
Abstract
The mobility and stability of the wrist joint are essential for daily function. Wrist injuries usually hinder independence and functionality by affecting the ability to perform basic activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Vergara et al., 2016). Wrist injuries constitute 15.2% of upper extremity injuries, among which wrist fractures are common (40.6%) and greatly affect joint mobility (Moritomo, 2010).
One of the main goals of therapy after wrist fracture is regaining mobilization through orthogonal anatomical planes, that is, flexion–extension (FE) and radial–ulnar deviation (RUD). Distal and proximal adjacent joints (i.e., fingers and elbow) are also exercised by means of maneuvers of finger and elbow FE as well as prosupination. Static, progressive, and dynamic orthoses for slow, prolonged stretching can be an integral part of the rehabilitation process and are used to increase the passive range of motion (ROM).
Normal active wrist ROM is approximately 80° flexion to 70° extension and 20° radial deviation to 30° ulnar deviation (Safaee-Rad et al., 1990). The functional ROM is 5° flexion to 30° extension and 5° radial deviation to 10° ulnar deviation (Ryu et al., 1991). Occupational therapy intervention aims to facilitate functional ROM by the end of the rehabilitation. Accordingly, rehabilitation after a wrist fracture can include exercising FE movements using a dynamic orthosis.
Typical wrist movements occur in both planes simultaneously. One important combined motion involves movement of the wrist along a path from radial extension to ulnar flexion, named the dart-throwing motion (DTM) plane (Moritomo et al., 2007). Anatomically, the axis of the DTM plane passes obliquely from the radio-palmar aspect of the scaphoid tuberosity to the ulnodorsal aspect of the hamate (Moritomo et al., 2006). An overview of ape carpal morphology suggested that morphologic adaptations in the carpal bones enabled the development of a dart thrower’s arc of wrist motion in humans (Wolfe et al., 2006). Several studies have shown minimal scaphoid and lunate motion throughout the dart thrower’s arc, which allows for an effective grip and manipulation of tools (Rohde et al., 2010; Wolfe et al., 2006).
Most functional activities in the dominant hand occur at a DTM plane angle of approximately 30°–45° from the sagittal plane (Moritomo et al., 2007). The differences in DTM plane angle result from the monitored task, intersubject variability, and intertask variability. Intersubject variability may result from anatomic differences or other physiological factors (Moritomo et al., 2007). Mobilization through the DTM plane may be considered a more stable and controlled movement because most motion occurs at the midcarpal joint, and the proximal carpal row of bones remains relatively stable (Garcia-Elias et al., 2014). This stable condition might prove advantageous in rehabilitation after wrist fracture when the ligaments are intact (Garcia-Elias et al., 2014; Rainbow et al., 2016), as well as after wrist fracture in which the tissues around the proximal carpal row are repaired, because these tissues might not be disturbed during early DTM (Braidotti et al., 2015).
Because the DTM is the most natural wrist motion in humans (i.e., the most frequently used during daily activities), wrist rehabilitation with or without an orthotic device restricting the movement of the wrist to the DTM plane has been hypothesized to enhance wrist rehabilitation (Moritomo et al., 2007). Accordingly, several attempts have been made to devise a DTM orthosis that restricts wrist movement to the DTM arc (Anderson & Hoy, 2016; Braidotti et al., 2015; Feehan & Fraser, 2016). However, all existing data regarding wrist kinematics in the DTM plane were recorded on the wrist of the dominant arm. Thus, the relevance of the aforementioned hypothesis to an injured wrist on the nondominant arm has not been addressed. This may be a concern because differences are known to exist between different parameters of the dominant and nondominant upper extremities (Sainburg, 2005). For example, right-handed people exhibited dominant-hand superiority in grip strength and manual dexterity, whereas left-handed people showed no differences (Özcan et al., 2004). Moreover, there was a general trend for faster object manipulation using the dominant hand (Cary & Adams, 2003).
Taking into consideration the differences between dominant and nondominant hand function, we expected to observe dissimilarity in the DTM angle between hands during daily functions and therefore a difference between dominant and nondominant wrist engagement in the DTM. To the best of our knowledge, no studies have compared wrist ROM and DTM plane angles during ADLs between the dominant and nondominant hands. This knowledge may affect the understanding of wrist motion biomechanics during daily life. More important, it might provide an answer as to whether training in the DTM during rehabilitation is beneficial after wrist injury to either the dominant or the nondominant hand. We therefore aimed to quantify and compare wrist ROM and DTM plane angles in both hands during common ADLs. Concluding whether similarity exists between wrist ROM and DTM plane angles between both hands in daily living conditions can only be determined with a healthy population whose wrist movements are not confined because of pain or anatomical limitations. We therefore conducted our study with healthy participants.
Method
Participants
The participants were 43 healthy adults (30 women, 13 men; mean age = 32 yr, standard deviation = 13, range = 20–64). The inclusion criterion was right-hand dominance. We chose to enroll only right-handed people because they are the majority and therefore represent most of the population. Also, left-handed people show higher similarity in hand function between hands so they could bias the results. Exclusion criteria were orthopedic or neurological impairment of the upper extremity. The study was approved by the Tel Aviv University ethics committee (Tel Aviv, Israel). Participants were recruited by convenience and snowball sampling methods.
Research Tools
A telemetric twin-axis electrogoniometer (SG65; Biometrics Ltd., Newport, England; Bashardoust Tajali et al., 2016; da Silva Camassuti et al., 2015; Rawes et al., 1996; Figure 1) was used to measure the wrist movement angles in both sagittal and coronal planes. The specifications of this goniometer have previously been examined and validated (Ojima et al., 1991), and the system was found to be highly reliable and accurate (Rawes et al., 1996). The electrogoniometer was calibrated using 7-point calibration with a manual goniometer on a flat surface for both planes (angles of 0°, ±30°, ±45°, ±90°), and a voltage to angle linear curve was produced. These data were used to calculate the angle of the DTM plane (Figure 1B). The use of electrogoniometers for clinical and research studies has been common in the past 2 decades. Various studies have shown high accuracy and reliability of measurements, including measurement of wrist angles (Bandy & Reese, 2009; Ojima et al., 1991; Rawes et al., 1996; Rowe et al., 2001). Also, a 1° increment manual goniometer was used for static measurement of the ROM of the wrist (Carter et al., 2009).
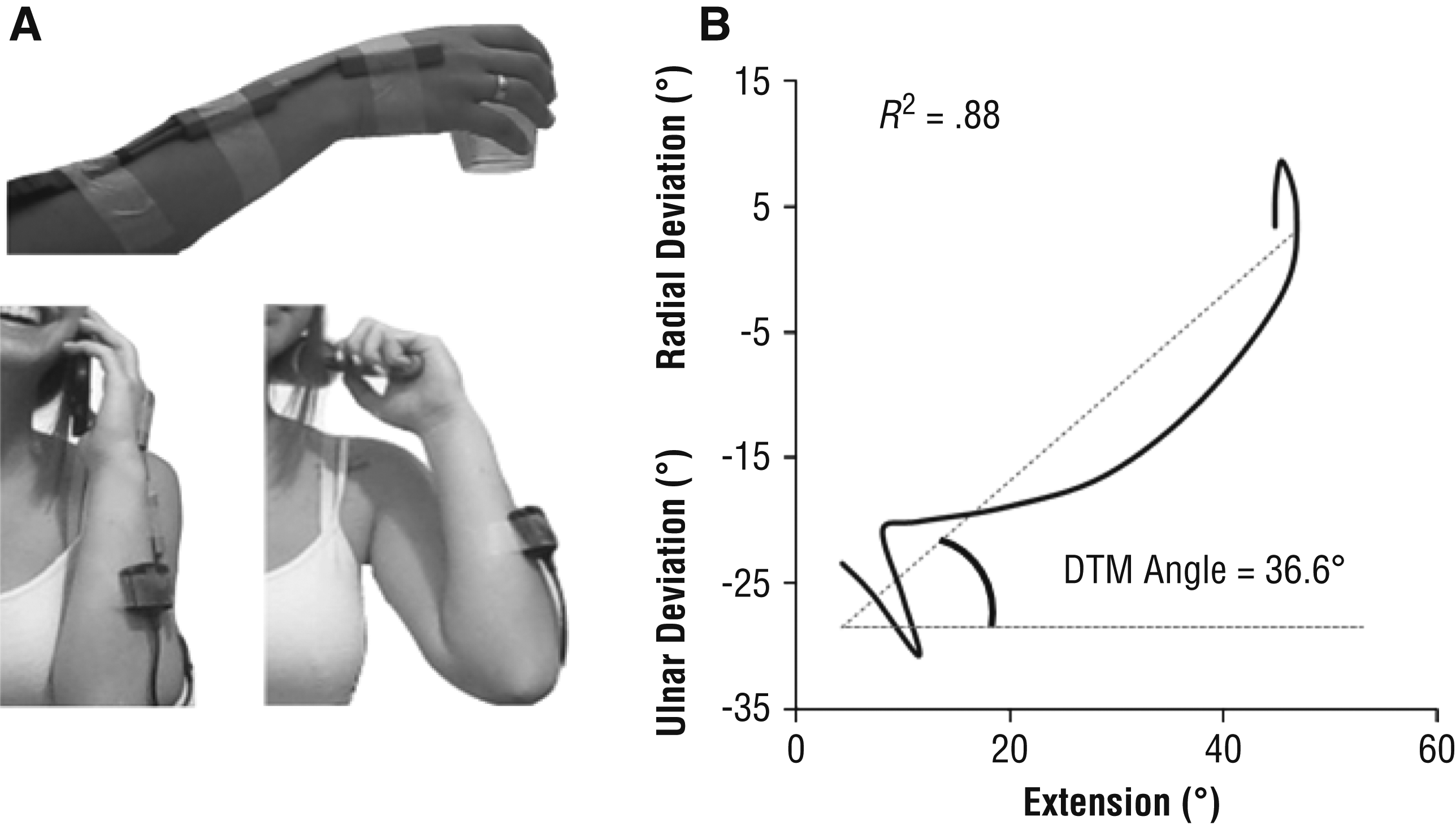
A telemetric twin-axis electrogoniometer was used to measure the wrist movement angles in both sagittal and coronal planes.
Protocol
Each participant read and signed an informed consent form before the trial. First, the active ROM of the wrists was measured using a manual goniometer. Second, an electrogoniometer was attached using medical tape, placed so that it would least impede motion (Figure 1A). The proximal attachment of the electrogoniometer was placed along the long axis of the dorsal aspect of the arm, and the distal end was attached above the third metacarpal bone.
Each participant performed a series of nine ADL tasks while sitting at a table, once when the electrogoniometer was placed on the dominant hand and once when it was placed on the nondominant hand. The chair and seat were adjusted according to the height of the participant, so that the participant’s feet rested comfortably on the floor. The sequence of the trials was counterbalanced so that 22 participants began the trials with the electrogoniometer attached to their dominant hand and 21 participants began the trials with the electrogoniometer attached to their nondominant hand. The participants were instructed to perform six frequent unilateral tasks. Some of the tasks chosen had previously been investigated for the dominant wrist (Garg et al., 2014), and other tasks were chosen because they were frequent movements that are important with respect to a patient’s level of independence after a wrist injury: Hammer a 6.4-cm-long nail into a 25-cm-long wooden board, pour water from a 750-ml plastic bottle into a disposable plastic cup, drink from a plastic cup (see Figure 1A), throw a ball toward a 22-cm-diameter bucket set 1 m away at a height of 1.5 m, use a comb (a plastic roller replaced a real comb; see Figure 1A), and answer a cellphone (see Figure 1A). In addition, the participants were asked to perform three bimanual tasks: first open and then close a 7-cm-diameter glass jar and wring a dry floor cloth.
As noted, each of the nine tasks was performed twice, once when the electrogoniometer was placed on the dominant hand and once when it was placed on the nondominant hand. Some of the unilateral tasks are seldom performed with the nondominant hand (e.g., using a hammer), but some of them may be performed during daily life with either hand (e.g., drinking from a cup). We chose to include the hammering task because it is often identified with studies of DTM. In each of these tasks, the object was placed in a marked position in front of the participant. Simple instructions were provided (e.g., “drink from the cup,” “answer the phone,” “open the jar”) so that the manipulation of the object would be similar to that in everyday situations.
Analysis
Data recorded by the electrogoniometer were analyzed using a code written in Labview software (Version 12; National Instruments, Austin, TX). For each of the nine tasks, we calculated the ROM in each plane for the dominant and nondominant hand. The DTM plane angle was also calculated as the angle between the best linear fit for scatter of FE versus RUD angles recorded by the electrogoniometer during each task and the axis of the FE (Figure 1B). Negative values represent the motion plane for ulnar extension with radial flexion. Statistical analyses were performed in IBM SPSS Statistics (Version 21; IBM Corp., Armonk, NY).
Bland–Altman plots were produced separately for each of the nine tasks to compare the DTM plane angles of the dominant and nondominant hands. Normality of the distributions was assessed using the Shapiro–Wilk test (Shapiro & Wilk, 1965). Most values were not normally distributed, so Wilcoxon matched pairs tests were performed. Bonferroni correction was used to counteract the effect of multiple trials (nine tasks), so the adjusted p for significance was <.0056. Moreover, because the static ulnar deviation range differed between the dominant and nondominant hands, we evaluated the relationship between static ulnar ROM and DTM plane angles. For this purpose, we calculated Spearman’s rank order correlation coefficients between the static ulnar ROM of each hand and the DTM plane angle calculated in each task for the specific hand. We used a 95% bias-corrected bootstrap (based on 1,000 bootstrap samples).
Results
We found no statistical differences between the DTM plane angles of the group who began with the electrogoniometer attached to their dominant hand and the group who began with it attached to their nondominant hand, implying that there was no learning effect during the trials.
Descriptive data for wrist ROM, DTM plane angles, and R 2 of the fitted DTM line measured for the nine ADL tasks for both hands are presented in Tables 1 and 2, respectively. No significant differences were found between the DTM plane angles of both hands in all tasks (see Table 2). Bland–Altman plots show some agreement between the measurements of the DTM plane angles between the dominant and nondominant hands, especially in the unilateral tasks (Figure 2).
Median and IQR of Static Wrist ROM and Dynamic ROM While Performing Different Tasks (N = 43)
Note.
Measured with a manual goniometer.
p < .0056.
Median and IQR of the DTM Plane Angle While Performing Different Tasks and R 2 Values of DTM Plane Angles for the Dominant and Nondominant Hands (N = 43)
Note.
p < .0056
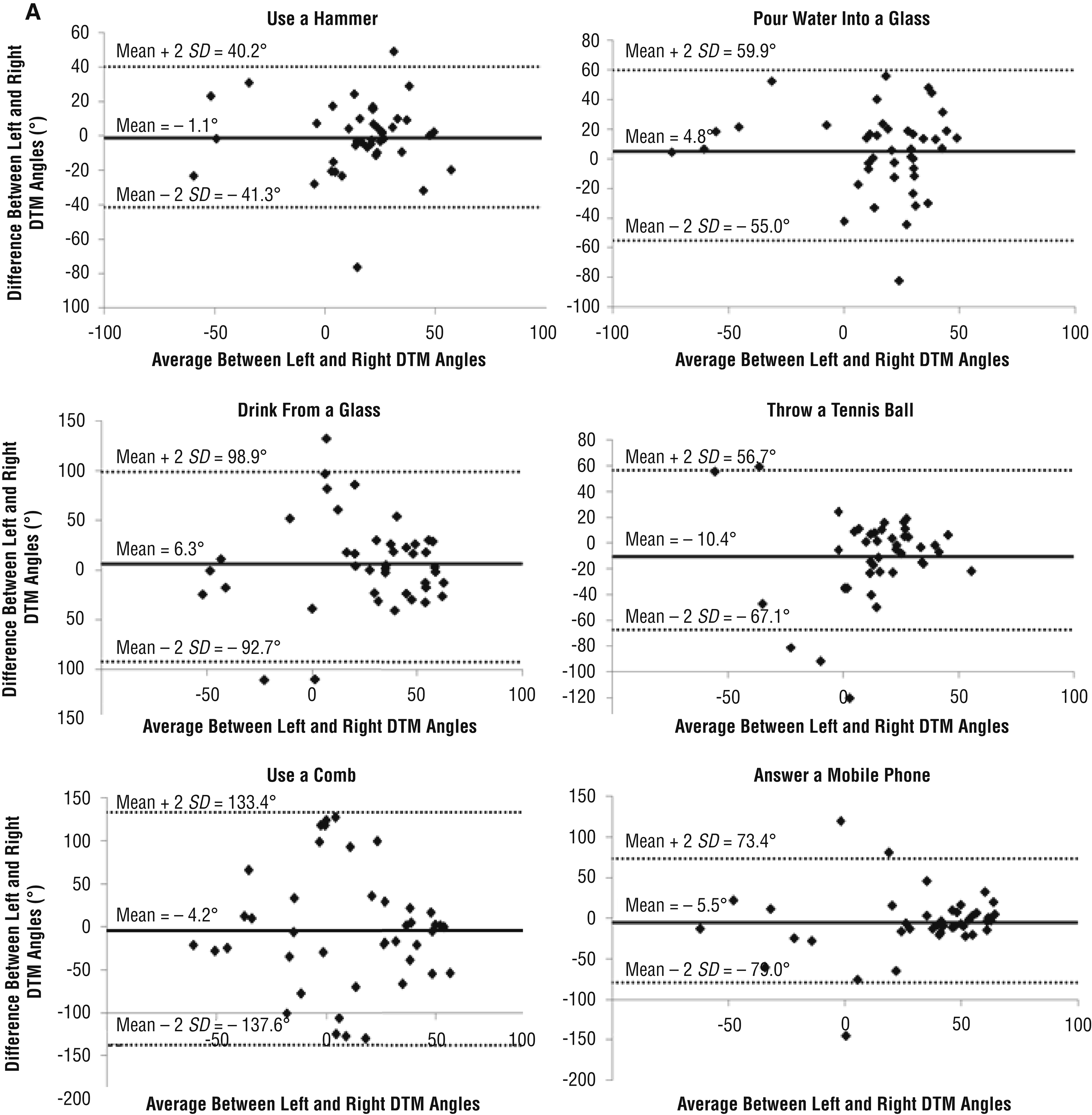
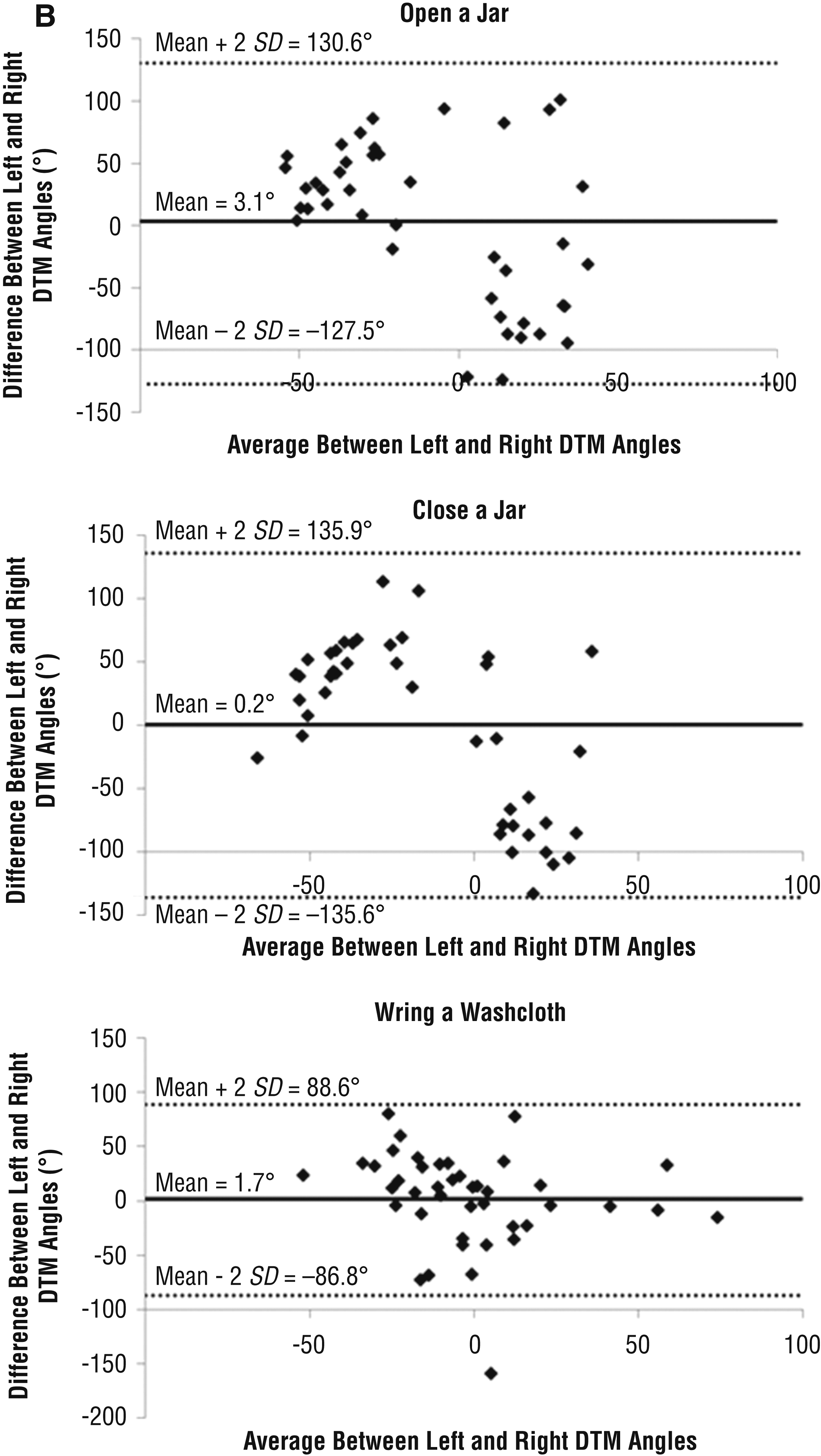
Bland–Altman plots for each of the nine tasks, (A) unilateral and (B) bilateral, comparing the DTM plane angles of the dominant and nondominant hands.
We found no significant differences between the static ROM of the two wrists, except for a greater ulnar deviation ROM in the nondominant hand. For the nondominant hand, no correlations were found between the static ulnar deviation ROM and the DTM plane angles during the nine tasks. However, in the dominant hand, the static ulnar deviation ROM correlated with the DTM plane angles during two tasks: answering a phone (r = .335, p = .028) and wringing a washcloth (r = −.376, p = .013). These tasks may therefore be chosen for practice in clinical settings because they may be able to incorporate a large range of DTM plane angles.
No significant differences in dynamic wrist ROM were found during the unilateral tasks, but while participants performed bimanual tasks, the dominant hand exhibited significantly higher FE and RUD ROM than with the nondominant hand (see Table 1). Most of the unilateral daily tasks showed DTM motion, based on the R 2 measurements (see Table 2). A low R 2 implies that the motion was not restricted to the DTM plane, as seen mainly in the nondominant hand during the bimanual tasks. The most common ADLs (e.g., pouring water, drinking from a cup, and answering a mobile phone) occurred at a DTM plane angle of approximately 20°–45°. These were the only tasks among the nine chosen ADLs that most participants performed with a positive DTM plane angle. An interesting finding was that, in several tasks (e.g., while using a comb and during the bimanual tasks), the DTM plane angle was negative (radial flexion to ulnar extension).
Discussion
In this study, we quantified and compared wrist ROM and DTM plane angles between the dominant and nondominant hands while participants performed different daily tasks. This study is the first to compare the kinematics of the dominant and nondominant wrists during the performance of such tasks. We found no statistically significant differences between the DTM plane angles for both hands while participants performed different ADLs. However, participants showed little agreement in the DTM plane angles between both hands in all tasks, highlighting the heterogeneity of the choice of DTM planes across participants and hands.
The dissimilarity between both wrist movements found here might be explained by compensation from proximal joints (i.e., the elbow and shoulder). As previous studies have demonstrated, elbow and shoulder kinematics differ between hands during reaching and throwing activities (Przybyla et al., 2012; Sachlikidis & Salter, 2007; Sainburg & Kalakanis, 2000). Moreover, previously reported differences between the hands referred to measurements of either gross motor function and grip force or finger dexterity in tasks that do not fully incorporate wrist motion. Conversely, the tasks chosen for this study included six unilateral ADLs that involve wrist movement. The kinematics of most of these daily tasks, except for answering a mobile phone, were reported in previous literature, but no data exist on the kinematics of the nondominant wrist (Brigstocke et al., 2014).
Our findings are important because each of these ADLs may be performed during dual tasking by either the dominant or the nondominant hand (e.g., answering a mobile phone with the nondominant hand while manipulating a computer mouse with the dominant hand). In addition, we chose three bimanual daily tasks for this study. The nondominant hand specializes in stabilization of an object against loads controlled by the dominant hand (Sainburg, 2005). In several tasks, the DTM plane angle was negative, mostly during the three bimanual tasks. This might be further explained by the bimanual task settings, because each hand is constrained by the other hand controlling the object (i.e., the jar or washcloth). Accordingly, the lack of absolute freedom to manipulate the object may induce movement strategy that is not the DTM.
Participants in this study used different movement strategies (high intersubject variability in the DTM plane angles). Figure 2 demonstrates that there were often great differences between hands, across tasks, and between participants. The largest intersubject variability in DTM plane angles was found in the jar manipulation task and while using a comb. This intersubject variability was also reported by Brigstocke et al. (2014). Considering this variability, a client-specific treatment plan that relies on quantitative data of the client's movement pattern might enhance the patient’s progress.
Our findings suggest that most unilateral functional movements of the wrist are performed along the DTM plane. The most common ADLs (e.g., pouring water and answering a mobile phone) occurred at a DTM plane angle of approximately 20°–45° (see Table 2). This result is similar to those of previous studies that showed that healthy participants perform most ADLs in the DTM plane with their dominant hand (Brigstocke et al., 2014; Garg et al., 2014; Rainbow et al., 2016). Reported DTM plane angles ranged from 30° to 45° in the dominant hand, as presented in the 2007 International Federation of Societies for Surgery of the Hand (IFSSH) report of the Wrist Biomechanics Committee (Moritomo et al., 2007). Other studies have reported DTM plane angles of the dominant hand ranging between 35° and 50° during ADLs (Brigstocke et al., 2014).
Another aspect of the DTM plane angle measurement is its consistency during the movement. Although Figure 1B appears to show that the wrist motion was consistent (R 2 = .88), this was not a representative pattern for some of the tasks. Participants did not maintain a constant DTM plane angle throughout the wrist motion on some tasks, as indicated by a low R 2 (see Table 2). This pattern was also recorded in a previous wrist kinematics study (Garg et al., 2014). The 2013 IFSSH Wrist Biomechanics Committee reported that “coupled” wrist motion (i.e., DTM) is an inclusive term for describing out-of-plane motion from kinematic, clinical, and rehabilitative perspectives (Moritomo et al., 2007). Several DTM planes of composite RUD and FE are likely to contribute to a variety of functional activities (Moritomo et al., 2014). This finding suggests that wrist rehabilitation should not be limited to a singular DTM plane angle but set to a wider range of angles in the vicinity of the person’s DTM plane angle or through circumduction.
In the dominant wrist, we found a low correlation between the DTM plane angle while answering a phone and the static ulnar ROM. This finding is of interest because the task of answering a phone incorporated the highest DTM plane angles among the nine chosen tasks, as seen by the large median of the DTM plane angle in Table 2. Our findings suggest that greater ulnar ROM allows the person to use a larger DTM plane angle. During the bimanual task of opening and closing a jar, the RUD and FE ROM of the dominant hand was greater than that of the nondominant hand.
These bimanual tasks emphasize the importance of the dominant hand in using the object, playing a more active role, whereas the nondominant hand functions as a less active stabilizer. Both hands reached greater FE range while wringing a washcloth than during the other tasks. The washcloth task differed from the other tasks in the high variety of movement strategies for implementation. Although a few participants used their dominant hand as a stabilizer, others used their nondominant hand, and some used both hands moving synchronically in opposite directions. For the jar manipulation tasks, the best fit found for the calculation of the DTM plane angle was significantly lower in the nondominant hand than in the dominant hand (see Table 2). This might be related to the quasi-static status of the nondominant hand during these activities, so that the wrist movement itself was negligible.
We should also note, in this context, that most of our chosen activities might be performed with very little or no wrist ROM by using proximal joints. Because the DTM has been shown here and in previous literature to be an inherent and functional movement, naturally chosen by participants to perform most ADLs, it should be firmly established in wrist training as an essential part of the rehabilitation after wrist injuries. One reason that it has not yet become a well-known part of the hand therapy protocol may be the lack of precise measurement tools for multiplane wrist motion. Using an electrogoniometer or a three-dimensional motion capture system provides an alternative, although more time-consuming and costly, method of assessing dynamic wrist kinematics. Therapists have conventionally assessed wrist ROM using reliable and valid manual goniometric measurements of FE and RUD limited to static positions (Carter et al., 2009). Recently, Bugden (2013) illustrated the difficulty of measuring the individual DTM plane angle with a standard goniometer. However, this technique was performed under static conditions.
Several limitations of this study should be considered when interpreting the results. First, taping the electrogoniometer to the hand and arm occasionally resulted in movement of the tape, so some tests were repeated after readjusting the device. Also, because only one electrogoniometer was available, the three bimanual tasks were recorded twice, so a slight difference in movement strategy when repeating the task might exist. Moreover, the study population was not heterogeneous and consisted of healthy young people. Finally, the study population was right handed, so our conclusions might not be applicable to left-handed people.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
Because there is a difference in DTM plane angle between daily tasks, wrist rehabilitation involving the DTM plane should not be limited to a singular DTM plane angle.
Because there are no significant differences between the DTM plane angles of the dominant and nondominant hand, wrist rehabilitation involving the DTM plane should be applied, whether the injured hand is the dominant or nondominant hand.
Conclusion
This study is the first to examine the DTM in the nondominant hand. The DTM plane angle varies by task and between participants. Most DTM plane angles were in the range of 20°–45° for the dominant hand and 15°–40° for the nondominant hand, as measured during dynamic daily activities. A range of different DTM plane angles were observed as a function of hand, task, and participant. On the basis of this observation, we conclude that, when performing wrist rehabilitation in the DTM plane, it is important to emphasize practice at various DTM plane angles. Future research should quantify the DTM plane angles in people after a wrist injury and compare the effects of conventional treatment with treatment that incorporates training in the DTM plane. Future research should also compare the effects of the aforementioned treatments on patients in different age groups, because age may also be a factor affecting upper limb kinematics (Gilliaux et al., 2016).
Footnotes
Acknowledgments
This work was part of Yael Kaufman-Cohen’s PhD thesis at the Sackler Faculty of Medicine, Tel Aviv University.