
Abstract
Athletes with mild traumatic brain injury (mTBI) should refrain from high-risk activities until recovered (symptom free and cognitive and physical exam findings normalize). Studies have suggested that this examination may not be sufficiently sensitive because dual-task paradigms, which typically assess motor performance while a person simultaneously completes a distractor task, can detect residual deficits in athletes who otherwise appear recovered from mTBI. Paradigms used to date are time-intensive procedures conducted in laboratory settings. Here, we report findings from a pilot study of the Dual Task Screen (DTS), which is a brief evaluation with two dual-task paradigms. In 32 healthy female adolescents, the DTS was administered in a mean of 5.63 min in the community, and every participant had poorer dual-condition performance on at least one of the motor tasks. The DTS is a clinically feasible measure and merits additional study regarding utility in adolescents with mTBIs.
In the United States, children age 18 yr and younger sustain an estimated 1.1–1.9 million sports- and recreation-related concussions, or mild traumatic brain injury (mTBI), each year (Bryan, Rowhani-Rahbar, Comstock, & Rivara, 2016). Given the prevalence of this issue, evaluation and management of mTBI have emerged as a major public health concern. Rehabilitation professionals, such as occupational therapy practitioners with their unique focus on participation in meaningful occupations, are well suited for participating in post-mTBI management because they recognize the essential role of athletic engagement and know that return to play before complete recovery could cause long-term consequences across other occupations (Reed, 2012).
A mainstay of mTBI management is that athletes refrain from high-risk activities (e.g., contact sports) until they have fully recovered. Presently, the gold standard for safe return to activity is to determine that an athlete is asymptomatic on the basis of parent and self-report, physical examination, and cognitive performance (Phillips & Woessner, 2015). However, this gold standard may be insufficient, especially when athletes underreport symptoms. For this reason, it is critical that performance-based evaluations are as sensitive to residual deficits as possible.
Dual-task paradigms—assessments of motor performance during simultaneous distractor task administration—have demonstrated sensitivity in detecting residual deficits in adolescent athletes with mTBI (Dorman et al., 2015; Howell, Osternig, & Chou, 2013, 2015, 2016; Howell, Osternig, Koester, & Chou, 2014). Dual-task paradigms examine the relationship of dual-condition motor performance to single-condition motor performance, and, in the studies cited earlier, people with mTBI had significantly poorer motor performance under dual conditions compared with uninjured peers. Note, however, that Howell et al. (2015) observed these performance deficiencies after athletes were deemed clinically recovered and reportedly symptom free and early return to activity exacerbated mTBI-induced deficits.
Despite the essential role that these studies have played in post-mTBI research, the dual-task paradigms are time intensive and rely on cumbersome laboratory-based assessments that use retro-reflective markers, whole-body motion analysis instruments, strain gauge force platforms, and complex analysis software, which are not feasible for everyday clinical assessment. Additionally, all dual-task paradigms used to date in adolescent mTBI populations focus primarily on gait, posture, and balance; however, they have not yet examined integrated visual and upper extremity capacities, which are equally important for most sports.
To address these limitations, we developed the Dual Task Screen (DTS), which includes two clinically feasible dual-task paradigms, including a gait (i.e., Lower Extremity [LE]) subtask and a throw-and-catch (i.e., Upper Extremity [UE]) subtask. We opted to conduct a pilot study with healthy adolescents before studying people with mTBI because the less-restrictive inclusion criteria enhanced efficiency for DTS testing and allowed us to begin identifying the range of normative performance for later comparisons with adolescents with mTBI. The primary objectives of this pilot study were (1) to establish the feasibility of administration of the DTS in a community setting in a time-efficient manner (5–10 min); (2) to determine in an uninjured youth athlete population whether the LE, UE, or parallel administration of both tasks was most sensitive to poorer dual-condition motor performance; and (3) to describe the range of dual-task effects (i.e., percentage of dual-condition to single-condition performance) for each subtask.
Method
Participants
Healthy female adolescents were recruited from a local school via collaboration with the school’s athletic trainer, who sent study recruitment information to parents. Parents provided written informed consent and information relevant to inclusion and exclusion criteria, and adolescents provided oral assent. Participants were excluded if they could not understand English or had a medical or physical condition that affected standing balance, walking ability, or ability to throw and catch a ball. Participants were also excluded if they had sustained a moderate or severe TBI, had sustained a recent mTBI (<6 mo before testing), or were experiencing any residual deficits from any previous brain injury. The Johns Hopkins Medicine institutional review board approved this study.
Procedure
A local school provided the research team with an empty classroom and four 50-min class periods for data collection. Participants were asked to list any medications taken on the day of testing (to assess potential confounding effects), which sports and positions they played, and how many years they had played these sports. Next, participants performed the DTS, which was videotaped by the research team so that scoring could be completed offsite.
Dual Task Screen
The DTS includes the LE and UE subtasks; each subtask was completed first as a single-motor condition without a cognitive distractor task and then as a dual condition including a cognitive distractor task. In the single-motor condition of the LE subtask, we used a previously published task of gait speed used in adults with mTBI (Cossette, Ouellet, & McFadyen, 2014). Participants were instructed to walk as quickly as possible for 6 m and step over a 1.5-m obstacle placed 4 m from the start; tape was placed on the floor indicating the start and finish lines. In the dual condition, participants engaged in the same LE subtask while repeating the months of the year backward. Gait speed (meters per second [m/s]) was calculated (see scoring of the DTS for detail) for the single and dual conditions, and the number of correctly recited months was recorded for the dual-task condition.
In the single-motor condition of the UE subtask, we used a publicly available coordination task, the Wall Toss Task (http://www.topendsports.com/testing/tests/wall-catch.htm), to measure hand–eye coordination. Participants were instructed to stand 1.5 m from a wall and to use alternating hands to throw (underhand) and catch a tennis ball for 30 s. In the dual condition, participants repeated the UE subtask while simultaneously serially subtracting 3s from 100. The number of successful catches was recorded for the single and dual conditions, and the number of correct subtractions was documented for the dual-task condition.
The DTS was designed to be administered without testing the cognitive tasks under a single-task condition; two factors contributed to this decision. First, there is precedence in dual-task studies with adolescents to test solely for poorer dual-condition motor performance (Dorman et al., 2015; Howell et al., 2013, 2014, 2016). Second, it was difficult to identify two distinct cognitive tasks (one for each motor task) that could adequately disrupt motor performance and be repeated without the confounding influence of practice effects. The cognitive tasks we selected had two important features: (1) they did not require any additional materials (e.g., headphones, visual materials), and (2) they took longer to complete than the motor tasks (i.e., participants would not finish the cognitive task before completing the motor activity, which ensured dual conditions throughout). The cognitive tasks were designed to require attention and distract motor performance; they were not designed to be matched on domain or level of difficulty.
Scoring of the Dual Task Screen
Two members of the research team viewed and scored all videotape recordings. For the LE subtask, timing started when the participant lifted her foot from behind the start line to begin walking and stopped when both feet crossed the finish line. The two researchers viewed the recording and repeated timing until timing by stopwatches agreed by <0.25 s, then averaged time was used to calculate gait speed (m/s). Videotape recordings were then viewed a final time to determine the number of months that the participant correctly recalled in the dual condition, with the scorers reaching consensus. Additionally, to determine how long it would take one person to score the DTS (i.e., in a clinical setting), one researcher rescored a subset of participants (10%) from the videotape recordings.
For the UE subtask, researchers counted the number of successful catches for the single and dual conditions. There were two characteristics of a successful catch: (1) the participant was correctly alternating hands, and (2) the ball was caught without dropping to the ground, even if bobbled. The researchers reached a consensus on the number of successful catches. Videotapes were viewed again to determine the number of correct subtractions in the dual condition. Researchers decided that an incorrect subtraction (e.g., 100 − 3 = 96) followed by subsequently correct subtractions resulted in only one error. Again, after the researchers reached a consensus, the number was recorded. Collectively, it took two researchers 4–6 min to score each participant’s DTS; it took one researcher less than 4 min to score the DTS.
Statistical Analysis
To establish the feasibility of administering the DTS efficiently outside of the laboratory, we calculated average administration time and we recorded a qualitative description of the testing site. To determine the sensitivity of the DTS, we used paired t tests to compare single- and dual-condition motor performance; the primary outcome measures for both single and dual conditions were gait speed (LE subtask) and number of successful catches (UE subtask). To further examine single- and dual-condition performance, we calculated a dual-task effect (dual-task performance/single-task performance), indicating the percentage of motor task performance under the dual-task condition compared with the single-task condition.
Values greater than 100% represent better performance under dual conditions, whereas values less than 100% represent poorer performance under dual conditions for both subtasks. Correlation analyses were used to test for relationships between the LE and UE subtasks’ dual-task effects. Additionally, the percentage of participants with poorer dual-condition motor performance was identified for each subtask and for parallel administration. In parallel administration, the DTS was considered sensitive if poorer dual-condition motor performance was elicited on either or both subtasks.
Results
Parents of 33 female adolescents consented to testing; 1 participant was excluded because of a previous TBI, which was initially not reported but affected her left UE function. Of the 32 remaining female adolescents (mean [M] age = 13.84 yr), 30 were engaged in at least one competitive sport. No participant took medication that interfered with testing.
The classroom setting allowed more than 6 continuous meters of unobstructed space for a walking path and one unadorned wall, which permitted administration of both subtasks of the DTS. The video camera was set up 3 m away from the walking path and wall on a height-adjustable tripod, which allowed for recording of the DTS without visual obstruction. Setup of masking tape and video camera took between 10 and 15 min on the first day and less than 5 min on each subsequent day. The DTS was administered with all 32 participants in a total of 3 hr over the four provided class periods, with an average administration time of 5.63 min. The LE subtask took an average of 3.40 s (standard deviation [SD] = 0.52) in the single-task condition and an average of 4.75 s (SD = 1.32) in the dual-task condition.
These completion times are comparable with uninjured adult participants’ performance in previously published work; under single-task conditions, adults completed a 6-m obstacle walk in approximately 4 s, and under dual-task conditions (which included a verbal fluency task), they completed the obstacle walk in approximately 4.6 s (Cossette et al., 2014). The UE subtask always took 30 s for both the single- and dual-task conditions. The total time for full DTS administration included providing directions and answering participants’ questions, which resulted in an average administration time of 5.63 min.
Significant differences were observed between single-condition and dual-condition motor performance on both the LE and UE subtasks. In the LE subtask, participants walked significantly slower in the dual condition (M = 1.35 m/s, SD = 0.34) than in the single condition (M = 1.81 m/s, SD = 0.29), t(1, 31) = 8.56, p < .01, d = 1.46 (Figure 1A). In the dual condition of the LE subtask, participants correctly recited an average of 4.7 mo (SD = 2).
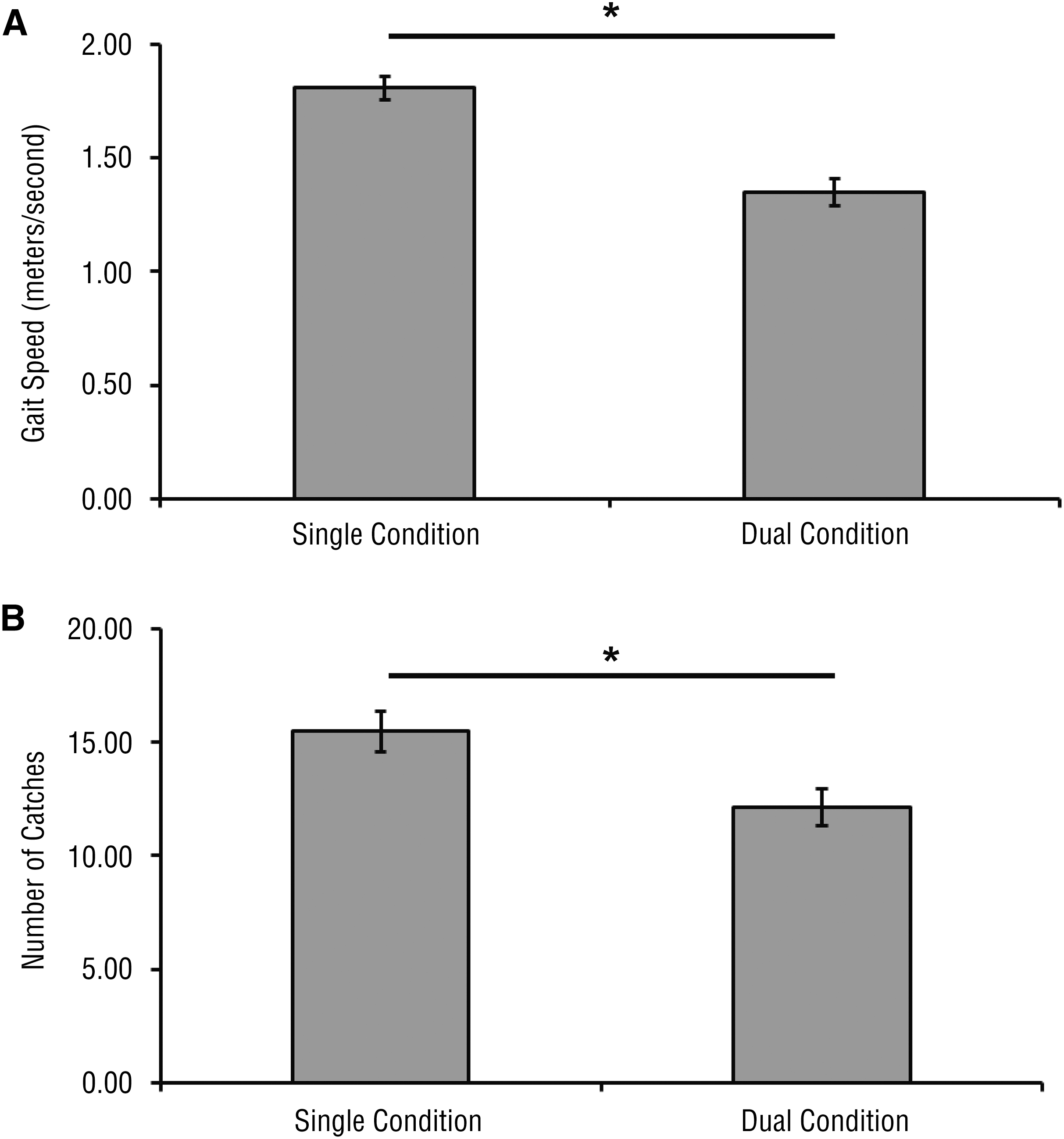
Single- versus dual-condition performance.
In the UE subtask, participants had significantly fewer catches in the dual condition (M = 12.13, SD = 4.48) than in the single condition (M = 15.47, SD = 5.02), t(1, 31) = 6.28, p < .01, d = 0.70 (Figure 1B). In the dual condition of the UE subtask, participants completed an average of 9.9 correct subtractions (SD = 4).
Individually, participants varied in the degree of dual-task effects on both subtasks (Figure 2). One participant walked faster during the dual condition (1.46 m/s) compared with the single condition (1.22 m/s) of the LE subtask (i.e., dual-task effect > 100%). Four participants had 1–2 more catches in the dual condition compared with the single condition of the UE subtask. The range of dual-task effects was similar between the LE (minimum = 37%; maximum = 119%) and UE (minimum = 36%; maximum = 118%) subtasks, but dual-task effects from the subtasks were not significantly correlated (p = .49). Overall, the LE subtask successfully elicited poorer dual-condition motor performance in 97% of the participants. The UE subtask successfully elicited poorer dual-condition motor performance in 88% of the participants. Parallel administration of both subtasks rendered 100% sensitivity in detecting poorer dual-condition motor performance.
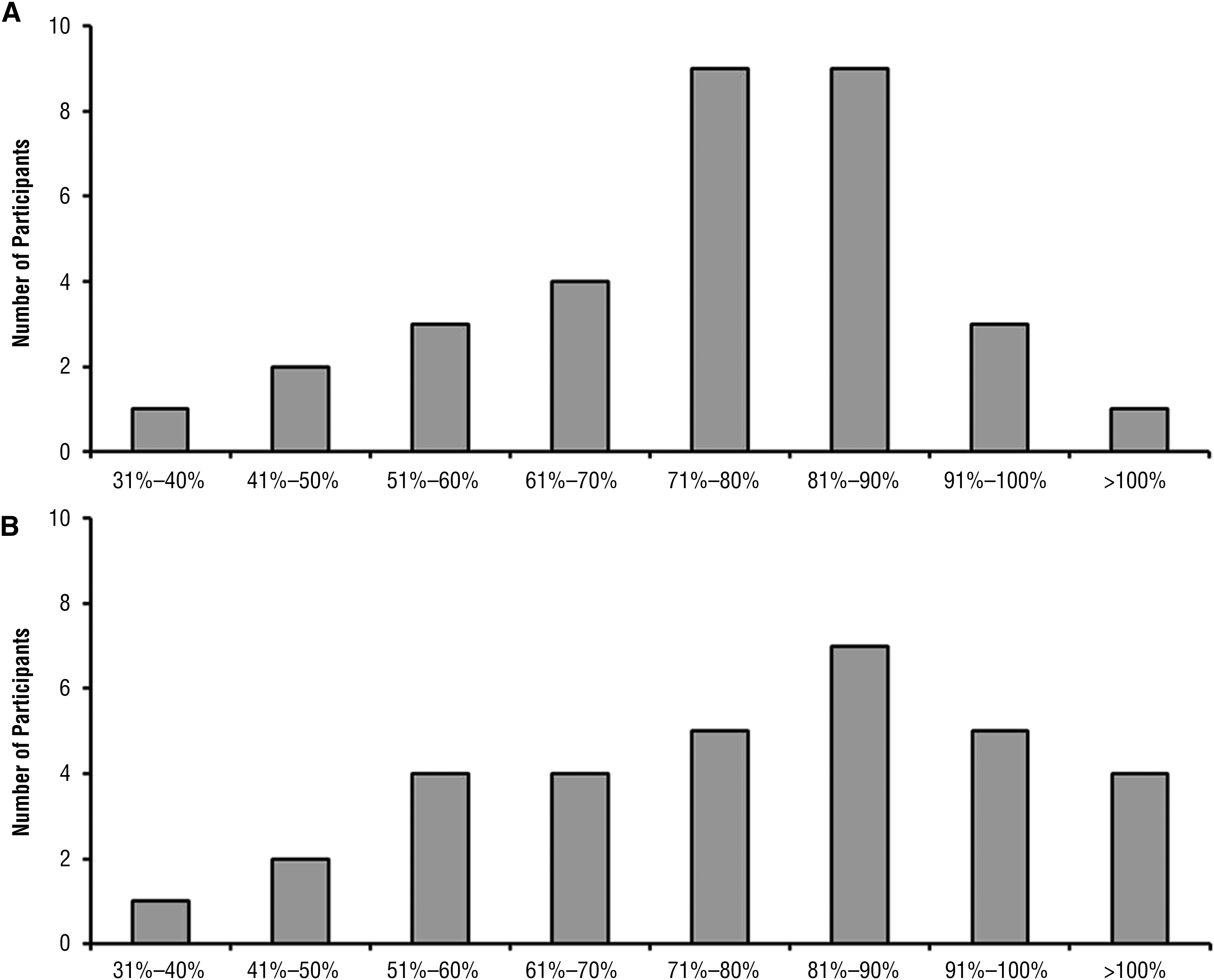
Dual-task effects.
Discussion
Here, in a population of healthy female adolescents, we established that our newly developed DTS could be administered in a time-efficient manner outside of a laboratory setting. We successfully tested 32 participants in a classroom setting in less than a total of 3 hr. We showed that the DTS could be administered for an individual participant in fewer than 6 min on average in any quiet environment with 6 m of unobstructed space and an unadorned wall. We also used video recording to permit two-rater scoring offsite, which facilitated consistent scoring and no loss of performance data.
We found that scoring could be completed quickly—between 4 and 6 min per participant with two raters who reach a consensus, or less than 4 min for a single rater. On average, the total time to complete the DTS with a single rater is less than 10 min, which is shorter than computerized measures that are commonly used in post-mTBI testing (e.g., ImPACT®; Schatz, Pardini, Lovell, Collins, & Podell, 2006), so the DTS could be easily added onto current evaluation procedures. Future research should include single-rater scoring and subsequent testing for interrater reliability. These findings indicate that the DTS has potential for use in a variety of environments, including clinical settings, such as a doctor’s office or outpatient rehabilitation facility, or in recreational facilities, such as in an athletic training room or gymnasium.
The DTS is more comprehensive than other dual-task paradigms because the LE and UE subtasks assess different motor skills used across multiple sports. The absence of correlation between performance on the LE and UE subtasks likely indicates that they were assessing distinct motor domains as we had intended. In future studies, researchers might consider use of other means of assessing visual–motor abilities, including through the use of technology such as the Dynavision
Here, we determined that dual-condition performance of the DTS was generally poorer than single-condition performance on both subtasks. We also saw a similar range in the degree of dual-task effects between the subtasks, although, as noted earlier, dual-task effects from the subtasks were not correlated. This finding likely indicates that individual performance on one subtask would not predict performance on the other subtask, lending further support that they assess different skills and supports the inclusion of differing motor tasks in dual-task paradigms. Likewise, administration of both subtasks was better than independent administration of either subtask because parallel administration of both subtasks had 100% sensitivity for detecting poorer dual-condition motor performance.
This pilot study was designed to test a newly developed screening tool. The primary limitation of this study is the small cohort that was homogeneous in age and sex; however, because the DTS robustly and reliably elicited poorer dual-condition motor performance, it is a strong candidate for further testing. Collecting additional data from uninjured youth across age, sex, sports, and expertise will improve the understanding of the effects of age and training on performance on these tasks. With data from uninjured adolescents, an age, sex, and sport-specific normative dataset could ultimately be developed.
Additionally, on both of the individual subtasks, at least 1 participant failed to demonstrate poorer dual-condition motor performance. This finding is consistent with prior dual-task studies measuring walking speed in adults (Cossette et al., 2014) and adolescents (Howell et al., 2013, 2014, 2016), in which some control participants perform equivalently to or better under the dual condition compared with the single condition, whereas people with mTBI typically consistently show poorer performance under dual conditions.
Future research testing the DTS for adolescents with mTBI may elicit comparable results with these prior studies. Still, it is possible that the DTS is less sensitive to motor deficits than the dual-task assessments conducted in laboratory settings (Dorman et al., 2015; Howell et al., 2013, 2014, 2015, 2016). However, unlike these assessments, the DTS is more portable and practical, and it was designed as a screen rather than a comprehensive motor assessment. Future evaluation of the sensitivity of this DTS to deficits during and after clinical recovery from mTBIs compared with the current gold standard is needed to determine its utility in that population.
Last, we were unable to comment on cognitive performance under the dual-task condition because we did not evaluate performance on the cognitive tasks alone. This outcome limited our ability to understand the interaction of the motor and cognitive tasks. It is possible that the participants who had equivalent or slightly better motor performance under dual conditions would have had poorer dual-condition cognitive performance. In future work, it may be useful to compare single-condition cognitive performance with dual-condition cognitive performance, even if confounding practice effects are present. Additionally, introducing a more challenging cognitive task to either subtask of the DTS may increase the likelihood of eliciting poorer dual-condition motor performance, particularly when examining uninjured control participants.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Participation in sports and recreation has inherent benefits and risks for adolescents. When an adolescent sustains an mTBI, the use of sensitive, practical, and portable measures, such as the DTS, may help to mitigate potential long-term consequences by preventing premature return to high-risk activities.
Occupational therapy practitioners and scientists equally benefit from empirical developments that facilitate safe return to meaningful occupations, such as participation in sports and recreation.
Conclusion
In summary, dual-task paradigms, including this DTS, hold promise as a behavioral measure that may be sensitive to compensatory recruitment of attentional resources for motor task completion (e.g., Risen, Barber, Mostofsky, & Suskauer, 2015). We conclude that these findings from our pilot study indicate that the DTS is a promising measure that merits more evaluation and possible refinement of the subtasks, as described earlier (e.g., using a more challenging distractor cognitive task). The additional sensitivity gained by novel inclusion of an upper extremity, visual–motor coordination task underscores how occupational therapy practitioners can contribute to advancing the work in this critical area by encouraging more holistic assessments. Still, additional research is paramount to a comprehensive understanding of which evaluation tools will emerge as clinically relevant and sensitive measures for monitoring recovery after youth mTBIs.
Footnotes
Acknowledgments
The authors declare no conflicts of interest. This research was supported by National Institutes of Health Grant 5T32HD007414. The authors thank Ms. Souris and the Bryn Mawr School for their assistance with this study.