
Abstract
Feeding interventions that support family relationships enhance children’s daily participation in meaningful occupations at home. A critical review of the literature yielded several premises that support the development of a relationship-based feeding framework. The proposed theoretical framework, based on the Biopsychosocial Model of Pediatric Feeding (Berlin, Davies, Lobato, & Silverman, 2009) and the Ecological Model of Occupation (Dunn, Brown, & Youngstrom, 2003), is presented to guide feeding interventions for children with significant feeding difficulties. A case example that illustrates the practical application of this framework is provided. Further development of relationship-based feeding theory and research is recommended to improve the occupational performance and quality-of-life outcomes for children and their families.
The purpose of this article is to provide occupational therapists with a new framework through which to view feeding practice. I propose the relationship-based feeding framework to stimulate reflection on and conversation about current practice and the need to approach feeding from both an occupational performance and a relational perspective. The framework embraces the core values of occupational therapy, with an emphasis on occupation that provides meaning and quality to one’s life. Observed trends in current feeding practice include a focus on individual performance abilities of a child in clinical settings and minimal family involvement. The relationship-based feeding framework calls on occupational therapists to reexamine current practice and to approach feeding as an occupation that improves quality of life for the child and family throughout the life course.
Premises
This article is based on the following six premises:
Feeding is a primary occupation of children that is necessary for their growth and development (American Occupational Therapy Association [AOTA], 2017). The prevalence rate of feeding problems is reported to be within the range of 25%–45% for typically developing children and to rise to 80% for children with disabilities (Linscheid, Budd, & Rasnake, 2003; Manikam & Perman, 2000). The high prevalence rate supports the need for a framework that effectively addresses a range of feeding difficulties.
Feeding is a social activity and involves a dyadic relationship between the caregiver and the child. Feeding problems may arise from a multitude of factors, yet they always occur within the context of relationships (AOTA, 2017; Berlin, Davies, Lobato, & Silverman, 2009; Davies et al., 2006; Ray, 2015). Therefore, interventions that strengthen the social relationship between the child and the caregiver are essential in feeding practice.
A holistic approach is key to addressing multiple factors while supporting the feeding relationship. Data obtained through a systematic review of the literature support multiple types of feeding interventions (i.e., oral–motor, parent mediated, positioning, behavioral) because of the complex nature of feeding difficulties (Clark & Kingsley, 2013; Howe & Wang, 2013; Lukens & Silverman, 2014; Snider, Majnemer, & Darsaklis, 2011; Williams, Field, & Seiverling, 2010). Although parental and caregiver stress associated with severe feeding difficulties is well documented in the literature (Berlin et al., 2009; Davies et al., 2006; Didehbani, Kelly, Austin, & Wiechmann, 2011; Franklin & Rodger, 2003; Hewetson & Singh, 2009), further research on interventions that reduce stress and support family relationships for feeding is needed (Clark & Kingsley, 2013; Howe & Wang, 2013; Pridham et al., 2005; Ray, 2015).
A family-centered approach is necessary in feeding practice (Clark & Kingsley, 2013). Data obtained through a systematic review of the literature provide support for family involvement in feeding interventions (Howe & Wang, 2013). Families also benefit from guided participation, support, and resources to build their resiliency (Pridham et al., 2005). Although multiple evidence-based interventions are available, not all interventions are applied in practice using a family-centered approach.
Most children with complex feeding problems have a combination of underlying issues that are best addressed by an interdisciplinary team (Berlin et al., 2009; Davies et al., 2006; Marcus & Breton, 2013; Williams et al., 2010). Because feeding, eating, and swallowing are within the scope of occupational therapy practice (AOTA, 2014) and multiple other health science disciplines, differing philosophical positions and approaches are used in practice. Many interventions focus on the individual, medical, or performance factors of the child without addressing the family, the environmental context, or quality of life. A coordinated team approach is needed to address the multidimensional aspects of feeding while working toward the primary goal: enabling meaningful occupations for both the child and the family.
Occupational therapy offers a unique perspective on feeding, eating, and swallowing because it considers all factors involving the person, environment, and occupation and recognizes the “complex dynamics” of the child and family (AOTA, 2014, p. S11). This holistic view of feeding also aligns with the International Classification of Functioning, Disability and Health: Children and Youth Version (World Health Organization, 2007), which emphasizes participation and quality of life within an environmental context of support and relationships.
Definitions
Key terms as used in relation to the framework presented in this article are defined as follows:
Family centered: An approach to service delivery that promotes collaboration and positive relationships with the caregiver and family to influence the child’s needs and occupational performance. The family plays a vital role in assessment, identifies the child’s needs and priorities, and helps the occupational therapy practitioner make decisions regarding services that are based on the best available evidence and family preferences (Clark & Kingsley, 2013).
Feeding problems: Refers to a broad range of difficulties involving self-feeding, eating, and swallowing skills; relational interactions; and mealtime behaviors. This definition excludes feeding difficulties related to food insecurity, obesity, and eating disorders (adapted from Berlin et al., 2009).
Occupational performance: “[The act] of doing and accomplishing a selected action (performance skill), activity, or occupation (Fisher, 2009; Fisher & Griswold, 2014; Kielhofner, 2008) that results from the dynamic transaction among the client, the context, and the activity. Improving or enabling skills and patterns in occupational performance leads to engagement in occupations or activities (adapted in part from Law et al., 1996, p. 16)” (AOTA, 2014, p. S43).
Quality of life: “From an occupational perspective[,] refers to choosing and participating in occupations that foster hope, generate motivation, offer meaning and satisfaction, create a driving vision of life, promote health, enable empowerment, and otherwise address the quality of life (adapted from the Canadian Association of Occupational Therapists [CAOT], 1997, 2002)” (CAOT, 2007, p. 20).
Relational: Something that pertains to the manner in which two or more people communicate, act toward, and interact with each other (adapted from “Relational,” 2015).
Relationship-based feeding framework: A conceptual tool that represents the primary constructs of occupational performance and the child–caregiver relationship to guide feeding practice. It is based on the Biopsychosocial Model of Pediatric Feeding (Berlin et al., 2009) and the Ecological Model of Occupation (Dunn, Brown, & Youngstrom, 2003).
Theoretical Framework
A theoretical framework is necessary to provide guidance in supporting family relationships in feeding practice. The Biopsychosocial Model of Pediatric Feeding (Berlin et al., 2009) and the Ecological Model of Occupation (Dunn et al., 2003) are two complementary models that, when combined, address the complexity of feeding difficulties and guide practice from an occupational and relational perspective.
The Biopsychosocial Model of Pediatric Feeding provides a comprehensive view of the multiple biomedical, psychological, and interpersonal factors that may contribute to the development of feeding problems. It considers the feeding relationship within the context of the social–cultural environment and recognizes the influence of medical conditions and caregiver variables. The model suggests the importance of addressing multiple factors that influence the environmental context and feeding relationship when applying interventions with children with significant feeding problems.
The Ecological Model of Occupation provides a framework to address a broad range of occupational performance difficulties and can be used in collaboration with other disciplines. The model considers the relationship among the person, context, task, and performance but focuses on the uniqueness of the individual performing the task within a natural context. It emphasizes primary social–cultural, environmental, and temporal factors and provides guidance for implementing context-based interventions to improve occupational performance. This model and the Biopsychosocial Model of Pediatric Feeding provide a basis for understanding a relationship-based feeding approach.
Relationship-Based Feeding Framework
The proposed framework combines theoretical components of the previous models to guide feeding intervention from a relational and occupational performance perspective. The primary constructs of the relationship-based feeding framework are listed in Table 1 and illustrated in Figure 1. The framework places the child–caregiver relationship as the central component. It considers complex biopsychosocial and contextual factors that affect the feeding relationship, and it promotes active engagement on the part of the child and caregiver within the context of family relationships, community support, and resources. Health, well-being, and quality of life are the primary outcomes of this approach.
Components of the Relationship-Based Feeding Framework
Note. The relationship-based feeding framework is based on Berlin, Davies, Lobato, and Silverman (2009) and Dunn, Brown, and Youngstrom (2003).
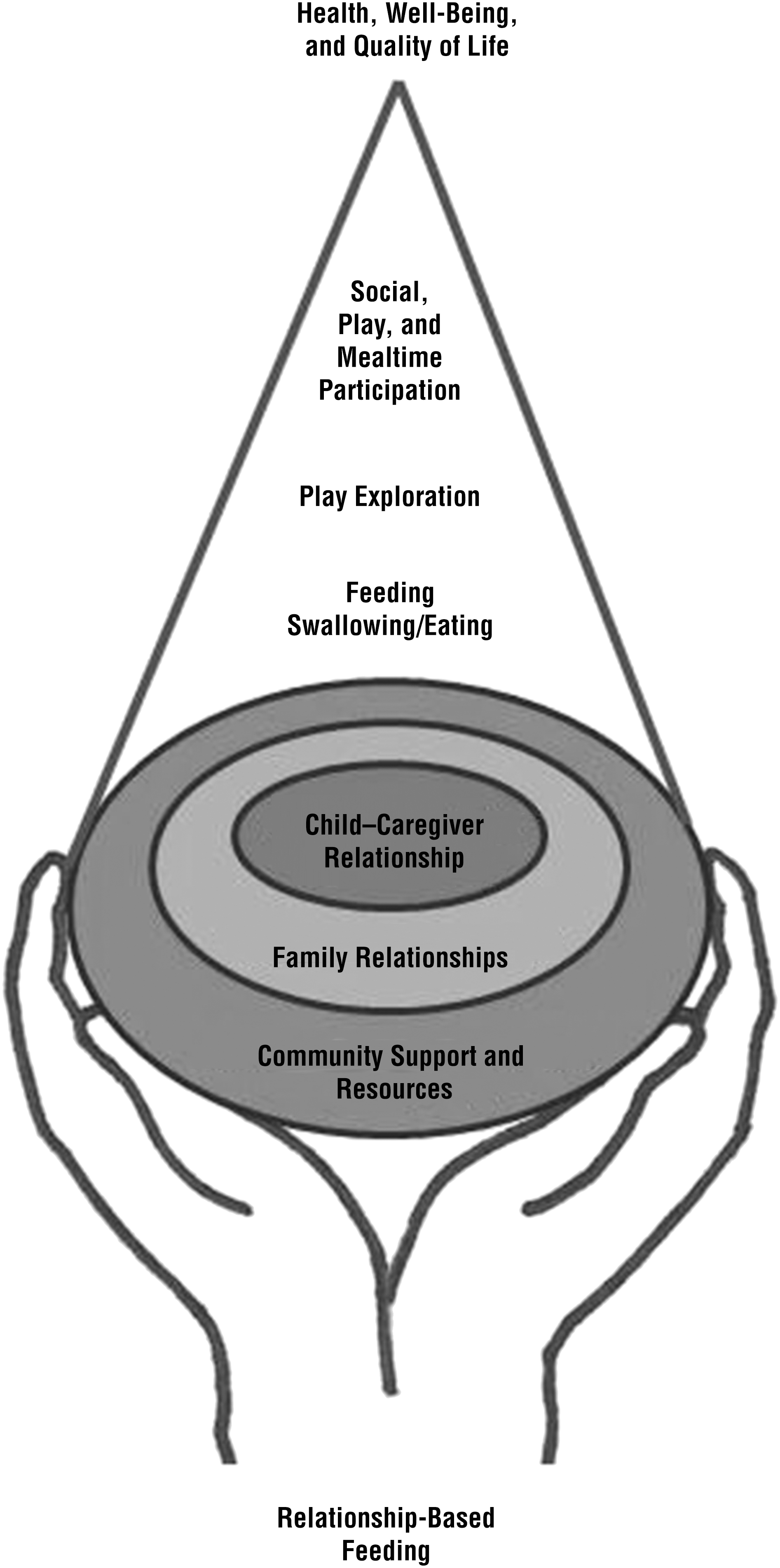
Relationship-based feeding framework.
Key Components of the Framework
The relationship-based feeding framework has five key components. First, it considers individual factors of the child and caregiver that affect the feeding relationship. Child factors may involve problems related to illness, developmental delays, and mealtime behaviors. Caregivers may have limited knowledge of the child’s developmental level or skill deficits, or they may have difficulty understanding the child’s cues, which may lead to stressful feeding interactions. Intervention is individualized for every child and caregiver to build on their unique strengths and to address specific needs to improve child–caregiver interactions during feeding. For example, caregivers may require specific training to improve their perception, understanding, and responsiveness to the child’s cues to support optimal pacing and participation.
Second, the framework considers environmental factors that support the child–caregiver relationship. Environmental modifications may be needed to promote opportunities for child–caregiver interaction and to improve their participation in family occupations.
Third, the framework focuses on engagement in meaningful occupations with an emphasis on improving the quality of participation for all participants. Primary occupations of this framework include eating, swallowing, and feeding; play exploration; and social, play, and mealtime participation. Caregivers play a key role in applying interventions to increase the child’s level of participation in family occupations, such as at mealtimes. Enabling participation in social play and play exploration with food provides social learning opportunities for both the child and the caregiver. Occupational therapy interventions assist caregivers in developing positive and supportive interactions to increase reciprocal engagement as the child learns to explore food and mealtime items in a nonpressured, relaxed manner. Social learning opportunities continue to expand as the child develops and participates in mealtime planning, preparation, and clean-up routines.
Fourth, the framework embraces family-centered practice and addresses feeding within the context of natural settings. The family is an integral part of assessment, goal setting, and intervention and is included in all interventions to the maximum extent.
Finally, interventions are applied within the home, school, and community and include optimal structuring to support positive child and caregiver interactions and occupational participation. The community offers a range of valuable resources to empower families and build resiliency. Resources may improve a family’s access to healthy foods, increase their knowledge of nutrition and feeding, and provide appropriate support to reduce family stress. A relationship-based feeding approach increases community awareness and links families to appropriate resources and supports.
Key Intervention Strategies
The environmental context is a crucial aspect of relationship-based feeding. According to Dunn et al. (2003), the interaction of the child’s individual performance factors and unique social, cultural, temporal, and physical contexts affects occupational performance. Because of this dynamic system, an intervention applied to any component (i.e., person, task, or context) has the potential to change the performance outcome. The relationship-based feeding framework uses the theoretical constructs of the Ecological Model of Occupation yet targets contextual factors that influence feeding and the feeding relationship when applying intervention strategies.
As an example, consider that a feeding intervention may primarily aim to increase the caregiver’s understanding of the child’s sensory processing patterns that are affected by changes made to the environment. Altering or adapting the environment for the child and caregiver may be necessary to provide supportive physical positioning and achieve optimal arousal for feeding. Other types of intervention strategies may involve altering, adapting, or creating an optimal fit among the child’s individual client factors, performance skills, performance patterns, and feeding context. For example, educating caregivers and families about foods that are appropriate for the child’s developmental level (i.e., temporal context) may affect the child’s ability to eat and swallow food safely and prevent negative mealtime experiences such as gagging or choking. Caregivers and families also benefit from information about how to develop predictable mealtime routines with appropriate levels of support and structure to increase participation and reduce family stress. Positioning interventions may alter the physical context to best support the child’s function while promoting opportunities for face-to-face contact and positive family interactions. Feeding problems may also require creative solutions to improve occupational performance. Many families are willing to meet a challenge by finding unique ways to improve the context or feeding task. Family involvement in interventions strengthens relationships and encourages future problem solving.
Application of the Framework
The framework can be used as a primary approach in combination with other evidence-based interventions that support occupational performance and relational feeding principles. In clinical practice, a variety of interventions may be needed to address the unique characteristics of the child, family, and environment. For example, a child with cerebral palsy may require multiple interventions to build oral–motor skills and improve positioning for eating and safe swallowing. Sensory-based interventions may be needed in combination with systematic desensitization to improve the child’s ability to accept touch and explore various foods. Education and coaching may be used to promote family involvement in interventions.
When using the relationship-based feeding framework as a primary approach to feeding, interventions are strategically applied to increase the child and family’s occupational involvement. As an example, an oral–motor intervention can actively involve the parent and support the parent–child relationship by using a playful and socially engaging approach. It would not be considered family centered or relationship based if it was applied solely by the occupational therapy practitioner and did not actively involve the parent through instruction or coaching.
The relationship-based feeding framework emphasizes occupational participation and quality of life within an environment of support and relationships. It may be used with other evidence-based interventions to address the complexity of feeding difficulties.
Case Example
Lily is a 2-yr-old who was initially referred to early intervention at age 2 mo because of prematurity and feeding difficulties. She was born at 29 wk gestation by cesarean section after a high-risk pregnancy. She weighed less than 1,100 g at birth and required an extended hospital stay in the neonatal intensive care unit. Lily was discharged home with a nasal–gastric feeding tube and support from a home visiting nurse. She received diagnoses of gastroesophageal reflux disease and hypotonia, and she has significant developmental delays in gross motor skills, communication, and feeding. Sensory processing concerns were also identified in several areas and appeared to contribute to difficulties with self-care, play skills, and feeding.
Lily has received multiple therapy services through early intervention and outpatient clinics. Additional team support has been provided through her pediatrician, a dietitian, and a neonatal developmental clinic.
Lily’s parents reported significant anxiety when Lily was first discharged home. She received the majority of her calories by nasal–gastric tube because of her poor endurance during oral feedings. Her mother assumed the primary caregiver role and fed Lily most of her bottles during attempted oral feedings. Lily’s father shared child care responsibilities when he was not working and participated in feeding Lily at least once each day.
Both parents were concerned with her poor weight gain and inconsistency in oral feedings. During the first visit with an occupational therapist, Lily’s parents verbalized their expectations for achieving her daily feeding goal primarily through oral feedings and wished to discontinue tube feedings as soon as possible. A variety of positioning, oral support, and environmental interventions were used over the course of 6 wk to improve child–caregiver responsiveness and positive interactions during feeding. Parental involvement was maximized by means of a teaching and coaching approach that involved minimal direct handling by the therapist. Within 6 wk, Lily demonstrated improved feeding skills, eagerly accepted the bottle from both parents, and met her daily feeding goals. During feeding, her parents learned to read Lily’s cues for pacing and engaged in pleasant interactions with her. Once Lily’s parents were no longer concerned with her bottle feeding, the focus of intervention shifted to developing Lily’s sensory–motor skills for mobility and play.
Feeding became a primary concern for Lily’s parents once again when she did not transition to baby food purees by an adjusted age of 9 mo. At this time Lily demonstrated good head control and was able to maintain an erect position in a supportive highchair but had not yet achieved independent sitting. Although Lily continued to take her bottle well, her parents became concerned that she refused all purees and began to turn her head away from an approaching spoon. Intervention focused on improving Lily’s acceptance of a variety of toddler utensils, cups, and foods through play with her parent. Sensory-based interventions were implemented by her parents throughout the day, and Lily was included in family mealtimes as much as possible. Because of her slow progress, Lily was referred for a comprehensive multidisciplinary feeding assessment, but the family did not pursue intervention through this clinic. Additional resources and supports were provided to the family at this time through outpatient and home services.
Lily’s parents learned to follow her lead in play, imitate her actions, and respond to her verbal and nonverbal cues during food play. At mealtimes, they allowed her to explore food on her own terms while modeling eating a variety of foods without pressuring her to eat. Her mother worked on replacing the phrase “Take a bite” by simply describing Lily’s interactions with the food. Although her mother had observed some improvement in Lily’s acceptance of spoon feeding when distracted by an iPad or TV, she realized that Lily was not socially engaged or learning how to eat food. A variety of evidence-based oral–motor, sensory–motor, positioning, and behavioral parent coaching interventions were used to build Lily’s performance skills for eating. Lily’s parents were actively involved in all aspects of these interventions and supported her steady progress. Over time, her parents shifted their focus from the quantity of foods consumed to the quality of feedings and interactions.
Significant improvement in Lily’s performance skills for eating and swallowing purees occurred when Lily was able to sit independently at the adjusted age of 12 mo. Parent education included training on structured mealtimes and providing multiple exposures to healthy foods and food textures that match Lily’s developmental skills. Positive reinforcement through smiles and praise became more natural as Lily participated in family mealtimes and shared enjoyment in eating table foods with her parents.
Lily is now eager for mealtimes, is able to self-feed a variety of soft table foods, and drinks liquids from a cup or with a straw. Her weight continues to be below the 3rd percentile, yet she is following her own curve on the growth chart. Her parents report increased satisfaction with Lily’s eating and drinking skills and family mealtimes and continue to support her positive social–emotional development during feeding. This case example demonstrates how a relationship-based feeding approach maximizes family involvement in intervention with the overall goal of enabling meaningful occupation and quality of life for both the child and family.
Discussion
The proposed relationship-based feeding framework described in this article provides a starting point for further dialogue on occupational therapy feeding practice, theory, and research. The concept of relationship-based feeding is not new to occupational therapists. Historically, occupational therapists recognized the importance of family relationships in feeding practice and have contributed foundational knowledge on this subject (Bazyk, 1989; Kellegrew, 2000; Morris & Klein, 2000; Wolf & Glass, 1992).
Over the past decade, however, research on interventions that support relationships in feeding has been limited. Current pediatric feeding education courses available to practitioners focus on the developmental, physical, behavioral, and sensory components of feeding yet minimize the psychosocial aspect. These courses incorporate some aspects of family-centered practice yet emphasize the relationship between the child and food. This gap in knowledge affects professional practice when occupational therapy practitioners focus on isolated components of feeding and neglect the foundation of relationships that support feeding.
Feeding interventions that build trust and attachment between the child and caregiver strengthen the family bond and promote quality interactions throughout the life course. Because the goal of occupational therapy is to support participation in meaningful occupations, feeding intervention should naturally include the family to effect long-term change and improve quality of life. Because families have varying situations, needs, and preferences, it is very important to communicate a range of evidence-based options and actively involve the family in assessment, goal setting, and feeding interventions.
In family-centered practice, families are the ultimate decision makers and therefore need to be appropriately informed of the evidence and allowed to make choices on behalf of the child. What message is being sent when caregivers are encouraged to sit in a waiting room or are informed of how well their child did in therapy without them? Very seldom have I seen parents decline the opportunity to participate when they are encouraged by the professional to do so. In my experience, most parents want the professional to invite them to participate and are excited to build and hone their skills. The result is that family involvement not only strengthens the child–caregiver relationship but also builds their resiliency, for an increased chance of long-term success.
Although it may be challenging to address feeding in natural settings, the positive long-term impact on the child and family makes this a worthwhile endeavor. Foundational knowledge in biopsychosocial theory positions occupational therapy practitioners to reach beyond the medical model into community practice. Our core values call us to be leaders of change that empowers families. The relationship-based feeding framework begins this journey of self-examination and allows occupational therapy practitioners to view occupational feeding practice through a new lens, with the goal of improving quality of life for children and families.
Conclusion
Evidence-based, family-centered practice is crucial to meet the occupational needs of children and their families. Current evidence suggests the need for a comprehensive feeding approach that addresses individual needs and supports family relationships. In this article, I have identified the child–caregiver relationship as the primary focus when applying feeding interventions. The relationship-based feeding framework is proposed as a tool to encourage reflection and to stimulate dialogue on occupational therapy practice, theory, and research related to feeding.