
Abstract
Eye–hand coordination, usually measured by a tracing task, and visual–motor integration (VMI), usually measured by copying figures, are involved in the ability to coordinate visual perception and finger–hand movement (Beery, 1997). Visual–perceptual capacities, fine motor skills, and the ability to integrate them have been considered as basic components underpinning the accomplishment of many daily functional activities (Cameron et al., 2012; Henderson, 1995). Eye–hand coordination and VMI abilities at a young age were found to predict later outcomes (e.g., school readiness; Bart et al., 2007). In addition, VMI difficulties have been reported for children with diverse disabilities (e.g., developmental coordination disorder [DCD]; Jarus et al., 2011).
It has been suggested that using a vertical surface might encourage appropriate wrist position and facilitate visual control (Benbow, 1995). The gravitational force applied during unconstrained arm movement may modify the movement dynamics (Gaveau et al., 2016). The upright position of the hand is related to proximal motor function (i.e., shoulder and upper arm) rather than distal motor function (i.e., wrist and fingers). Proximal function has been considered to be a prerequisite for distal function and manipulative hand use (Naider-Steinhart & Katz-Leurer, 2007). However, clinical experience has revealed positive outcomes on grasp when using the upright position of the hand while working on a vertical surface. Although the underlying motor processes of this strategy have not been carefully studied, it is a common practice for occupational therapy practitioners to recommend for a child with difficulties in drawing to use an inclined surface.
To determine the mechanism underlying this apparently effective treatment strategy, we have recently compared the level of performance of a tracing task and a copying figures task in horizontal and vertical postures in typically developing (TD) children (Portnoy et al., 2015). Compared with drawing on a horizontal surface, we found higher activity of the upper trapezius (UT) and biceps brachii (BB) and lower activity of the extensor carpi radialis (ECR) during drawing on a vertical surface. In addition, the ECR was more fatigued after the drawing activity on the horizontal surface. On the basis of these results, we aimed to compare the level of performance and muscle activity patterns in the two positions between TD children and children with mild disabilities (MD). We hypothesized that the performance on the vertical surface would be better for children with MD than on the horizontal one. Further comparison of muscle activity patterns between the two postures and groups was performed, because we expected higher muscle activation and fatigue in proximal muscles than in distal muscles during drawing on the vertical surface.
Method
Study Design
This was a mixed-design study, with the inclination of the surface as a within-groups factor, and the group (TD or MD) as a between-groups factor.
Participants
Twenty-two right-hand-dominant TD children (8 boys, 14 girls; mean [M] = 5.2 yr, standard deviation [SD] = 0.1) and 13 children with MD (9 boys, 4 girls; M = 4.9 yr, SD = 0.5) participated in this study. Inclusion criteria for the TD children were healthy and age 4–6. No significant difference in age was found between the two groups (p = .064). Exclusion criteria were any orthopedic or neurologic impairment or inability to understand and follow simple instructions.
Inclusion criteria for the children with MD were age 4–6 and on the wait list or at the beginning of an occupational therapy intervention process at the Department of Child Development, Loewenstein Rehabilitation Hospital (Raanana, Israel). The reasons for referrals were observable difficulties in performing daily activities. The referred children were assessed for MD (Gantschnig et al., 2013), including gross motor, fine motor, and visuomotor disabilities. Participants in the study group had a Beery–Buktenica Developmental Test of VMI (Beery VMI; Beery, 1997) shape-copying grade below the 50th percentile. Exclusion criteria were children in special education, neurological impairment, intellectual disability, genetic syndrome, or chronic medical impairment.
TD children were enrolled in full-time preschool programs and recruited through personal contact and snowball sampling. Children with MD were recruited through patient lists at the Loewenstein Rehabilitation Hospital. The study was approved by the Occupational Therapy Department ethics committee at the research facility and by the institutional review board of Loewenstein Rehabilitation Hospital (0022–14-LOE).
Research Tools and Protocol
The parents signed an informed consent form pretrial. Each participant was administered the Beery VMI. The participants were further divided into two groups matched according to Beery VMI percentiles. Half the participants were first tested with the horizontal orientation while sitting and then the vertical orientation while standing, and the other half were tested in the reverse order. The chair provided was fitted to the height of each participant.
A tablet (Galaxy Note 10.1 GT-N8010; Samsung, Seoul, South Korea) with an 11.5-cm-long stylus was used to test part of the Fine Manual Control subtest of the Bruininks-Oseretsky Test of Motor Proficiency (Wilson et al., 1995). The participants copied four shapes (circle, square, star, and wave) and completed two path-tracing tasks between broken or curved paths. The stylus tip coordinates were recorded at 125 Hz using custom Android (Alphabet Inc., Mountain View, CA) software and analyzed using custom software (Matlab R2012b, MathWorks, Natick, MA). The raw data were filtered using a second-order two-way low-pass (5 Hz cutoff) Butterworth filter. The tablet was placed in a wooden frame that held it in either a horizontal or a vertical orientation. The frame was placed on the table so that the participant could comfortably draw on the surface of the tablet while resting the arm on the table, as per the preference of each participant. In the vertical position, the frame was set so that the tablet was directly in front of the standing participant at shoulder height.
A telemetric surface electromyography (sEMG) system (Myon RFTD, Myon AG, Schwarzenberg, Switzerland) with a floating ground and pairs of bipolar Ag/AgCl surface electrodes was used. The UT, BB, and ECR were monitored. Electrode placement was performed according to the sEMG for a noninvasive assessment of muscles (SENIAM) guidelines. Data were collected at 1000 Hz and bandpass filtered (dual-pass second-order Butterworth, 10–500 Hz). Data were acquired and analyzed using custom software (LabView V12, National Instruments, Austin, TX). The participants performed several maximum voluntary contractions (MVCs) for 5 s for each muscle (Burden, 2010).
Data Analysis
The amount of time that the stylus contacted the tablet was computed for each task. In addition, the total number of acceleration zero crossings (AZC) more than 100 ms apart in both lateral and vertical directions was computed as a measure of the fluency of the drawing.
For the copied shapes, we varied the scale and location parameters of the shape drawn by the participant to minimize the sum of the squared distance between the curve drawn and the ideal curve, using the simplex algorithm. The algorithm produced an ideal shape (e.g., a perfect circle) that best aligned with the shape drawn by the participant. Some characteristics of the ideal shape were compared with the characteristics of the prototype shape, provided in the original test for copying. The following properties of quality were considered: mean error (the mean distance between the drawn and ideal shapes), scale (the scale difference between the ideal and prototype shapes; e.g., a 2 means the ideal shape is double the size of the prototype), and shift (the distance between the ideal and prototype shapes). For the path-tracing task, the percentage of time inside or on the lines and the shortest distance from a center line were calculated.
For each muscle, the MVC value was computed as the average of three peaks, which differed by no more than 10% from one another. The mean root mean square values of the sEMG data of each muscle were normalized by MVC. Frequency analysis was performed on the sEMG data of both mazes. The median power frequency (MDF) was computed after a short-time Fourier transform spectrogram calculation using a Hanning sliding 500-ms window. A decrease in MDF is associated with an increase in fatigue (Alfonsi et al., 1991).
Statistical analysis was performed using IBM SPSS Statistics (Version 22, IBM Corp., Armonk, NY). A mixed-design multiple analysis of variance (MANOVA) was used, with within-subjects factors of surface inclination and shape drawn and a between-group factor of participant group (TD or MD). The MANOVA was performed on the graphical product quality and muscle activation patterns. For the graphical product quality measures, a separate MANOVA was performed for the shape-copying tasks and the path-tracing tasks because of the use of different outcome measures. When the MANOVA was significant, unilateral ANOVAs were performed on the outcome variables. p < .05 was considered statistically significant.
Results
Graphical Product Quality: Copying Shapes
We found a significant between-group main effect, F (5, 29) = 5.41, p = .001. The MD group was slower than the TD group (M = 7.90 s, SD = 0.66, compared with M = 5.50 s, SD = 0.49; F [1, 33] = 9.02, p = .005), had greater magnitude of error (M = 0.37 cm, SD = 0.03, compared with M = 0.30 cm, SD = 0.01; F [1, 33] = 7.46, p = .01), and had more AZC (M = 39.5, SD = 3.2, compared with M = 24.1, SD = 2.2; F [1,33] = 13.7, p = .01).
A significant main effect was found for the inclination, F (5, 29) = 3.47, p = .014. This effect was significant for movement time, F (1, 33) = 11.5, p = .002, with vertical movements (M = 6.18 s, SD = 0.39) faster than horizontal movements (M = 7.23 s, SD = 0.47), and for AZC, F (1, 33) = 7.99, p = .008, with more AZC in the horizontal inclination (M = 34.3, SD = 2.4) than in the vertical inclination (M = 29.3, SD = 2.1).
The shape also had a significant effect on the outcome measures, F (15, 19) = 27.8, p < .001, because of a significant difference in all five measures (Figure 1). Because this result is expected and not related to our hypotheses, it is not further analyzed.
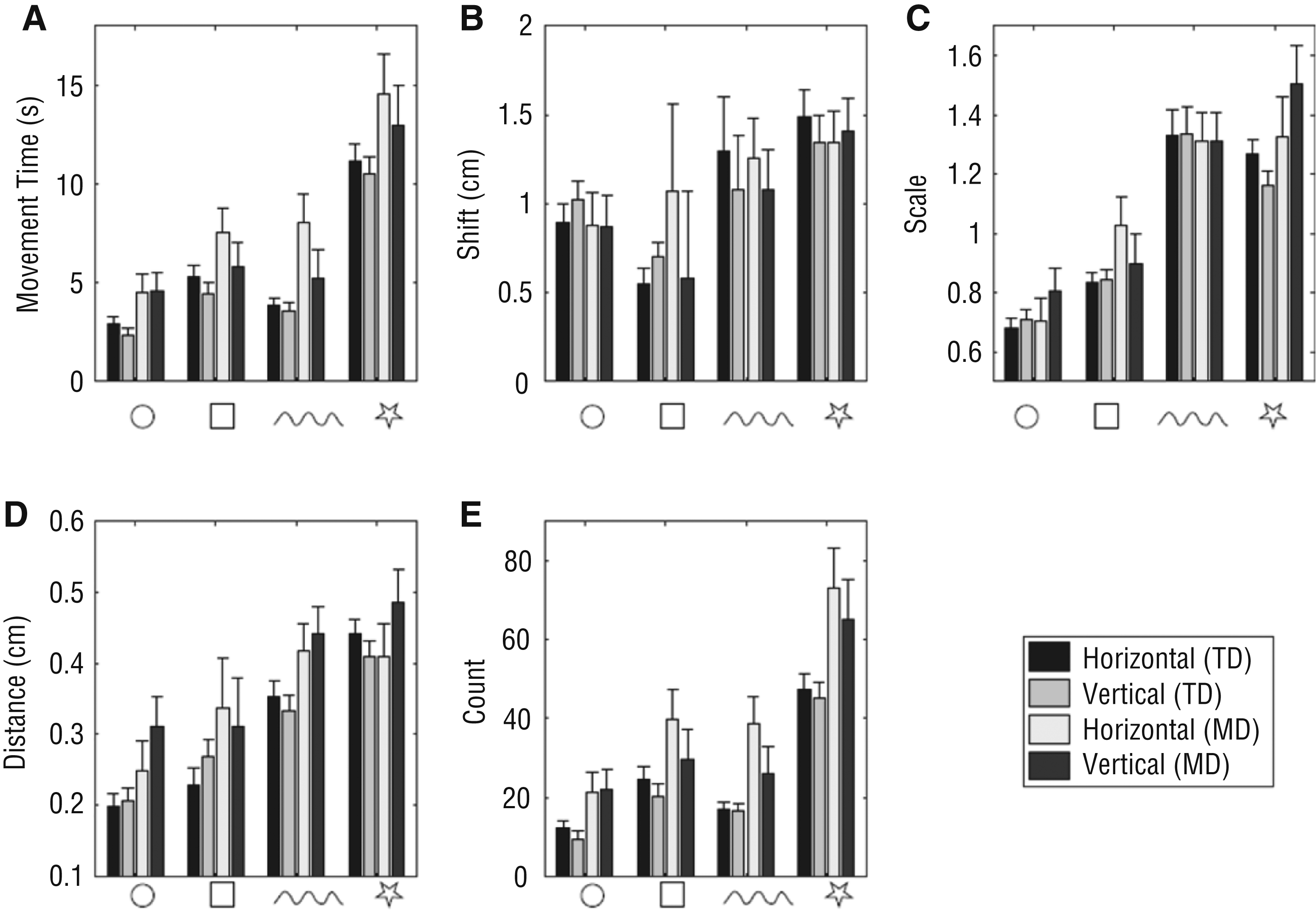
Copying task performance measures for the TD and MD groups.
A significant interaction was found for shape and group, F (15, 19) = 2.53, p = .029. For both groups, the magnitude of error increased with the complexity of the shape, but the difference is smaller for the most complex shape (i.e., star; Figure 2). t tests showed that although the simple shapes showed significantly less error in the TD than in the MD group (i.e., circle: M = 0.20 cm, SD = 0.01, vs. M = 0.28 cm, SD = 0.03; t [33] = –2.61, p = .014; square: M = 0.25 cm, SD = 0.02, vs. M = 0.32 cm, SD = 0.03; t [33] = –2.05, p = .048; wave: M = 0.34 cm, SD = 0.02, vs. M = 0.43 cm, SD = 0.03; t [16.8] = –2.44, p = .02), the star did not show a significant difference between the groups (M = 0.43 cm, SD = 0.02, vs. M = 0.45 cm, SD = 0.04; t [33] = –0.55, p = .58).
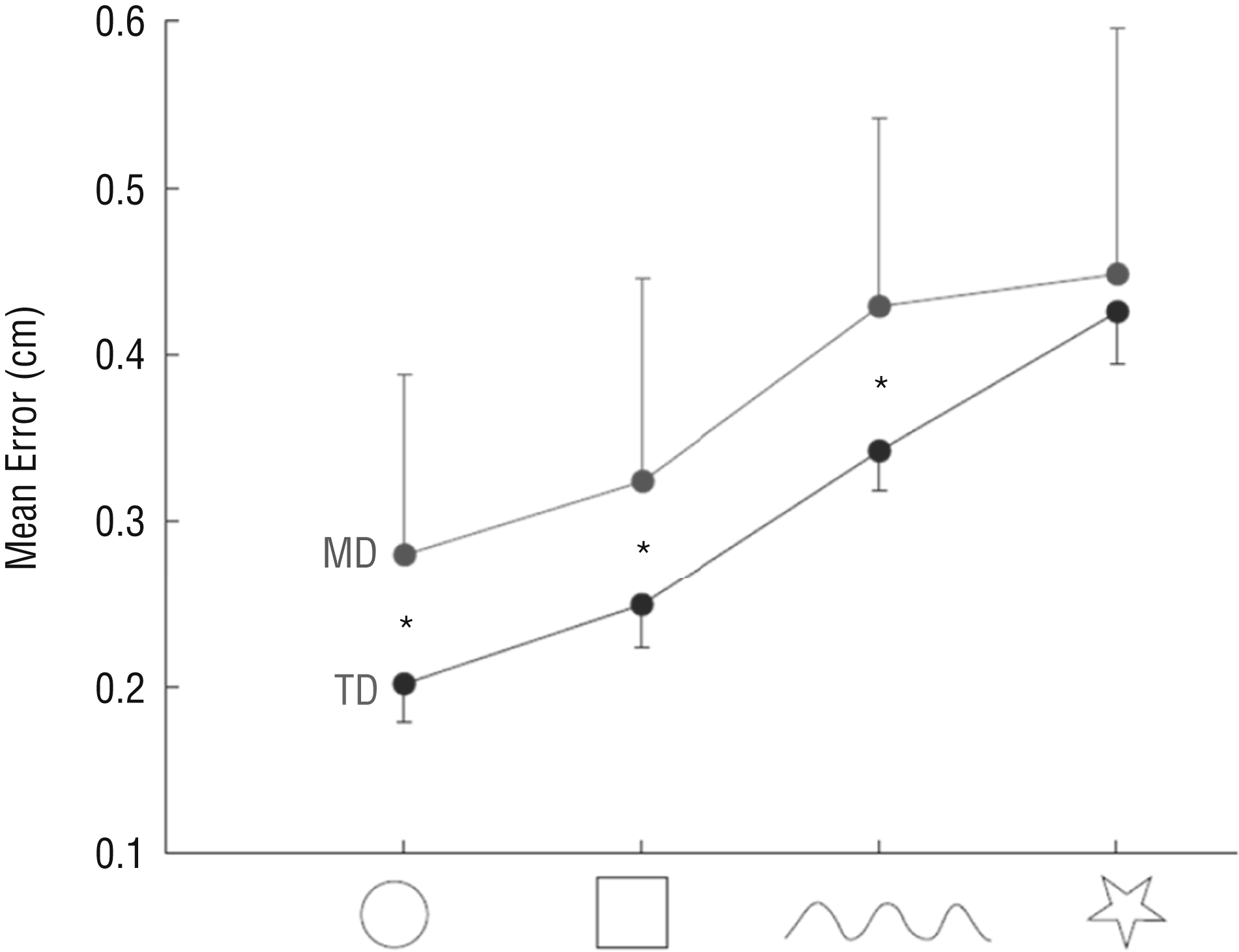
Mean error of the copying tasks for the TD and MD groups.
Graphical Product Quality: Path Tracing
There was a main effect of group, F(4, 30) = 4.39, p = .006. The MD group showed a larger number of zero crossings than the TD group (M = 142.2, SD = 11.6, compared with M = 111.7, SD = 8.9; F[1, 33] = 4.32, p = .046). A main effect was found for the inclination, F(4, 30) = 2.83, p = .042. In the horizontal inclination, movement times were slower than in the vertical inclination (M = 24.5 s, SD = 1.51, vs. M = 21.6 s, SD = 1.22; F[1, 33] = 8.15, p = .007), percentage inside was greater (M = 84.8%, SD = 2.2, vs. M = 81.8%, SD = 2.1; F[1, 33] = 4.58, p = .04), distance from the center was lower (M = 0.13 cm, SD = 0.01, vs. M = 0.17 cm, SD = 0.02; F[1, 33] = 8.27, p = .007), and there were more AZC (M = 135.5, SD = 8.8, vs. M = 118.5, SD = 7.1; F[1, 46] = 7.62, p = .009).
A main effect was found for the maze type, F(4, 30) = 44.3, p < .001, and differences in all four measures were significant (Figure 3). Because this result was expected, it is not further analyzed. The interactions between maze type and group and between maze type and inclination were not significant.
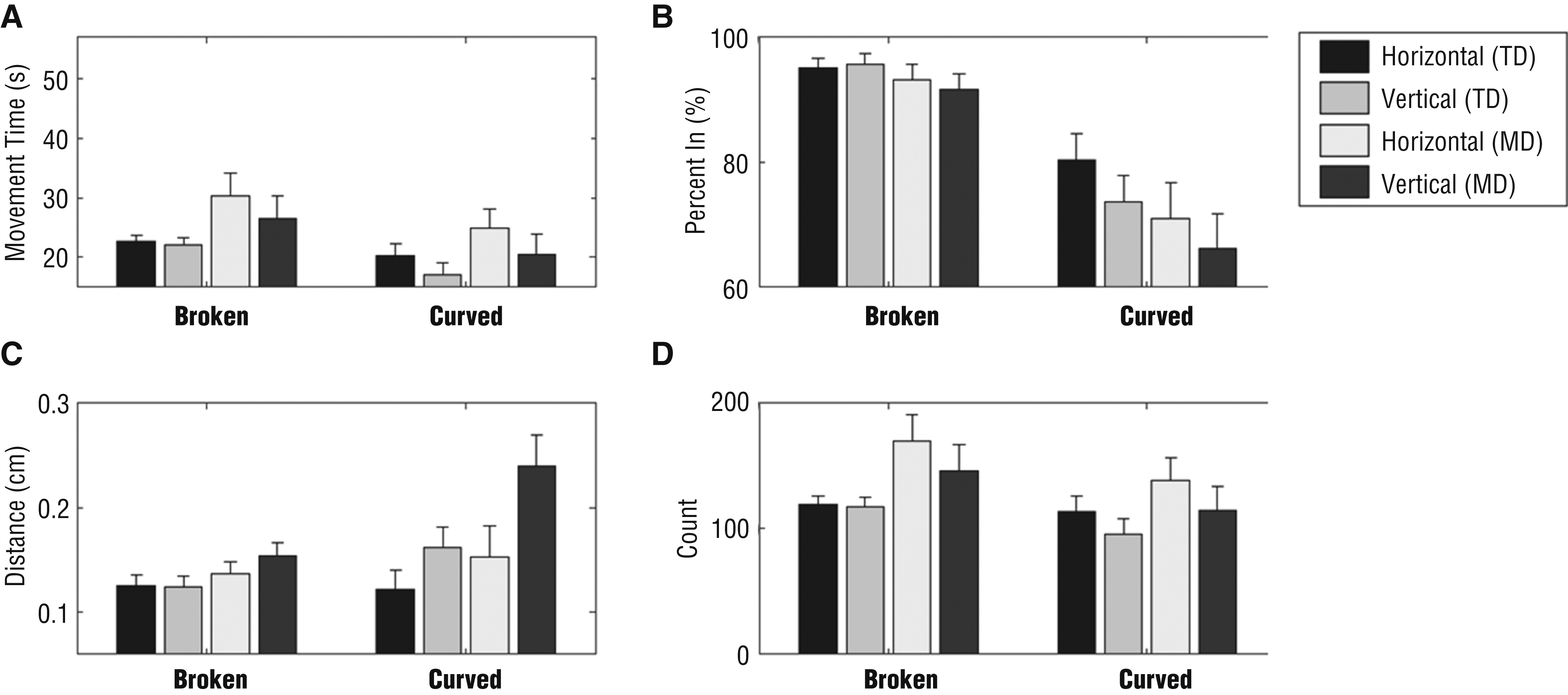
Path tracing performance measures for the TD and MD groups.
Muscle Activity Patterns
Table1 depicts the mean normalized muscle activity and the MDF for the three monitored muscles. We found a significant between-subjects main effect, F (9, 29) = 3.734, p = .008. During path tracing, children with MD had lower activity of their ECR than did the TD children. In addition, the MDF of their ECR was significantly lower than that of the TD children.
TD Group and MD Group Mean Normalized Muscle Activity and MDF, by Muscle and Tablet Orientation
Note. TD group, n = 35; MD group, n = 13. BB = biceps brachii; ECR = extensor carpi radialis; MD = mild disabilities; MDF = median power frequency; Mdn = median; MVC = maximal voluntary contraction; TD = typical development; UT = upper trapezius.
Within-subjects statistical differences, p ≤ .005.
There was a significant main effect for the inclination, F (9, 29) = 4.566, p = .003. The univariate ANOVAs did not show a difference in the mean muscle activity while using the vertical surface compared with the horizontal surface. However, the MDF of the ECR was significantly lower during path tracing on the horizontal surface than on the vertical surface, F (1, 26) = 25.106, p < .001.
An Inclination × Group interaction effect was found, F (9, 29) = 2.680, p = .036. The interaction effect was significant for the MDF of the ECR during path tracing, F (1, 37) = 8.425, p = .007, because the MDF of the ECR in the TD group was lower on the horizontal surface than on the vertical surface, whereas the MDF of the ECR in the MD group was similar between these surfaces.
Discussion
In this study, we compared the copying and tracing performance of children with MD and TD on a vertical versus horizontal surface. Our main findings show that the children performed faster and smoother movements when copying shapes on the vertical surface. When tracing the mazes, the participants traced further from the maze center on the vertical surface. Additionally, children with MD increased the activation of the UT while copying shapes on the vertical surface but showed no difference in muscle activation levels while tracing on the two surfaces and no muscle fatigue.
When copying shapes, children with MD were slower, their movements were less smooth, and their copied shapes had greater errors than those of the TD children. It would be expected that slower movement would allow greater accuracy and, therefore, smaller errors, but this trade-off was not observed in the MD group. Previous studies investigated the speed for accuracy trade-offs in TD children and children with DCD performing real and imagined visually guided pointing tasks (Maruff et al., 1999; Wilson et al., 2001). In TD children, the speed–accuracy trade-off followed Fitts’ law, stating that the time required to reach a target is a function of the ratio between the distance to the target and the width of the target. However, in children with DCD, imagined movements did not conform to Fitts’ law, suggesting that the ability to generate internal representations of movements in children with DCD is impaired. Another interesting finding was that the differences in copying errors between the two groups were high for the simpler shapes but similar for the more complex shape (star), which likely poses a high difficulty level for both TD children and children with MD. This finding suggests that clinical evaluation of 4- to 6-yr-old children is better accomplished using the simple shapes.
The children performed faster and smoother movements when copying shapes on the vertical surface than on the horizontal surface. Because we found no significant differences in the accuracy of the copied shapes between the two surfaces, this finding suggests an improvement in terms of speed–accuracy trade-off (i.e., maintaining graphical quality while increasing the movement velocity). This result may explain positive reports from clinicians regarding the application of vertical surfaces in clinical settings, because if the child is able to perform the task faster, yet maintain good graphical quality, it might require less effort and increase motivation. Changes in posture (e.g., by changing seating type) are also known to affect motor skill performance in children (Smith-Zuzovsky & Exner, 2004).
Interestingly, the MD group was slower for the broken maze than for the curved maze, the opposite of the pattern seen for the TD group. The MD group also showed a large drop in accuracy in the curved maze (compared with the TD group), much greater than the difference for the broken maze. It demonstrates that the MD group had significant difficulty with accuracy constraints but showed similar performance to the TD group in the ability to make complex movements (reflected in the similar number of acceleration zero crossings between the groups).
When using the vertical surface, the distance from the center was greater in both paths (i.e., performance was worse) than when using the horizontal surface. Note that this finding is different from the findings for the copying tasks, in which differences were observed in timing (faster movements for the vertical orientation, as was also observed for the tracing tasks) but not in graphical quality. These findings suggest that for tracing tasks there is a larger degradation of performance when using the vertical orientation. Thus, it seems that the vertical orientation is more suited to tasks with lower accuracy demands (e.g., copying tasks). The differences observed between tracing tasks and copying tasks may be the result of differences in the feedback requirements; however, this is a topic that requires further investigation.
In this study, children with MD incorporated similar muscle activation strategies during the copying and tracing tasks as TD children but had lower activity of the ECR during path tracing than the TD children. Hence, the ECR in children with MD was not fatigued. When copying shapes on a vertical surface, children with MD showed higher activity levels of the UT than when copying on a horizontal surface. This finding is not surprising because an accepted principle is that proximal stability is a prerequisite for manipulative hand use. Accordingly, in contrast to the conditions during drawing on a table, the vertical surface lacks a means of support for the elbow or forearm, thereby compelling the child to maintain the stability of the proximal upper extremity to allow distal control.
A possible clinical application may be using a short task of copying shapes or letters to assist in strengthening proximal muscles, consequently resulting in better control of the upper extremity. However, this conclusion cannot be deduced from the shape-copying task alone because the high activity levels of the UT in the MD group during shape copying on the vertical surface did not occur during path tracing. Consequently, no fatigue was registered in the three muscles. Whereas the BB and ECR were more fatigued when TD children traced a path on the horizontal surface compared with the vertical surface, there was no statistically significant difference in the MDF in all three muscles of the MD group between vertical and horizontal surfaces.
Implication for Occupational Therapy Practice
This study has the following implication for occupational therapy practice:
Incorporating short copying tasks on a vertical surface may increase the control of proximal muscles and ease the graphomotor performance in children with mild disabilities.
Study Limitations
Several limitations of this study should be considered. First, the small sample size of the MD group may not reflect the general population. Additionally, the study was conducted using a tablet without the typical drawing tools that the participants were accustomed to instead of the typically used drawing board.
Conclusion
This study shows some benefits of performing a short copying task in the vertical orientation. Mainly, the movements of children with MD on the vertical surface were faster and smoother, with no reduction in accuracy, than their movements on the horizontal surface. Moreover, they exerted their UT while performing the short tasks on the vertical surface. We therefore conclude that incorporating short copying tasks on a vertical surface may increase the control of proximal muscles and ease the graphomotor performance in children with MD.