
Abstract
Self-efficacy refers to a person’s confidence in his or her ability to manage situations with the skills he or she possesses. Additionally, self-efficacy is the foundation of motivation and action that lead to behavioral change (Bandura, 1977; Riazi et al., 2004). People with higher self-efficacy are more likely to set challenging personal goals, persist in achieving them, and feel more capable of reaching them (Bandura, 1977; Rigby et al., 2008).
In people with multiple sclerosis (MS), increased self-efficacy has been related to enhanced quality of life, their own perceived health status, positive adjustment to the disease, and increased motivation and engagement in meaningful activities (Motl, McAuley, Wynn, et al., 2013; Mullen et al., 2012; Ng et al., 2013; Schmitt et al., 2014). Conversely, people with MS with decreased self-efficacy experience more depression (Shnek et al., 1995) and loneliness (Beal & Stuifbergen, 2007; Fry & Debats, 2002). People with MS have reported increased loneliness with increased isolation, decreased social support, fewer social contacts, and stigmatization (Beal & Stuifbergen, 2007). However, there is limited literature pertaining to loneliness in MS despite its prevalence (Beal & Stuifbergen, 2007).
Although self-efficacy plays an important role in everyday life, only a few studies have examined treatments designed to improve self-efficacy in people with MS (Riazi et al., 2004). The results of these studies provide evidence that self-efficacy may be improved in people with MS (e.g., Graziano et al., 2014; Jongen et al., 2014; Motl, McAuley, & Sandroff, 2013; Motl, McAuley, Wynn, et al., 2013; Ng et al., 2013; Rigby et al., 2008; Thomas et al., 2013). These studies focused on education and self-management (i.e., educating participants on healthy living, nutrition, exercise) or on participation in recreational activities. Occupational therapists should assess their clients’ level of perceived self-efficacy and implement treatments to improve occupational performance and perceived self-efficacy. The treatment in the current study combines educational and performance-based components related to socialization and participation.
This study examined the efficacy of a treatment program for people with MS called Community Reintegration for Socially Isolated Patients (CRISP), which aims to improve self-efficacy. A detailed protocol of the CRISP program has been published (Kalina & Hinojosa, 2016). The program is an occupation-based intervention that uses education and self-management strategies to address self-efficacy during the performance of functional daily living tasks of recreation and socialization. We hypothesized that compared with the control group, participants in the treatment group would demonstrate significant improvements in self-efficacy. Possible effects of the intervention on more distal outcomes were also tested, specifically, whether improved self-efficacy reduced symptoms of depression and feelings of loneliness in people with MS. We hypothesized that participants who improved their self-efficacy would report lower levels of loneliness and depression.
Method
Study Design
A pretest–posttest randomized experimental control group superiority trial design compared the effects of participation in the CRISP intervention program by the experimental group with a control group that received routine neurological treatment. The study was done at an urban comprehensive outpatient MS center that serves more than 2,500 people with MS.
Participants
Participants consisted of 91 people with a diagnosis of MS according to McDonald’s diagnostic criteria (Polman et al., 2011). Potential participants contacted the first author (Kalina) by responding to an advertisement for the study at the MS center. The first author screened potential participants according to the following inclusion criteria: between ages 18 and 70 yr; able to understand and write English at a sixth-grade level, as determined by the Wide Range Achievement Test–Revised (Glutting & Wilkinson, 2005); agree to participate in 12 group sessions over 12 wk; and agree to travel to the MS center and outing destinations. Potential participants who had a history of neurological disease aside from MS, a history of alcohol or drug abuse, or major psychiatric disturbance were excluded. Before enrollment, participants signed a consent form approved by the institutional review board that indicated their willingness to participate.
The first author randomly assigned participants into two groups: experimental (n = 51) and control (n = 40). Table 1 summarizes the participant demographics. The experimental and control groups did not differ statistically on years of education, months since diagnosis, gender composition, or disease subtype. However, participants in the experimental group were older and reported more disability, as determined by the Patient Determined Disease Steps (PDDS; Hohol et al., 1995, 1999), than those in the control group. On average, participants in the control group presented with mild disability, whereas participants in the experimental group used a cane, single crutch, or some other form of support. Additionally, more people in the control group were employed than in the experimental group.
Experimental and Control Group Baseline Demographics
Note. M = mean; MS = multiple sclerosis; PDDS = Patient Determined Disease Steps; PP = primary progressive; RR = relapsing–remitting; SD = standard deviation; SP = secondary progressive.
Measurements
Proximal Outcomes.
Two self-efficacy measures were chosen to be primary outcome measures to examine the consistency of the results. In the General Self-Efficacy Scale (GSES; Schwarzer & Jerusalem, 1995), participants rated 10 questions about self-efficacy on a scale of 1 (not true at all) to 4 (exactly true). Summed scores range from 10 (low self-efficacy) to 40 (high self-efficacy). The GSES has good reliability and validity (Scholz et al., 2002; Schwarzer et al., 1997; Schwarzer & Jerusalem, 1995). The Multiple Sclerosis Self-Efficacy (MSSE) Scale (Rigby et al., 2003) is a 14-question scale with scores ranging from 14 (low self-efficacy) to 84 (high self-efficacy). This scale has high internal consistency (Cronbach’s α = .81) and test–retest reliability (r = .81, p < .001; Rigby et al., 2003).
Distal Outcomes.
Two measures were used to assess the distal outcomes of loneliness and depression. The Revised UCLA Loneliness Scale (Version 3; Russell, 1996) consists of 20 questions about loneliness asking participants to rate each question from 1 (never) to 4 (always). Higher scores indicate greater degrees of loneliness. The scale has high internal consistency (α = .89–.94) and test–retest reliability (r = .73) and established convergent validity (Russell, 1996). The Chicago Multiscale Depression Inventory (CMDI; Nyenhuis et al., 1998) is a 50-item measure of depression. The items on the scale consist of a single word describing feelings, and participants rate each item on a scale from 1 (not at all) to 5 (extremely). The CMDI has adequate reliability and validity in people with MS (Chang et al., 2003).
Procedure
Recruitment ran from January 2014 to December 2014. After screening, 118 participants were eligible to participate. Participants were randomly assigned by the first author (Kalina) to either the experimental or control group before baseline testing using block randomization and a random numbers table, and thus group allocation was not concealed. A blinded research assistant who did not know whether participants were in the experimental or control group collected baseline data and follow-up data after 12 wk for both groups. Participants who could not return within 14 wk from baseline were dropped from the study. Figure 1 illustrates the procedural flow of the study and the number of participants who dropped out during the study and their reasons for dropping out. The first author did not make any changes to the study protocol (eligibility, testing times, and intervention) after recruitment began.
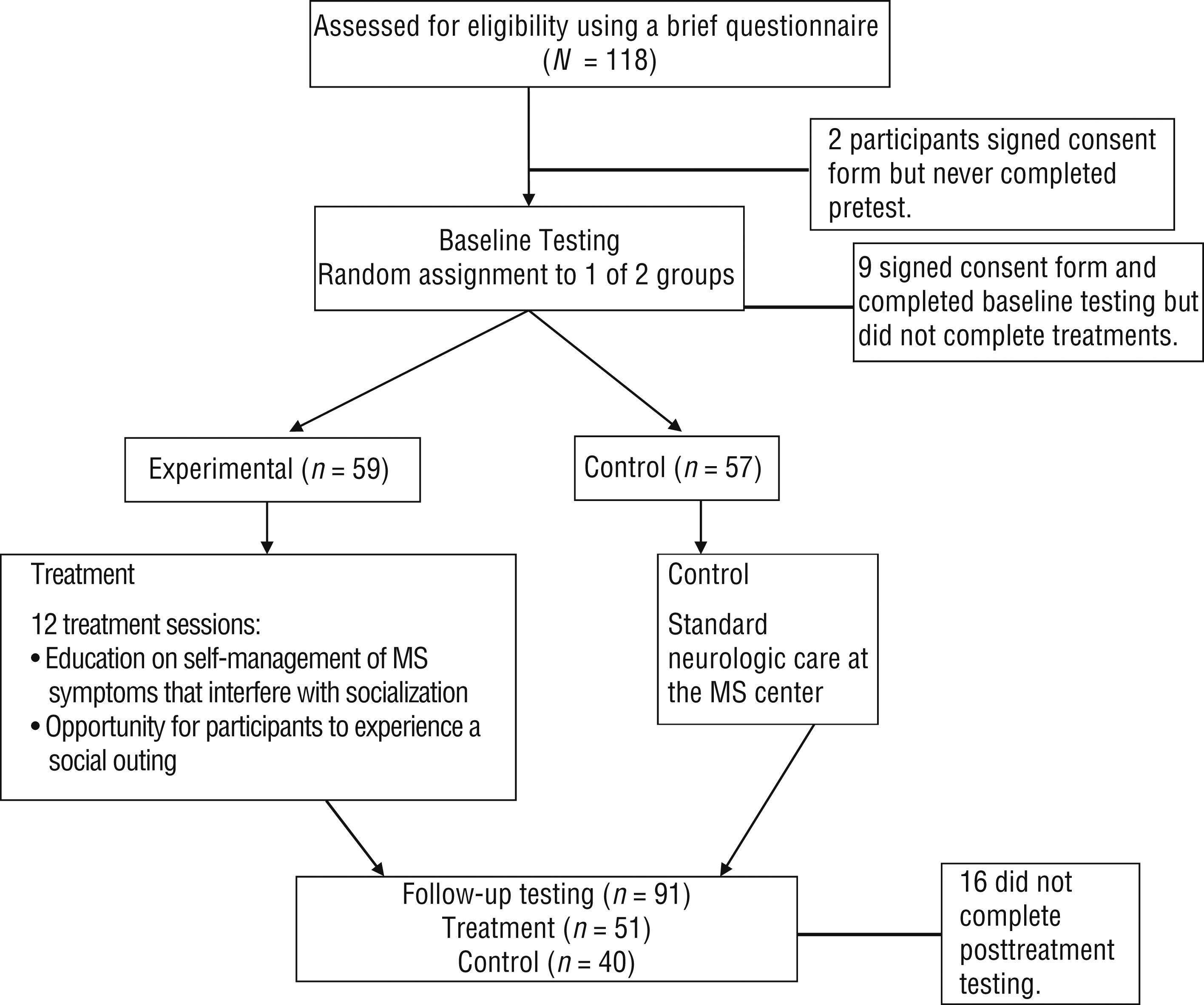
Participant flow diagram.
Participants who completed the entire study and those who were dropped from the study were compared on several background and pretest variables. The two groups did not differ regarding age, gender, type of MS, or disease duration. They did differ on employment status; 46% (n = 11) of those who did not complete the study were employed, whereas only 24% (n = 22) of those who completed the study were employed. No adverse effects occurred during this trial.
Experimental Group.
The CRISP program (Kalina & Hinojosa, 2016; Fromm-Kalina et al., 2007; Fromm-Kalina et al., 2008) is composed of two types of groups: educational and social outing. Educational sessions and social outings were held 4–8 times per week. Participants selected groups from a list provided to them and were required to attend any 12 group sessions over the 12 wk. Participants were required to participate in both social outings and educational groups. Participants could take the program over 12 wk or attend the 12 required sessions in less than 12 wk.
The educational groups focused on teaching self-management strategies (e.g., thoughts, goals, plans, acts) for symptoms that prevent social interactions of any kind, especially social outings. Each session, led by the first author, lasted 45 min and provided information about compensatory strategies of managing MS symptoms, awareness of disability rights, minimizing costs while participating in social activities, and assertiveness skills.
Social outing groups consisted of 4–10 participants. Participants were responsible for their transportation to outing destinations, because negotiating transportation independently was a topic of the educational group and is part of an actual social experience. The social outings took place in various locations, such as museums or baseball stadiums, and offered an opportunity for participants to experience and test what they were learning in the educational groups. Participants had to attend at least one social outing over the course of the intervention.
Control Group.
The control group did not attend any intervention groups and received their usual care at the center (i.e., follow-up with a neurologist or nurse, physical therapy, occupational therapy). After administration of the follow-up outcome instruments, participants in the control group were given the opportunity to participate in the CRISP program.
Data Analysis
Differences between the CRISP intervention group and the control group on self-efficacy were tested by analyses of covariance (ANCOVA) with the self-efficacy score after treatment as a dependent variable and group as a between-subjects factor. Self-efficacy at baseline, age, and PDDS scores were entered as covariates to control for group differences. Before conducting the ANCOVA, we tested the assumptions of homoscedasticity and normally distributed errors.
To examine whether participants in the experimental group who improved in self-efficacy also reported less loneliness (as assessed by the Revised UCLA Loneliness Scale score) and depression (assessed by CMDI score) than those who did not improve their self-efficacy, we divided participants in the experimental group into two groups: improvers (n = 30; improved on both self-efficacy measures) and nonimprovers (n = 21; did not improve in either or both self-efficacy measures). Two 2 × 2 repeated-measures analyses of variance, with two groups (improvers vs. nonimprovers) as a between-subjects factor and time of testing as a within-subjects factor, were conducted.
Power Analysis
Prior intervention studies that had improved health outcomes had an effect size for self-efficacy of about .30 (Jerant et al., 2008). A sample size of 90 participants was required, calculated using G*Power Version 3.1.9 (Faul et al., 2007) and using an effect size of .30 with an α of .05 and power of .80.
Results
After controlling for MSSE Scale baseline differences, participants in the experimental group reported better self-efficacy compared with the control group, F(1, 87) = 17.5, p < .001; η2 = .25. This finding suggests that the increase in self-efficacy score from pretest to posttest in the experimental group was larger than in the control group after controlling for baseline differences (Figure 2A). Similar results were found with the GSES as a dependent variable. There was a significant group main effect, F(1, 87) = 9.3, p < .01, η2 = .15, indicating larger pretest to posttest change in the experimental group than in the control group (Figure 2B).
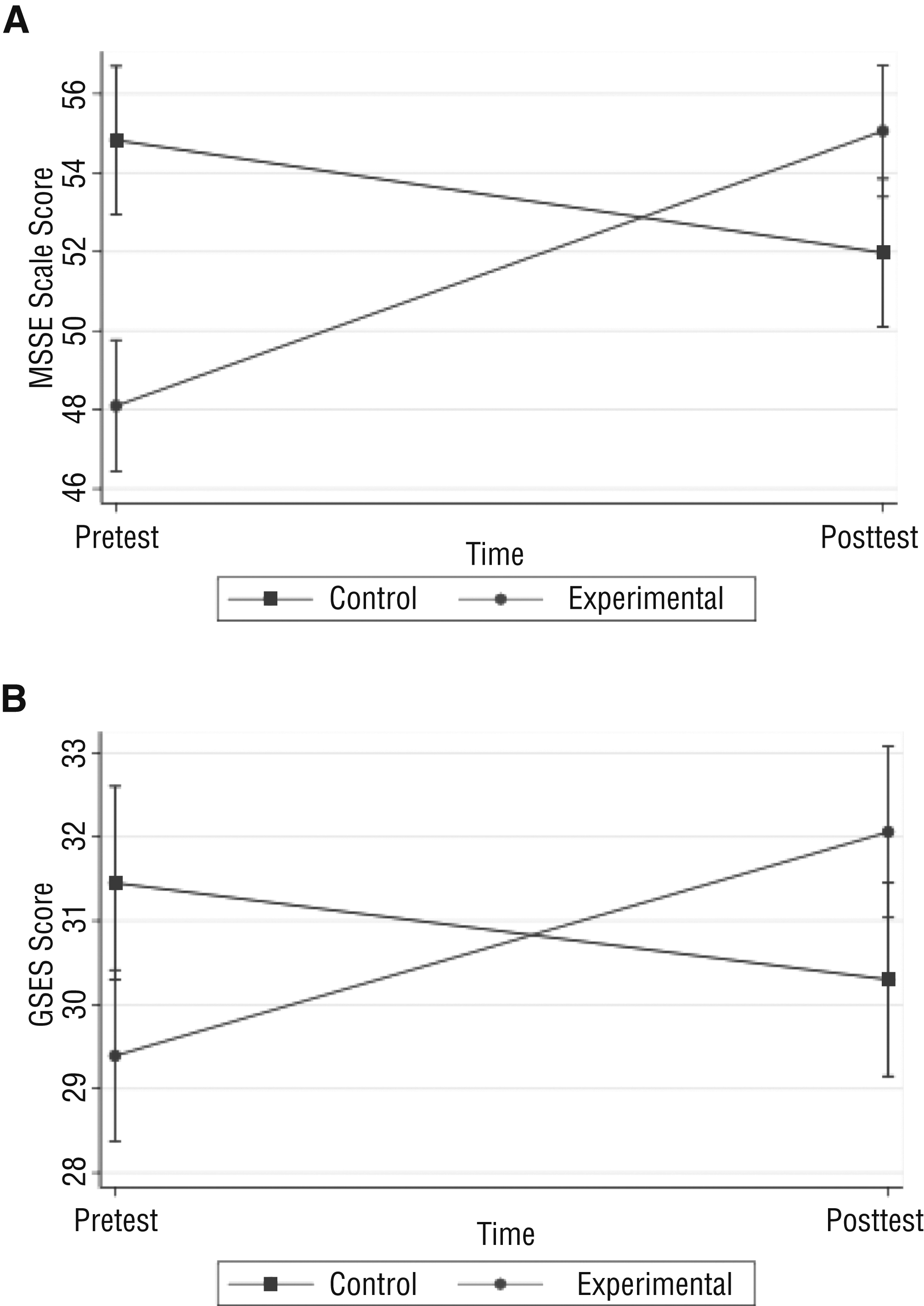
(A) MSSE Scale and (B) GSES mean scores and confidence intervals (shown with bars) before and after treatment for the experimental and control groups.
A significant interaction was observed between time and group in relation to loneliness, F(1, 49) = 11.01, p < .002. Thus, the decrease in loneliness from pretest to posttest was significantly larger among participants who demonstrated an improvement in self-efficacy (mean pretest [M pre] = 45.80, standard deviation pretest [SD pre] = 10.04; mean posttest [M post] = 37.97, standard deviation posttest [SD post] = 11.04) than among those who did not improve in self-efficacy (M pre = 42.29, SD pre = 11.60; M post = 39.67, SD post = 10.08; Figure 3).
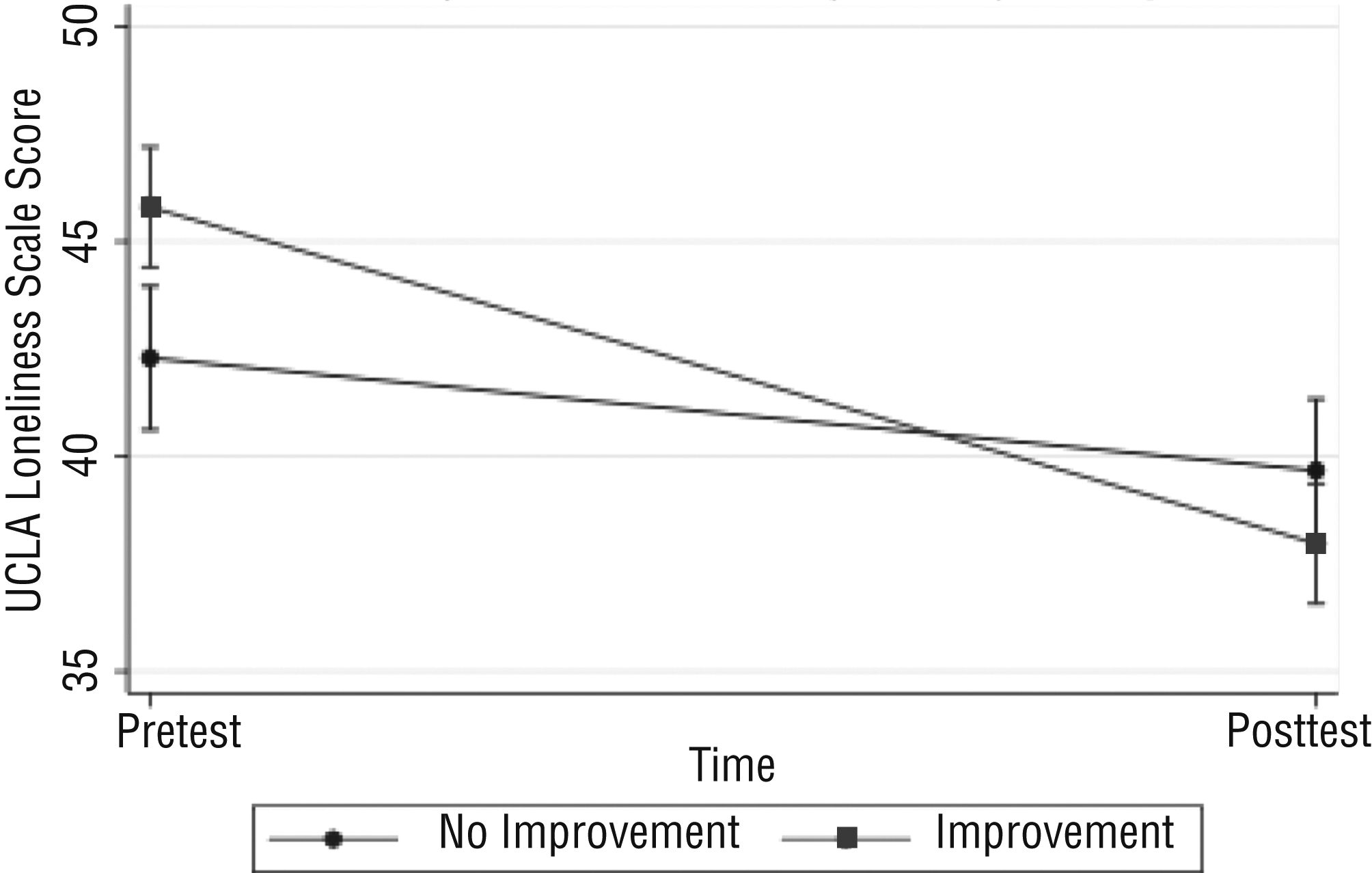
Revised UCLA Loneliness Scale mean scores and confidence intervals (shown with bars) for experimental group participants (improvers and nonimprovers).
The difference between pretest and posttest in relation to depressive symptoms among participants who improved in self-efficacy (M pre = 4.54, SD pre = 0.34; M post = 4.43, SD post = 0.38) did not differ from the nonimprovers (M pre = 4.50, SD pre = 0.38; M post = 4.40, SD post = 0.36) as indicated by the insignificant interaction, F(1, 49) = 0.04, p = .84.
Discussion
Participants who received the CRISP intervention demonstrated a statistically significant improvement in both general and MS-specific self-efficacy. CRISP, a social performance–based intervention, is intended to improve self-efficacy to help mitigate common MS symptoms, specifically difficulty with social outings. This study finding indicates that increasing the repertoire of self-management strategies and having the opportunity to experience the use of such strategies during social activities may be an important component in improving self-efficacy. This finding was also reported by Rigby and colleagues (2008).
This current study examined whether participants with MS who experienced improved self-efficacy would report lower levels of loneliness. Because there was a significant reduction in loneliness in those with improved self-efficacy, improved self-efficacy may be an important component of changing a person’s perception about feeling lonely. Improved self-efficacy can help people reevaluate and perceive their current social situation and relationships in a different way, and it can motivate people to overcome challenges that have prevented them from socializing. This finding is of particular importance because loneliness among people with MS and its consequences have been neglected in the literature to date.
Participants who improved in self-efficacy did not significantly differ from nonimprovers in depressive symptoms after treatment. This finding was surprising, because previous studies have demonstrated that people with MS who reported low levels of self-efficacy also experienced increased levels of depression (Amtmann et al., 2012; Garfield & Lincoln, 2012; Schmitt et al., 2014; Shnek et al., 1997; Tan-Kristanto & Kiropoulos, 2015). Others studies, however, have concluded that self-efficacy may not always be associated with depression in people with MS (Motl, McAuley, Wynn, et al., 2013; Rigby et al., 2008). The findings of this study suggest that self-efficacy and depression are not related. MS is a multifaceted disease that can convolute a direct association between self-efficacy and depression because depression can be influenced by various MS symptoms and can also be a primary symptom directly related to lesions (Arnett et al., 2008). Therefore, the relationship between self-efficacy and depression may be complex and requires further clarification.
Study Limitations
This study did not control for the social interactions of participants in the control group during the duration of the study. In addition, the CRISP interventions occurred during working hours (9 a.m. to 5 p.m.), which made participation difficult for people who were employed. Study participants, therefore, consisted of a largely unemployed sample. However, this intervention program can still be generalized to the MS population because the unemployment rate of the study sample (90%) is representative of the unemployment rate of people with MS (80%; Kornblith et al., 1986). Finally, twice as many participants dropped out of the control group as the intervention group. This dropout rate may have increased the difference in the posttest findings.
Future Research
Future research should determine whether the effects of the CRISP intervention program are maintained over extended periods of time. In addition, it would be helpful to determine the ideal number of total group sessions and the number of social and educational groups that can produce comparable findings. Treatment efficacy could be assessed using other outcome measures, such as quality of life, community integration, social participation, and self-esteem outcomes.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
The CRISP intervention has the potential to be a useful program for occupational therapy practitioners to address self-efficacy through engagement in occupations related to socialization.
Self-efficacy may be associated with decreased loneliness, one of the many MS symptoms that can affect quality of life.
Conclusion
This study supports that an educational and performance-based socialization program can improve self-efficacy among people with MS and that improved self-efficacy is associated with reduced feelings of loneliness. CRISP, an innovative socialization program, results in positive outcomes for people with MS and can help them regain control over some of their symptoms.