
Abstract
Self-esteem refers to a person’s sense of his or her worth (Blascovich & Tomaka, 1991). High self-esteem is important for stable personal development (Brooks, 1992) and for life satisfaction (Borg et al., 2008). Adolescents with low self-esteem have poorer mental and physical health, worse economic prospects, and higher levels of criminal behavior during adulthood (McGee & Williams, 2000; Orth, Robins, & Roberts, 2008; Trzesniewski et al., 2006). In women, self-esteem has been shown to be correlated with active employment, maintenance of intimate relationships, and health-promoting behavior (Nosek, Hughes, Swedlund, Taylor, & Swank, 2003).
Self-esteem has been reported to be lower in adolescents with cerebral palsy (CP; Riad, Broström, & Langius-Eklöf, 2013), especially girls (Magill & Hurlbut, 1986), and in women with disabilities (Nosek et al., 2003) than in matched controls. One of the main factors underlying these differences is likely to be functional ability. Alterations in body functions and structure directly affect functional capacity, hindering the performance of activities of daily living (ADLs). These difficulties in function may, in turn, cause anxiety and psychological distress; limitations in social participation and in personal and work lives; and reduced self-esteem (Horsman, Suto, Dudgeon, & Harris, 2010). Nevertheless, few studies have addressed the relationship between functional ability and self-esteem in people with disabilities. Most of those that have done so were restricted to adolescents (Manuel, Balkrishnan, Camacho, Smith, & Koman, 2003; Riad et al., 2013) or young adults (Gannotti, Minter, Chambers, Smith, & Tylkowski, 2011; Magill-Evans & Restall, 1991) with CP or to stroke patients (Chang & Mackenzie, 1998); based on small samples (Magill-Evans & Restall, 1991; Manuel et al., 2003); restricted to those who were able to walk (Riad et al., 2013); or conducted more than 10 yr ago.
To fill this gap, we conducted a study with the objective of assessing whether functional capacity, with respect to ADLs, predicted self-esteem in a sample of adults and young people with CP. CP comprises a group of movement and posture disorders, caused by a nonprogressive insult to the developing brain of the fetus or young infant, that may result in functional limitations (Bax et al., 2005). Sensory, cognitive, perceptive, communication, or behavioral alterations or growth disorders may also be present. The prevalence of CP in Europe is 1.77 per 1,000 live births (Sellier et al., 2016), and 46% of children with CP are unable to walk unaided at age 5 yr (Beckung, Hagberg, Uldall, & Cans, 2008).
We chose CP as the disability of interest because its effects are present throughout the life course, including the critical periods of childhood and adolescence when both functional skills and self-esteem are developing, and because it manifests as a range of impairments whose severity varies from mild to severe. We hypothesized that people with better functional ability would have higher self-esteem.
Method
Participants
The inclusion criteria were (1) a diagnosis of CP, (2) communication ability (oral, written, or alternative), (3) ages 16–65 yr and resident in Spain. Because of the absence of population-based registers in Spain of people with CP, we used convenience sampling. The principal investigator (PI; Espín-Tello) developed a database of all centers in Spain that she considered accessible, including schools, day care centers, residential homes and occupational centers for people with special needs, and associations for people with physical impairments. She next sent an information sheet about the study to the manager of each center, asking him or her to bring it to the attention of possible participants and, if necessary, their family or legal guardian. She then contacted those who showed an interest in participating to resolve any queries and provide further information. Those who agreed to participate were interviewed after they—or their legal guardian—had read and signed a consent form.
Data
The PI interviewed all participants face to face in their school, day care center, or residential home between January 1, 2013, and December 31, 2014, to assess self-esteem and functional capacity and capture the sociodemographic and impairment characteristics summarized in Table 1. Presence or absence of intellectual impairment was obtained from clinical records with the participant’s consent, as was information not available from the participant or information about which he or she was unsure. Questions were repeated and explained in more detail if necessary. Participants who did not understand the questions after such explanations were excluded. Eight people with anarthria were interviewed using computer-aided methods or pictograms.
Distribution of Sociodemographic Variables, the Barthel Index, and the Total Score of the Rosenberg Self-Esteem Scale
Note. BI = Barthel Index; M = mean; RSES = Rosenberg Self-Esteem Scale; SD = standard deviation.
The p values were derived using the Mann–Whitney test for dichotomous variables and the Kruskal–Wallis test for other variables. Statistically significant (p < .05) values are in
Outcome Variable.
We evaluated self-esteem using the Total score of the Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1965). This instrument has been widely used in studies of self-esteem in the general population (Roth, Decker, Herzberg, & Brähler, 2008; Sinclair et al., 2010) and among people with disabilities (Blair, 1999; Chang & Mackenzie, 1998; Manuel et al., 2003; Nosek et al., 2003). It has been translated into Spanish (Martín-Albo, Núñez, Navarro, & Grijalvo, 2007) and has shown excellent psychometric properties in populations in the United States (Sinclair et al., 2010), Germany (Roth et al., 2008), and Spain (Vázquez-Morejón, Jiménez, & Vázquez-Morejón, 2004); Item Response Theory has confirmed its unidimensionality (Roth et al., 2008). The RSES was developed for use with adolescents but has since been widely used with a variety of groups, including adults. It consists of 10 items that address global feelings of self-worth, 5 targeted positively and 5 negatively. Each item is scored on a Likert-type scale with four categories of response (1 = strongly agree, 2 = agree, 3 = disagree, and 4 = strongly disagree); negatively targeted items are reverse scored. We summed these responses to give a total score that could range from 10 (low self-esteem) to 40 (high self-esteem). Permission to use this scale was granted by BiblioPRO (http://www.bibliopro.org/).
Putative Predictor.
We evaluated functional capacity using the Barthel Index (BI; Mahoney & Barthel, 1965). This instrument has been widely used in rehabilitation research, in which it has been shown to have excellent reliability and validity (Cohen & Marino, 2000). It has been used in children and young adults with CP (Ketelaar, Vermeer, & Helders, 1998; van der Dussen, Nieuwstraten, Roebroeck, & Stam, 2001), is brief and simple to administer, and has been translated into Spanish (Baztán et al., 1993). It consists of 10 items that evaluate aspects of functional capacity with respect to ADLs: feeding, bathing, grooming, dressing, bowels and bladder management, toilet use, transfers (e.g., bed to chair and back), mobility (on level surfaces), and stairs. Responses have two, three, or four possible categories, each of which is assigned a number of points depending on its perceived importance (Mahoney & Barthel, 1965). These points are summed to give a total score that can range from 0 (low functional capacity) to 100 (high functional capacity). Permission to use this scale was granted by the Stroke Center (Dallas, TX).
Covariates.
Participants’ sociodemographic characteristics are listed in Table 1. Given that any relationship between self-esteem and functional capacity might differ between men and women, sex was included as a potential effect modifier. Because age was an extraneous variable likely to be correlated with both the outcome (self-esteem) and the predictor (functional ability), it was regarded as a potential confounder (Rothman & Greenland, 1998). Education, employment, marital status, and living arrangements were postulated as possible mediating variables that might be on the pathway between functional capacity and self-esteem. Variables describing impairments—walking ability, intellectual disability, and neuromotor disorder—were recorded. Categories of variables including less than 10% of participants were amalgamated with closely related categories.
Sample Representativeness.
Spanish census data indicate that, among people with CP in Spain age 6 yr and older, 52% are male (Instituto Nacional de Estadística, 2008), compared with 51% in our sample (ages 16–65 yr). These data did not report the breakdown by age or impairment of people with CP in Spain, but among the general population in Spain ages 16–65 yr on January 1, 2014, 15%, 46%, and 39% were in age groups 16–25, 26–45, and 46–65 yr, respectively (Instituto Nacional de Estadística, 2016), compared with 11%, 54% and 35%, respectively, in our sample. Data recorded on 13 population-based registers of people with CP in Europe indicate that 52% were able to walk (Surveillance of Cerebral Palsy in Europe, 2002), compared with 23% in our sample.
Statistical Analysis
We first summarized the distribution of RSES and BI scores and the covariates. To compare BI and RSES scores between groups with different sociodemographic and impairment characteristics, we used the nonparametric Mann–Whitney U test for dichotomous variables and the Kruskal–Wallis test for polytomous variables (Altman, 1990).
Hypothesis Testing
To analyze the relationship between the RSES and BI, we initially used simple linear regression (Altman, 1990), with RSES score as the outcome and BI score as the predictor. To assess whether the effect differed between sexes, we repeated this for males and females separately. The model with both sexes combined was then adjusted for each covariate in turn. Both RSES and BI were treated as continuous variables. Covariates were treated as categorical variables. The largest group was chosen as the reference group to yield narrower confidence intervals for estimated effects in nonreference groups; similar categories were amalgamated if they were not significantly different. We checked that the final model satisfied the assumptions of linear regression (Altman, 1990). Significance was set at p < .05.
This study was approved by the Departamento de Fisiatría y Enfermería of the Faculty of Health Sciences of the University of Zaragoza and by the Clinical Research Ethics Committee of Aragón.
Results
A total of 108 people participated in the study. The mean age of the sample was 41.3 yr. The average RSES score was 32.0 (standard deviation [SD] = 5.2, range = 18–40). The median BI score was 37.5 (range = 0–100), an indication that most participants had severe functional dependence.
Descriptive Statistics
The sample included similar proportions of men (51%) and women (49%; Table 1). Most participants (89%) were older than age 25 yr. Approximately 20% had completed higher education, but most had not progressed beyond primary school. Most were unemployed or pensioners, and the most frequent marital status was single. Almost half were living in a care home, and only 7% were living independently. Most participants (81%) had spastic CP, 77% were unable to walk without help, and 19% had intellectual impairment. Both RSES and BI scores were significantly (p < .02) higher among people with a higher level of education, in active employment, and living independently or with family.
Hypothesis Testing
Figure 1 shows the relationship between RSES and BI scores along with the simple linear regression line and its 95% confidence interval (CI). The regression coefficient was 0.047, 95% CI [0.017, 0.078], p = .003; see first line of Table 2), indicating that the RSES score increased on average 0.047 points when the BI increased 1 point. The R 2 was 8%, reflecting the wide scatter of points seen in Figure 1 and indicating that the BI explained only 8% of the variation in the RSES. Residuals from this model were checked visually and showed no indication of deviations from the assumptions of homoscedasticity, linearity, and normality that underlie linear regression or of outlying points that could have had undue influence on the model. The relationship was similar for both sexes (regression coefficient = 0.038, 95% CI [−0.004, 0.081] for men and 0.059, 95% CI [0.011, 0.107] for women). Adjustment for age as a possible confounder made little difference to this relationship (see Table 2); the regression coefficient for the BI remained virtually unchanged and highly significant, although participants ages 46–65 yr had significantly lower RSES scores than others.
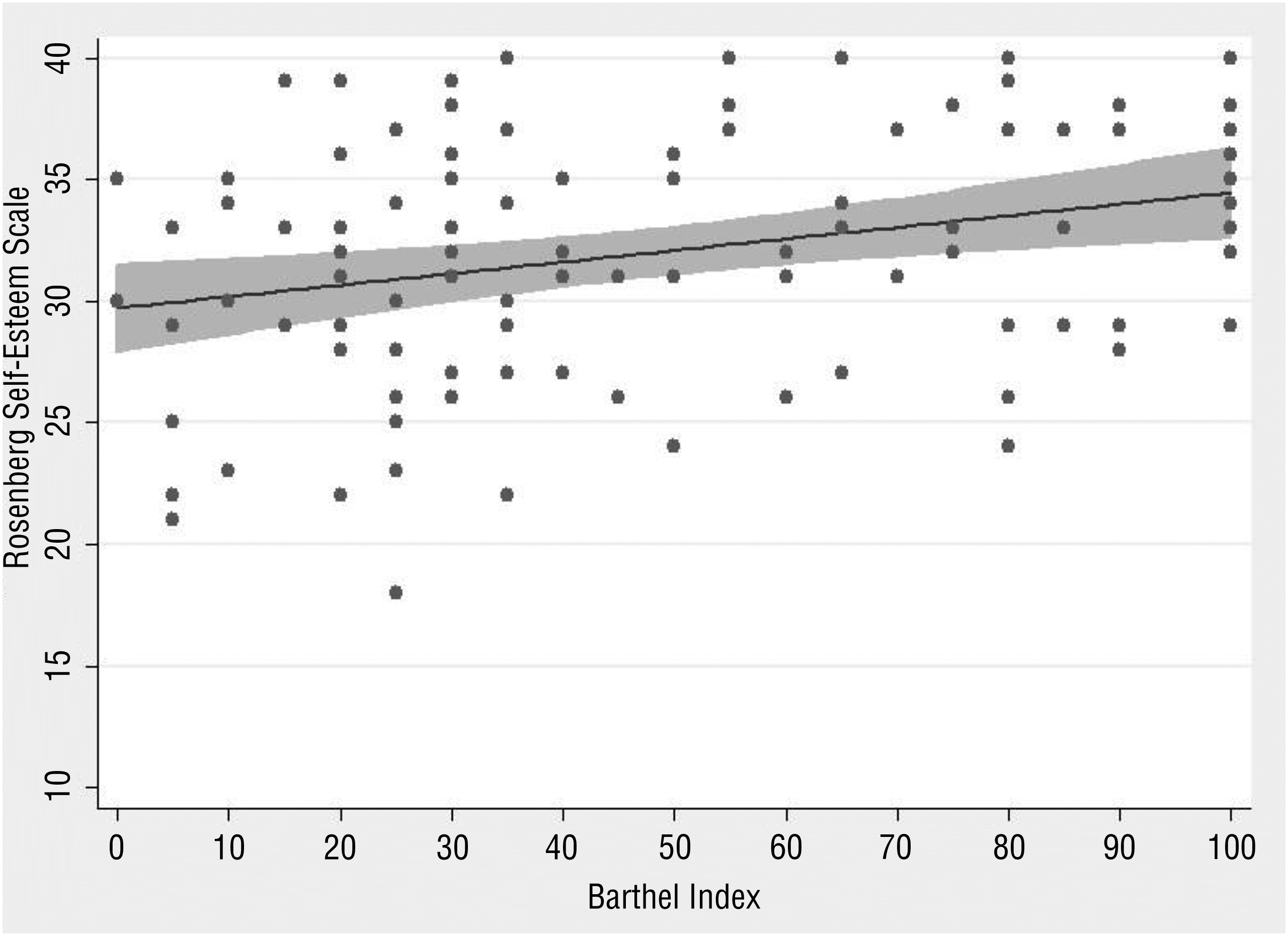
Scatterplot of the Total scores on the Rosenberg Self-Esteem Scale and the Barthel Index, showing the estimated regression line and its 95% confidence interval in shading.
Regression of the Total Score of the Rosenberg Self-Esteem Scale on the Barthel Index, Adjusted For Sociodemographic Variables
Note. Empty cells indicate data that were not applicable. Statistically significant values (p < .05) are in
We included each potential mediating variable in the regression in turn (see Table 2). Education, employment, and living arrangements were significant: Participants with higher education had a higher RSES score than others by an average of 3.8 points, 95% CI [1.4, 6.1]; those who lived independently or with family had a higher RSES score by 3.7 points, 95% CI [1.4, 5.9]; and those who were students or in active employment had a higher RSES score by 3.3 points, 95% CI [0.9, 5.8]. However, inclusion of employment or living arrangements resulted in the regression coefficient for the BI decreasing substantially and becoming nonsignificant, reflecting the high correlations between these covariates and the BI (p from Mann–Whitney test < .002). The models that included education and living arrangements accounted for the most variance in the RSES scores (16%). After excluding 16- to 25-yr-olds who might not have completed their education, entered employment, or started living independently, these effects changed little. Because education, employment, and living arrangements were highly correlated (p from χ2<.0001), it was not possible to develop a more complex model that would have allowed us to disentangle their effects.
Discussion
We found a statistically significant (p = .003) relationship between the BI and RSES, which increased by an average of 0.047 points for each increase of 1 point in the BI. This implies that, for example, an increase of 40 points on the BI was associated with an average increase of 40 × 0.047 = 1.82 points on the RSES, which is just more than one-third of the standard deviation (5.2) of the RSES in the sample. The statistical model was robust: The relationship was similar in men and women, consistent across the entire range of the BI, and unconfounded by age and did not rely on any influential points. Further strengths of our study are that all interviews were conducted face to face by the same person, who ensured not only consistency but also a complete absence of missing data, despite the collection of a large amount of information describing sociodemographic factors.
Although we found that functional capacity was a statistical predictor of self-esteem, it is difficult to infer that this relationship is causal. In principle, the most convincing evidence for causality is provided by longitudinal studies, but these may not be enlightening in populations such as those we have studied in which disability is stable over time. Nevertheless, the robustness of the association found in our cross-sectional study suggests that functional capacity influences self-esteem.
More education, active employment, and living independently or with one’s family were also statistical predictors of higher self-esteem. However, these sociodemographic factors were so highly correlated with each other and with the BI that it was difficult to determine the underlying factor. They may, as postulated, be on a causal pathway between functional capacity and self-esteem; alternatively, they may be a consequence of higher self-esteem (Nosek et al., 2003). Indeed, both pathways could be simultaneously operational (Kline, 2010).
We compared our findings with those in the literature and found only three studies that had considered self-esteem in adults with CP (Gannotti et al., 2011; Magill-Evans & Restall, 1991; Riad et al., 2013). Consistent with our findings, Riad et al. (2013) found that, among 44 people with CP who could walk, deviations of arm and leg movements were inversely correlated with self-esteem, although the effect was not statistically significant. In contrast to our findings, Gannotti et al. (2011) reported that self-concept was not associated with gross motor function or operational independence in 64 people with CP, and Magill-Evans and Restall (1991) found no association between education and self-concept in 19 adults with CP. The differences between these findings and ours may be partly due to their small sample sizes and younger participants (average age = 26 yr).
Research on closely related populations supports our findings. In a study of adolescents with CP, Manuel et al. (2003) found that self-esteem was significantly correlated with physician-assessed functional ability. In a cross-sectional study of 881 women, approximately half of whom had disabilities, Nosek et al. (2003) found that self-esteem was significantly associated with both disability and employment. Although, like us, they postulated that disability influenced self-esteem, they assumed that self-esteem influenced employment, whereas we assumed the opposite direction of causality.
Limitations and Future Research
Selection bias may have arisen in two ways. First, because of the lack of population-based registers of people in Spain with CP, we were unable to select a random sample from all Spanish people with CP. Thus, our sample overrepresented older adults and those with more severe impairment. However, selection bias is more likely to affect estimates of means than of associations, which were the statistic of interest in the current study (Korn & Graubard, 1999).
Second, our study was conducted in Spain, which could compromise its relevance to other countries. However, societal attitudes toward disability in Spain appear to be close to the average of a diverse range of countries (Room, Rehm, Trotter, Paglia, & Ustun, 2001). Furthermore, Spain is one of the 171 countries that have ratified the United Nations Convention on the Rights of Persons With Disabilities (United Nations, 2006), which obliges states to promote mobility, independent living, education, an accessible environment, employment, and social participation for people with disabilities. Although the United States has not ratified this convention, the Americans With Disabilities Act of 1990 (Pub. L. 101-336) has similar aims. Both frameworks address the situation during childhood, when functional skills and self-esteem are developing. Therefore, the results of our study are likely to be applicable outside Spain, given that the countries that subscribe to these legal instruments are likely to have similar facilitators and barriers to disability.
In addition, intellectual or communication difficulties may have resulted in erroneous responses, which could have attenuated the estimate of the relationship between self-esteem and functional capacity. Finally, interviewer bias may have arisen because the sole interviewer had the same pathology as those interviewed. This may have resulted in interviewees responding more openly with more confidence, and possibly exaggerating.
Future studies should use random sampling, stratified by age, so that the results can be generalized to the wider population of people with CP. Longitudinal studies would allow stronger inferences about causality. A larger sample would allow one to conduct an analysis using structural equation modeling, a multivariate technique used to estimate and test supposed causal relationships (Kline, 2010). National population-based registers of people with CP should be created in Spain, to facilitate epidemiological studies of higher quality, which would allow a better understanding of the prevalence of CP and of the situation and needs of those affected. Future studies should also consider additional factors that might influence self-esteem of people with CP, in particular personality traits such as the Big Five: openness to experience, conscientiousness, extraversion, agreeableness, and neuroticism (Karwowski, Lebuda, Wisniewska, & Gralewski, 2013).
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
It is important that occupational therapy programs help people with impairment to perform ADLs as independently as possible. In addition to the intrinsic benefits gained, our study shows this is likely to lead to higher self-esteem.
By working with individuals to improve function and advocating for improved accessibility, occupational therapy practitioners can facilitate access to higher education, independent living, and active employment.
Conclusion
Greater functional capacity predicts higher self-esteem in people with CP. It is likely that education, employment, and independent living mediate the effect of functional capacity on self-esteem. National policies should facilitate, through the removal of social, physical, and attitudinal barriers, the access of people with severe impairment to higher levels of education, homes in which they can live independently, and an active working life.
Footnotes
Acknowledgments
We thank all participants in the study and all professionals and colleagues who helped recruit the sample. We also thank Allan Colver for helpful comments on the article.