
Abstract
The main purpose of this study was to estimate the minimal detectable change (MDC) on the Lawton Instrumental Activities of Daily Living (LIADL) scale in community-dwelling patients with schizophrenia. Fifty-seven patients completed the LIADL assessment twice, about 14 days apart. Two scoring methods (dichotomous and polytomous) were used to record the patients’ performance on the LIADL scale. The MDCs of the LIADL scale were 1.5 (dichotomous) and 4.4 (polytomous) points. The MDC percentages were 22.0% (dichotomous) and 22.5% (polytomous), both of which are within acceptable measurement errors. The test–retest reliabilities of the LIADL scale were both acceptable with two different scoring methods (dichotomous = .75; polytomous = .76). Users can choose the scoring method according to their individual needs.
Schizophrenia is characterized by delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, and negative symptoms (i.e., diminished emotional expression or avolition; American Psychiatric Association, 2013). These symptoms affect patients’ self-care, independent living, work, school, and leisure (Mueser & McGurk, 2004). More than half of patients with schizophrenia have problems with instrumental activities of daily living (IADLs) and need assistance (Bowie et al., 2006; Mausbach et al., 2008; Twamley et al., 2002).
In addition, poor IADL function leads to disability in these patients (Das et al., 2012; Godbout et al., 2007; Hsieh et al., 2011). Thus, independent living and the related performance of daily activities have been identified as treatment outcome priorities by people with schizophrenia (Fischer et al., 2002). To manage and monitor daily activity function in these patients, clinicians need to routinely measure their performance of activities of daily living (ADLs) and IADLs.
The Lawton Instrumental Activities of Daily Living (LIADL) scale (Graf, 2008; Lawton & Brody, 1969) was developed to assess complicated ADL functions necessary for independent living. It contains eight items and can be administered through an interview or by means of a written questionnaire. Several scoring methods (e.g., dichotomous, trichotomous, and polytomous) have been developed for different purposes (e.g., rapidity, ease, or comprehensiveness) in previous studies (Boyle et al., 2003; Cromwell et al., 2003; Lawton & Brody, 1969; Vittengl et al., 2006).
The LIADL scale has been translated into several languages and is now widely used to assess living skills in older adults and community residents who are cognitively impaired (Jekel et al., 2015; Vergara et al., 2012). It has also been used to assess IADL function in people with schizophrenia (Brodaty et al., 2003; Doroud et al., 2011; Roldán-Merino et al., 2013; Wu et al., 2013).
The minimal detectable change (MDC) represents the smallest threshold to determine whether a change score of an individual patient between successive measurements is beyond or within random measurement error at a certain confidence level (usually 95%; Haley & Fragala-Pinkham, 2006)—that is, a change score between repeated assessments lower than the MDC can be attributed to random error (Schreuders et al., 2003). Clinicians and researchers can use the MDC of a measure as a threshold to determine whether a change score between repeated assessments of an individual patient represents a true change or is within the bounds of random error (Haley & Fragala-Pinkham, 2006). Therefore, the MDC is crucial for users in interpreting the results of assessment in research and clinical settings (Haley & Fragala-Pinkham, 2006; Jette et al., 2007).
The LIADL scale is a reliable measure for older adults and patients with dementia (Hassani Mehraban et al., 2014; Olazarán et al., 2005; Tong & Man, 2002; Vergara et al., 2012). However, to our knowledge, the reliability and MDC of the LIADL scale in patients with schizophrenia are unknown, limiting the utility of the measure. Thus, the purpose of this study was to estimate the MDC and the test–retest reliability of the LIADL scale in community-dwelling patients with schizophrenia.
Method
Patients
All patients were recruited from two community psychiatric rehabilitation centers of a medical hospital in northern Taiwan. The patients were included in this study if they met the following criteria: diagnosis of schizophrenia or schizoaffective disorder according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; American Psychiatric Association, 2000), age ≥20 yr, stable dose of antipsychotic medication for at least 1 mo, and Mini-Mental State Examination (MMSE; Folstein et al., 1975) score ≥21.
Exclusion criteria consisted of diagnosis of a neurological condition affecting cognition (e.g., stroke, depression) or of a severe medical condition or psychiatric disorder requiring treatment during the study. In addition, if the Clinical Global Impressions–Severity scale (CGI–S; Guy, 1976) scores of the patient changed between the first and second assessment sessions, the patient’s data were excluded.
This study was approved by the institutional review board of the medical hospital. All patients signed consent forms before participating in this study.
Procedure
All patients were interviewed by one rater in two sessions, about 2 wk apart. The rater was a trained research assistant who was also a licensed occupational therapist familiar with the LIADL assessment protocol. The CGI–S was assessed by the patient’s main occupational therapist working in the center. In addition, we also collected the patients’ demographic and clinical characteristics from chart review.
Measures
Lawton Instrumental Activities of Daily Living Scale.
The LIADL scale was developed by Lawton and Brody (1969) to assess the more complex ADLs necessary for living in the community (Graf, 2008). The LIADL scale contains eight items required for independent living: using the telephone, shopping, preparing food, housekeeping, doing laundry, traveling away from home, taking medications properly, and handling personal finances. The scale was assessed by interview in this study and took about 10–15 min to administer. The items of the LIADL scale are common daily activities for patients with schizophrenia living in the community.
We adopted the method of previous studies (Cromwell et al., 2003; Graf, 2008; Roldán-Merino et al., 2013), in which all items were assessed and scored regardless of gender. Several scoring methods (e.g., dichotomous, trichotomous, and polytomous methods) have been used in the past (Boyle et al., 2003; Cromwell et al., 2003; Lawton & Brody, 1969; Vittengl et al., 2006). To examine the test–retest reliability and MDC of the simple (i.e., dichotomous) and comprehensive (i.e., polytomous) methods, we adopted the dichotomous (0 = less able, 1 = more able) and polytomous (including 0–2, 0–3, and 0–4 scoring) methods.
The total scores of the dichotomous method range from 0 to 8, and those of the polytomous from 0 to 23. The dichotomous scoring method can be easy and time saving for users. The polytomous scoring method can help users realize the level of function and detect subtle changes on each item. A greater score indicates a higher level of independence (Cromwell et al., 2003; Graf, 2008; Kuchibhatla & Fillenbaum, 2003; Vittengl et al., 2006).
Mini-Mental State Examination.
The MMSE (Folstein et al., 1975) was used to measure cognitive functioning, including orientation, attention, and memory. It has 11 tasks and is administered by interview. Test scores are summed (from 0 to 30 points), and higher scores indicate better cognitive functioning (Vertesi et al., 2001).
Data Analysis
Data were analyzed with IBM SPSS Statistics (Version 15; IBM Corp., Armonk, NY). The MDC (at the 95% confidence level) was calculated on the basis of the standard error of measurement (SEM) as follows (Haley & Fragala-Pinkham, 2006):


In the first formula, the multiplier of 
The ICC was calculated by a random-effects, two-way analysis of variance. An ICC value ≥.80 indicates high reliability, .60–.79 indicates moderate reliability, and <.59 indicates poor reliability (Bushnell et al., 2001; Prince et al., 1980). In addition, the MDC percentage (MDC%) of the LIADL scale was computed to demonstrate the relative amount of random measurement error. The MDC% was the MDC divided by the mean of all patients’ scores. An MDC% <30 was considered acceptable, and <10 was considered excellent (Smidt et al., 2002).
The reproducibility between two repeated assessments can be presented by Bland–Altman plots with 95% limits of agreement (LOA; Bland & Altman, 1986). In the plots, the differences (đ) between each pair of assessments were plotted against the mean of each pair of assessments. In general, 95% of the differences lie between đ ± 1.96 × SD (i.e., LOA). In ideal conditions, there should be no systematic bias in a Bland–Altman plot. Systematic bias was examined by means of a paired t test.
Results
Seventy-four patients with schizophrenia participated in this study and completed the first assessment. Of the 74 patients, 14 patients were excluded because their CGI–S scores changed between the first and second assessment sessions; another 3 patients were lost to follow-up because of refusal to retest. Demographic and clinical features of the 57 patients are shown in Table 1.
Patients’ Demographic and Clinical Features
Note. LIADL = Lawton Instrumental Activities of Daily Living; M = mean; Mdn = median; SD = standard deviation.
There were only two valid numbers; median could not be calculated.
The mean age was 42.4 yr, and 29.8% of the patients were men. The median time of evolution of schizophrenia was 19.0 yr. The mean baseline scores on the LIADL scale were 7.0 (dichotomous) and 20.7 (polytomous) points, respectively; t tests showed that there were no significant differences in mean baseline scores on the LIADL scale between those who completed both sessions of testing and those who did not (p = .27 [dichotomous]; p = .35 [polytomous]; see Table 1).
The test–retest reliability indices of the LIADL scale are shown in Table 2. The mean differences for the LIADL scale were 0.00 (dichotomous) and 0.18 (polytomous), respectively. The MDCs of the LIADL scale were 1.5 (dichotomous) and 4.4 (polytomous) points. The MDC%s were 22.0 (dichotomous) and 22.5 (polytomous), representing acceptable measurement errors. The ICCs for the LIADL scale were .75 (dichotomous) and .76 (polytomous), indicating acceptable test–retest reproducibility.
Test–Retest Reliability Indices of the LIADL Scale (n = 57)
Note. Total score range of the dichotomous method = 0–8 points. Total score range of the polytomous method = 0–23 points. CI = confidence interval; ICC = intraclass correlation coefficient; LIADL = Lawton Instrumental Activities of Daily Living; M = mean; MDC = minimal detectable change (= 1.96 × 
In Figure 1, the differences in the scores are plotted against the mean scores of the two measurements of the LIADL scale. The LOAs ranged from 1.57 to −1.57 points for the dichotomous scoring method and from 4.66 to −4.31 points for the polytomous scoring method.
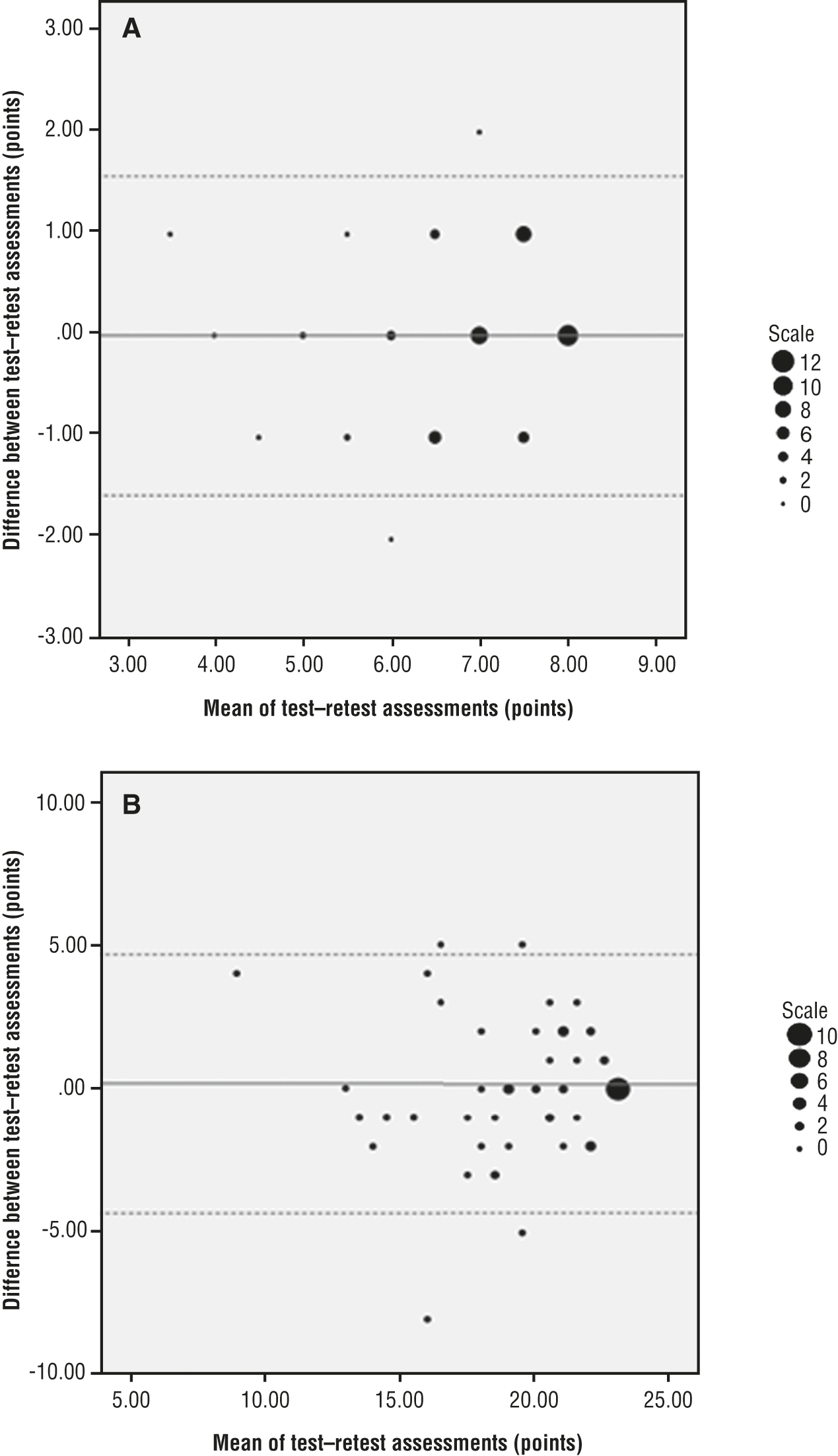
Bland–Altman plots showing the difference scores against the mean scores of each pair of scores on the Lawton Instrumental Activities of Daily Living (LIADL) scale with dichotomous (A) and polytomous (B) scoring methods (n = 57).
Discussion
IADL function has been identified as one of the major treatment outcomes for community-dwelling patients with schizophrenia (Fischer et al., 2002). Although the LIADL scale is commonly used for patients with schizophrenia (Brodaty et al., 2003; Doroud et al., 2011; Roldán-Merino et al., 2013; Wu et al., 2013), the MDC has not been explored. In this study, we provided the MDC and test–retest reliability data of the LIADL scale. The results of this study can help clinicians and researchers determine the true change between successive LIADL assessments for community-dwelling patients with schizophrenia.
We used two scoring methods in this study to estimate the ICC and MDC of the LIADL scale. The ICCs for the LIADL scale were .75 (dichotomous method) and .76 (polytomous method), respectively, indicating moderate and similar test–retest reliability. These similar results may be due to the two scoring methods simultaneously applied in our study. The MDC of the LIADL scale was 1.5 points when the dichotomous scoring method was used. This result indicates that a change of at least 2 points between two consecutive assessments can be interpreted as a true improvement with 95% certainty. Moreover, the MDC of the LIADL scale was 4.4 points when the polytomous scoring method was used.
This finding indicates that only a change of ≥5 points between two consecutive assessments can be interpreted as a true improvement with 95% certainty. The dichotomous method makes assessments and calculation of the scores easy and fast. However, this method may not be useful for treatment planning or showing detailed changes because the scaling is rough. Although the polytomous method is time consuming, the increased scaling can help clinicians to detect subtle changes in patients and thereby develop further treatment plans accordingly. Given the prerequisite similar test–retest reproducibility, we suggest that the dichotomous scoring method be used for research purposes and the polytomous scoring method be used for clinical evaluations.
However, it may not be easy for a patient to have a change score beyond the MDC of the LIADL scale (i.e., 2 points for the 8-point scale or 5 points for the 23-point scale). Such a substantial amount of MDC also shows the importance of our findings. The MDC of the LIADL scale is critical for users in confirming whether the change score exceeds the measurement error for a single person with schizophrenia. In addition, reducing the measurement error of the LIADL scale might be an issue to be addressed in the future.
Both MDC%s were <30 (22.0 for the dichotomous method and 22.5 for the polytomous method), indicating that the relative measurement errors for these two scoring methods are acceptable. In other words, no matter which scoring method was used, the MDC%s were similar.
The test–retest reliability of the LIADL scale has been shown to be high for older adults (ICC = .93; Lawton & Brody, 1969) and patients with dementia (ICC = .99; Hassani Mehraban et al., 2014). In our study, however, the test–retest reliability was only moderate (ICC = .75) for the community-dwelling patients with schizophrenia. Our patients’ scores were relatively high, but the variation was low, which may have been an important factor in the lower ICC. Although the test–retest reliability in this study was only at the moderate level, the result can be used as an evaluation reference of the LIADL scale for patients with schizophrenia living in the community.
From the Bland–Altman plots (see Figure 1), we found that most of the patients’ LIADL scale scores were in the higher partition. In the beginning, 16 patients (28%; dichotomous method) and 13 patients (23%; polytomous method), respectively, were even at the highest score, affecting the progress and distribution of patients’ scores in these figures. That is, our results indicate that the LIADL scale may have a ceiling effect in community-dwelling patients with schizophrenia.
Limitations
This study had some limitations. First, our patients were community-dwelling patients with schizophrenia. Their IADL needs and performances might be different from those of patients in other situations; therefore, our findings may not be generalizable to inpatients with schizophrenia. Second, the rater in this study was an occupational therapist. The assessment results might be different from those obtained by other medical professionals or other therapists. Future studies might need to examine the interdiscipline and interoccupational therapist reliabilities of the LIADL scale. Third, because of the high IADL function of the numerous patients in this study, the results of reliability may have been overestimated. Fourth, to our knowledge, the validity of the LIADL scale has not been examined in people with schizophrenia.
Further studies to investigate the validity of the LIADL scale in this population are needed. Finally, we excluded patients with inconsistent CGI–S scores during the study. These features of the sample might influence the generalizability of our results. Future studies should recruit patients with various situations and levels of IADL function to further validate our findings.
Implications for Occupational Therapy Practice and Research
The results of this study have the following implications for occupational therapy practice and research:
IADL function is an important indicator of the quality of life in patients with schizophrenia. In this study, we provided the MDC and test–retest reliability data of the LIADL scale. The results of this study can help clinicians and researchers determine the true change between successive LIADL assessments for a single community-dwelling patient with schizophrenia.
Two scoring methods were used in this study. The dichotomous scoring method is easy and time saving for users. The polytomous scoring method can help users quantify the level of function for each task and item. Both scoring methods were shown to have similar test–retest reliability and MDC. Thus, considering time and necessity, users can choose the dichotomous or the polytomous scoring method according to their needs.
Conclusion
The test–retest reliability of the LIADL scale was acceptable, and the MDC was estimated in people with schizophrenia living in the community. The test–retest reliabilities and measurement errors of the two scoring methods were similar and acceptable. Users can choose the scoring methods according to their individual needs.
Footnotes
Acknowledgments
Shu-Chun Lee and Ching-Lin Hsieh contributed equally to this work. We thank all the patients who contributed to this study. This study was supported by a research grant from the Taipei City Hospital (TPCH-104-057), Taiwan.