not meeting the AMPS MCID in the motor or process domain.
This preliminary pilot work is limited, and the results should be interpreted with caution because only 4 volunteers with chronic stroke were studied. Type of stroke, time since stroke, age, and clinical presentation differed among the participants; this could also have affected the results. The two tasks chosen on the AMPS measure were preselected instead of allowing participants to select their choice of task. This could have influenced the results because of the lack of choice and meaning for the individual; this will be revised in our future studies.
Because the SaeboFlex device is widely used in clinical practice (more than 100,000 people treated worldwide; see http://www.saebo.com) and limited evidence exists of its effectiveness in improving performance of daily tasks, further studies should be conducted. Designing a larger controlled trial will allow in-depth statistical analysis and further exploration of other pertinent factors, such as patient response, dosing, and so on, so professionals can better interpret these preliminary findings.
Implications for Occupational Therapy Practice
This study offers the following implications for occupational therapy practice:
Hand strength, ROM, and release of grasp may be enhanced in people with chronic stroke who participate in a combined ES–DHO program incorporating RTT.
Such training could contribute to improvements in the ability to perform specific daily living tasks.
Studies that explore evidence-based interventions that can translate improvements in biomechanical impairments to directly yield changes in the ability to perform specific daily living tasks are urgently needed.
Conclusion
The results from this pilot work suggest that a 6-wk program of a combined ES–DHO regimen incorporating RTT is feasible and may be effective in improving UE deficits experienced by some people with chronic stroke. A larger, more comprehensive comparative study is needed to further investigate and expand on these preliminary findings.