
Abstract
Loss of upper extremity function after a stroke has been attributed to significant limitations in a person’s ability to perform daily tasks (Lai, Studenski, Duncan, & Perera, 2002). Innovations have emerged in the past 2 decades in the field of stroke rehabilitation based on contemporary understanding of brain recovery. Interventions that have undergone rigorous clinical trials include constraint-induced movement therapy, robot-assisted therapy, transcranial magnetic stimulation, and functional/neuromuscular electrical stimulation (Carter, Connor, & Dromerick, 2010). However, these interventions come with practical limitations for the frontline occupational therapy practitioner, including cost of and access to delivery and stringent inclusion criteria (Viana & Teasell, 2012). Few options exist, especially for people who demonstrate a significant impairment (Invernizzi et al., 2013). Mirror therapy presents an option for a variety of stroke survivors along the recovery spectrum. A Cochrane Review representing 14 studies showed evidence for the effectiveness of mirror therapy as an adjunct for improving upper extremity motor function in people who have suffered a stroke (Thieme, Mehrholz, Polh, Behrens, & Dohle, 2013).
Mirror therapy is an approach that makes use of a mirror to reflect movements of the less involved upper limb as if it were the more affected limb. This approach draws from the understanding that the mirror neuron system from the parietal-frontal and premotor brain regions becomes activated by simply observing an action (Carvalho et al., 2013; Thieme et al., 2013). Research on mirror therapy continues to emerge. In their systematic review, Thieme and colleagues (2013) found that studies were inconsistent in the application of therapy protocols, including treatment dose and the use of controls. They recommended that mirror therapy be applied as an adjunct to rehabilitation therapies for motor impairments.
Task-Oriented Training
The use of active practice of task-oriented activities is commonplace in stroke rehabilitation. Advances in neurorehabilitation research have demonstrated that movement repetition is key to promoting functional improvements (Teasell, Bitensky, Salter, & Bayona, 2005). However, repetition alone may not suffice. In their Cochrane Review of 14 trials (n = 659), French and colleagues (2010) noted that intensive repetition did not produce meaningful improvements in upper limb function. They suggested that task specificity and not repetition should be considered for practice. Studies have shown positive neuroplastic and lasting functional improvements in the hemiplegic upper limb as a result of task-specific training (Fleming et al., 2015; Kumar & Goyal, 2012; Paik, Kim, Lee, & Jeon, 2014; Song, 2014).
One clinical challenge to providing task-specific training is ensuring that the task itself has intrinsic value to the patient and that it presents a just-right demand to the patient’s upper limb functioning. When the task demands exceed the patient’s abilities, augmentative strategies may be warranted. For patients whose functional repertoire is limited because of slow or poor motor recovery in the hand (e.g., limited finger extension or thumb opposition), a variety of rehabilitative modalities, combined with task-specific training, have shown promising effects. These modalities include electrical stimulation (Persch, Page, & Murray, 2012; Sullivan & Hedman, 2007), functional orthoses (Taub et al., 2013), and mirror therapy (Arya & Pandian, 2013; Kumar & Goyal, 2012). Particularly for mirror therapy, it is not only readily accessible to the everyday clinician but also low cost, easy to use, portable, and feasible for in-home implementation. In addition, as intervention protocols for mirror therapy continue to emerge, one important concept that supports its clinical use is priming.
Mirror Therapy as Priming
Priming is defined as an implicit type of learning based on a prior exposure to stimuli (Stoykov & Madhavan, 2015). When the cortical region of the brain is primed by certain stimuli, it is more responsive to the training that precedes or accompanies the stimuli. Motor imagery, such as mental practice and mirror therapy, has been identified as a priming modality that can influence corticospinal excitability (Fadiga et al., 1999), which translates into improved motor control (Barclay-Goddard, Stevenson, Poluha, & Thalman, 2011; Butler & Page, 2006; Peters & Page, 2015). However, the type of movement to be practiced through motor imagery has to be task specific and meaningful for it to be successful. Thus, the purpose of this study was to determine the effect of a combined intervention of mirror therapy priming and task-oriented training on upper extremity functioning and occupational performance in people with hemiparesis.
Method
Design
The study followed a quasi-experimental case series design with repeated measures (Zhan & Ottenbacher, 2001). Outcome data were collected at baseline and at 2 wk (midtest), 4 wk (Posttest 1), and 6 wk (Posttest 2) after the intervention.
Participants
Participants were conveniently recruited from local outpatient clinics through flyers and referrals. The five inclusion criteria were (1) at least 3 mo poststroke, (2) home-dwelling status, (3) >24 on the Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975), (4) availability of arm and hand function at Brunnstrom Approach (Sawner, LaVigne, & Brunnstrom, 1992) Recovery Stage III or above, and (5) at least 21 yr of age. The 3-mo onset was chosen for two reasons: First, the typical clinical course of inpatient through outpatient stroke rehabilitation tends to take place over a 12-wk period, and second, the literature suggests that functional recovery in the first 3 mo of onset is largely influenced by the natural recovery (Teasell & Hussein, 2016). The exclusion criteria were major visual deficits, history of other neurological diseases, and actively healing musculoskeletal conditions.
Intervention
Each participant completed a 4-wk intervention consisting of both mirror therapy and task-oriented training 2×/wk for 45- to 60-min sessions in the clinic and 4×/wk at home. Intervention frequency and duration reflect the typical therapy dosing received by clients in real-world practice. In-clinic sessions were used to train participants on interventions to be completed at home. Compliance logs and return demonstrations at the start of the subsequent sessions were reviewed by the interventionists for fidelity.
Mirror Therapy Intervention.
Participants began mirror therapy sessions with 20–25 repetitions of reaching forward, elbow flexion, forearm supination and pronation, wrist flexion and extension, gross grasp and release, and opposition, amounting to a minimum of 150 repetitions. Participants were instructed to initially focus on the mirror reflection of the nonparetic limb and imagine that the movement was being produced by the paretic extremity. Subsequently, participants were encouraged to try moving the paretic limb in the same fashion. Each participant was provided with a foldable mirror box for home use.
Task-Oriented Training.
Using the Patient-Specific Functional Scale (PSFS; Horn et al., 2012), participants identified three priority activities that were difficult to complete with their paretic upper limb. Task analyses, incorporating the participant’s level of arm and hand function and the task demands, were performed to identify the optimal combination of movements. Practice activities were planned to ensure high repetition (>150 trials) and included shaping, variations in bilateral arm–hand use, and adaptations to task and environment to ensure the just-right challenge. Problem solving was facilitated so that participants generated strategies to use their paretic limb in a variety of functional ways both in the clinic and at home.
Outcome Measures
The study used the following outcome measures: Upper Extremity subscale of the Fugl-Meyer Assessment (FMA–UE; Fugl-Meyer, Jääskö, Leyman, Olsson, & Steglind, 1975), the Motor Activity Log (MAL; Uswatte et al., 2006), and the PSFS. The FMA–UE was used as the primary outcome measure to assess volitional movement of the paretic extremity using a 3-point ordinal scale (Gladstone, Danells, & Black, 2002). Scores for the arm and for the hand/wrist were analyzed separately and provided bases for how task-specific training was graded. Wagner, Rhodes, and Patten (2008) reported a minimum detectable change (MDC) of 5.2 points to be clinically meaningful.
The PSFS is a questionnaire used to record activity limitations and participation restrictions that patients find important. The measure shares a similar approach as the Canadian Occupational Performance Measure (Law et al., 2005) in assessing a person’s perceived performance in activities that he or she finds meaningful. Thus, the authors consider the PSFS as a scale to measure occupational performance. Patients rate their perceived level of difficulty from 0 (being unable to perform the activity) to 10 (being able to perform the activity at the same level as before the stroke). Stratford, Gill, Westaway, and Binkley (1995) indicated an MDC of 3 points on a single item and 2 points on the average score of all items.
The MAL is a self-report measure that is used to assess real-world function of the hemiparetic limb. It measures both how often (Amount of Use [AoU] index) and how well (Quality of Movement [QoM] index) the patient uses the affected limb (Page, Levine, Leonard, Szaflarski, & Kissela, 2008) on a scale from 0 (not used at all) to 5 (used as before or normal like my other arm) at half- or 1-point increments. The MDC for the AoU index is a score increase by 24% and for the QoM index is a score increase by 15% (Chen, Wolf, Zhang, Thompson, & Winstein, 2012).
Data Analysis
Through graphical and tabular representation of data, we examined trends in data and interpreted a change at or above the established MDC of the previously mentioned measures as clinically meaningful (i.e., an observable functional change has occurred in the domain of concern).
Results
Four adults, ages 22–67 yr, with varying onset of stroke participated in the study (Table 1). Five participants met all inclusion criteria after baseline testing and began the intervention protocol. One participant withdrew because of family issues after 1 wk of intervention.
Participant Demographics
Note. — = not applicable.
Fugl–Meyer Assessment—Upper Extremity
Figure 1 shows the trend in participants’ scores on the FMA–UE. Three participants achieved the MDC at Posttest 1, and 1 achieved it at Posttest 2. Participants 3 and 4, who began with lower FMA–UE scores (38 and 41, respectively), benefited the most with a 13-point increase by Posttest 2. Participants 1 and 2 had a higher baseline but achieved the MDC by Posttest 2. Participants 3 and 4 had a greater increase in the hand–wrist items, at 10 points, by Posttest 2 compared with Participants 1 and 2, who had an increase of 3 and 4 points, respectively, for the same period. All participants had an increase in the arm items of 2 to 5 points, which appears to correspond with the practice activities that participants chose for their task-oriented training. Participants who identified tasks with more fine motor demands (e.g., crocheting, playing with checkers) had more gains in their hand function than their arm function.
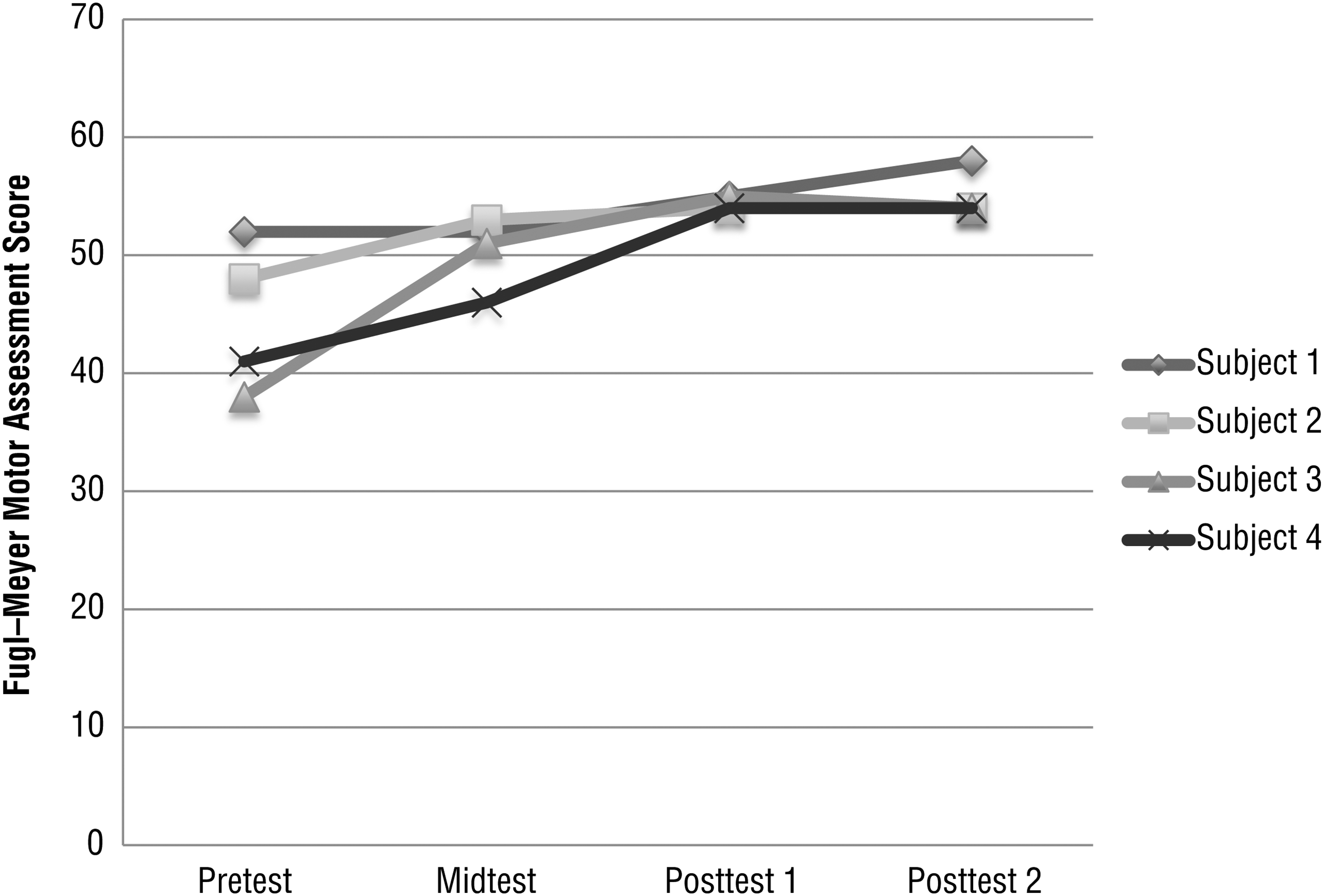
Line graph depicting trend of participants’ scores over time for the combined components of arm and hand on the Fugl–Meyer Assessment—Upper Extremity.
Motor Activity Log
Participants varied in their AoU scores over time but displayed a pattern of steady improvement in QoM scores until achieving the MDC (Table 2). Another important observation is the gradual increase in the number of items attempted by the participants over time. Such an increase may signify an expansion in movement repertoire as function and control increase. The inconsistency in AoU scores may be attributed to participants’ focused effort to practice tasks that were more meaningful as part of their home program. These activities have similarities with, but are exclusive of items listed in, the MAL. Thus, during AoU assessment, participants may report less frequency of attempts to “flip a light switch” (MAL Item 1) or “remove an item of clothing . . .” (MAL Item 3) but continue to observe improvements in movement quality.
Change in MAL AoU and QoM Index, Activity Items Attempted, and MDC Achievement
Note. AoU = Amount of Use; MAL = Motor Activity Log; MDC = minimum detectable change; NA = not applicable; QoM = Quality of Movement.
MDC for AoU index is a score increase by 24% and for QoM index is a score increase by 15%.
Patient-Specific Functional Scale
Table 3 details the activities identified by the participants as priorities for intervention and the corresponding self-rating across measurement points. Participants 1, 3, and 4 exceeded the MDC on the average of all items. Participant 2 also had an average change of +2 points (which met the MDC), but each individual item did not achieve the MDC of +3 (Stratford et al., 1995). Note that Participant 2 reported having a cold, which lessened her ability to carry out her home practice schedule.
Items Selected, Individual Item Scores and Averages in the PSFS, and MDC Achievement
Note. MDC = minimum detectable change; PSFS = Patient-Specific Functional Scale.
MDC for single item = +3 points; MDC for average of all items = +2 points.
Discussion
This study examined the effect of a combined mirror therapy and task-oriented training for people with hemiparesis. Because of heterogeneity of the participants, our use of a single-subject methodology (Zhan & Ottenbacher, 2001) afforded meaningful analyses of the intervention effects. All participants demonstrated clinically meaningful improvements in their arm and hand function as measured by the FMA–UE and in their performance of tasks within their chosen occupations as measured by the PSFS. Most motor improvements were seen in the wrist and hand in large part because of the types of task-specific practice chosen. One limitation of this study, however, is not measuring the long-term outcomes. Therefore, a research implication is to determine whether short-term gains have long-term functional carryover. One unintended but positive outcome is that participants reported an increase in their repertoire of activities as a result of improvements in the quality of their movement. As clients rediscover greater functional utility in their paretic limb, they more likely are motivated to continue to incorporate its use.
Our findings are consistent with the literature showing that mirror therapy is effective in facilitating motor recovery in the paretic limbs of people with stroke regardless of whether onset is acute or subacute (Arya et al., 2012; Invernizzi et al., 2013; Lee, Cho, & Song, 2012; Samuelkamaleshkumar et al., 2014; Yavuzer et al., 2008) or chronic (Arya & Pandian, 2013; Michielsen et al., 2011). When used as an adjunct to traditional therapies, mirror therapy is just as effective for stroke survivors who have mild impairments in their arm and hand function as it is for those with severe impairments. With various protocols to incorporate mirror therapy in stroke rehabilitation (Dohle et al., 2009; Thieme et al., 2013), this study adds to the body of literature by demonstrating how mirror therapy was used as priming (Stoykov & Madhavan, 2015) to task-oriented training.
A particular feature of this study is the use of client-centered, patient-specific task practice that did not require extensive amounts of practice. We considered the participants’ lifestyles and occupational routines in designing the home-based component of the intervention protocol. The specificity of the task to the client has been identified as a more important feature to training than repetition alone (Kumar & Goyal, 2012; Page, 2003; Paik et al., 2014; Teasell et al., 2005). In addition, the literature supports embedding occupation as an effective strategy for promoting functional motor recovery in people with stroke (Lin, Wu, Tickle-Degnen, & Coster, 1997; Trombly & Ma, 2002). When clients engage in tasks that they find meaningful, the task performance itself is intrinsically motivating. Moreover, when the tasks exert the just-right challenge and fit within clients’ occupational patterns, clients are likely to persevere and experience a sense of self-efficacy with use of their paretic limb.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
Despite a growing body of evidence that demonstrates the efficacy of mirror therapy and task-specific, task-oriented training, the translation of evidence into practice remains a major concern. However, this study contributes to evidence translation by demonstrating the effectiveness of an intervention protocol that closely approximates typical therapy dosing in real-world practice. The limited number of in-clinic visits by participants was largely augmented by a highly structured, well-planned home program that put participants in charge of their own training.
Given issues regarding follow-through on home programs for people with stroke (Chen, Neufeld, Feely, & Skinner, 1999; Taub et al., 2013), this study carefully considered the participants’ occupational routines and interests as a way to facilitate compliance. Our findings support the notion that when prescribed activities are deemed meaningful and relevant to their life, people will likely persist through engagement.
This intervention is practical for both the client and the occupational therapy practitioner. The tools used for mirror therapy are inexpensive, easy to use, and portable, and they do not require specialized training or technical maintenance. However, for this intervention to be effective, practitioners must consider the evidence and its theoretical underpinnings.
Conclusion
Mirror therapy, when combined with and used as priming for client-specific, task-oriented training, can produce improvements in motor function and facilitate increased occupational performance for people with hemiparesis. Clients with varying severity and onset of stroke may equally benefit from a combined mirror therapy and task-oriented training.
Footnotes
Acknowledgments
This study is registered through ![]() (NCT02917343). The study was funded by a Quinnipiac University School of Health Sciences Interprofessional Faculty Research Grant. Portions of this study were presented at the American Congress of Rehabilitation Medicine 92nd Annual Conference, October 2015, Dallas, TX.
(NCT02917343). The study was funded by a Quinnipiac University School of Health Sciences Interprofessional Faculty Research Grant. Portions of this study were presented at the American Congress of Rehabilitation Medicine 92nd Annual Conference, October 2015, Dallas, TX.