
Abstract
Discontinuity of axons and nerve fibers results in sensory and motor function deficits distal to the lesion site after a peripheral nerve is injured. Wallerian degeneration, axonal regeneration, and end-organ reinnervation are long-term processes of nerve recovery in patients with peripheral nerve repair. However, the return of sensation remains disappointing for adult patients after nerve repair (Chemnitz et al., 2013; Lundborg & Rosén, 2007) despite the development of microsurgical repair techniques and instruments in recent years. Several contributing factors, such as the imperfect survival rate of the nerve cell bodies, poor axonal outgrowth rate and orientation, atrophy of target organs, and the mismatch of fiber–receptor combination, may affect the outcomes after nerve anastomosis (Sunderland, 1978). However, it is worth noting that a rapid process of functional reorganization of the cortex after nerve injury has been reported in several neuroscience and neuroimaging studies (Merzenich & Jenkins, 1993; Wall et al., 2002).
In a classical sensory reeducation program, the intervention should be initiated when the patient begins to feel touch perception out to the fingertips and, in general, a prolonged period is required for the reconnections between the nerve fibers and sensory receptors to occur (Dellon, 1981); that is, the projected sensorimotor cortex of the affected nerve may be vacant before the nerve fibers are reinnervated into the receptors (Chen et al., 2002). As reported in a previous study, cortical reorganization after peripheral nerve injury might be the main reason for the imperfect sensory return after hand surgery (Chen et al., 2002). Moreover, one study revealed a positive association between sensory input and cortical activation (Fornander et al., 2010). Therefore, an initial increase in the activated volume may alter the return of sensory function after a nerve injury, which indicates an important and potential mechanism for neurological rehabilitation (Knecht et al., 1998).
Mirror therapy, a top-down treatment model, modulates central nervous system processing (Ramachandran & Altschuler, 2009) to enhance treatment effectiveness after peripheral nerve injury and repairs in the hand. When looking into a mirror and experiencing synchronization of the mirror illusion and the touch stimuli of the unaffected hand, the patient gets a perception of tactile stimuli in the insensate hand (Rosén & Lundborg, 2005). Mirror therapy provides artificial sensation to feed the cortex, which has the effect of reducing learned nonuse for the affected hand (Michielsen et al., 2011). Moreover, the clinical significance of early mirror therapy for sensory function in patients with nerve injury has been demonstrated (Rosén et al., 2015). However, the patients recruited in the previous study had nerve injury only from distal forearm to wrists.
The effects of mirror therapy in rehabilitation after hand surgery have been investigated by researchers using touch-observation but not task-based movement (Rosén & Lundborg, 2005). In addition, the improvements that may or may not occur in the delicate sensorimotor control and function of the hand (Oud et al., 2007) have received relatively little attention with regard to patients who received sensory reeducation training. Consequently, the purpose of this study was to study the effects of a practical mirror therapy protocol that includes an integrated program of touch-observation and task-based mirror therapy in patients with injury levels from elbow to midpalm. The hypothesis was that using mirror therapy for sensorimotor reeducation in the early phase after nerve repair might reduce cortical reorganization, thereby encouraging more rapid return of function.
Method
Research Design
We used an assessor-blinded study with a randomized controlled design.
Participants
The participants included patients with nerve repair who experienced one of the following five injuries: (1) median or ulnar nerve injury, (2) a combination of nerve and tendon or vascular injury, (3) injury sites between the level of midpalm and elbow, (4) Class 3 injury type (neurotmesis type) under Seddon’s (1942) classification, and (5) lacking or impaired sensation of the hand. Exclusion criteria were deficits in cognition or language comprehension and severe limitations in the range of motion of the upper limbs. Patients who met the inclusion criteria were referred by the plastic surgery clinic of a university hospital in southern Taiwan. Sealed opaque envelopes with a prefilled numbered series were used to conceal group allocation. Eligible patients were randomized in a 1:1 ratio to either the experimental or the control groups by stratifying on the basis of the injury level.
Ethics Statement
Before participation, each participant was informed of the experimental purposes and procedures and then was asked to sign a consent form approved by the National Cheng Kung University Hospital institutional review board.
Intervention
The participants in the experimental and control groups received training for 12 wk, at a frequency of three sessions per week. For the experimental group, before reaching the pressure threshold of 4.31 on the Semmes–Weinstein monofilament (SWM) test (Bell-Krotoski et al., 1995), the participants received 15 min of mirror therapy. This treatment was followed by 20 min of regular hand therapy under an occupational therapist’s supervision based on the protocol in the protective phase, including early and late mobilization and strengthening, and 20 min of physiotherapy in each treatment session.
Mirror Therapy Protocol.
The touch-observation and task-based mirror therapy protocol is designed to promote sensory return for hands with traumatic nerve injury. The protocol is conducted before the hand reaches a pressure threshold of 4.31 on the SWM test. It comprises two phases: a phase of touch-observation mirror therapy and a phase of task-based mirror therapy, with each phase addressing the different components of the sensory reeducation program. The phase of touch-observation mirror therapy begins in Week 1 after nerve repair with the following procedures.
In Phase 1, each participant places his or her affected hand in the mirror box and concentrates on the mirror reflection of the uninjured hand while the therapist applies different texture stimulations to the uninjured hand. After Week 4 subsequent to nerve repair, the phase of task-based mirror therapy replaces the touch-observation mirror therapy. Following the same protocol as the touch-observation mirror therapy, each participant places his or her affected hand in the mirror box. While the participant concentrates on the mirror reflection, the uninjured hand performs the specific sensory activities of the needed motor function, such as (1) touching objects with different shapes and textures, (2) picking up objects from a background medium, and (3) using a work-simulated task with different sensory surfaces. After the affected hand regains protective sensation (reaching a pressure threshold of 4.31 on the SWM test), the experimental program is replaced with a discriminative sensory reeducation program, with the training involving texture recognition, geometric discrimination, and object manipulation.
Control Group Protocol.
For the control group, before the return of protective sensation, the participants received 15 min of classical sensory reeducation followed by 20 min of regular hand therapy and 20 min of physiotherapy in each treatment session. The classical sensory reeducation program included a program of protective sensory reeducation, exercise for reeducating the perception of constant pressure or moving touch across a specific area, and exercise for reeducating precision pinch force control. Following the mirror therapy protocol, after the protective sensation returned, the discriminative sensory reeducation program commenced.
During the period of the immediate intervention to 12 wk after treatments, scar management, stretching blocking exercise, and muscle strengthening protocols were provided as home programs for all the recruited participants. As for sensory deficits, visually guided object-manipulation tasks were carried out as a home-based sensorimotor reeducation for both the experimental and control groups.
Outcome Measures
Outcome measurements were obtained at pretreatment (Time 1 [T1]), immediately after treatment (Time 2 [T2]), and 12 wk after the last treatment (Time 3 [T3]). The sequences of the following tests were randomized to minimize potential order effects during the assessments:
SMS test. The SMS test is a light touch-deep pressure test that is used as one of the objective tests for evaluating hand sensibility (Bell-Krotoski et al., 1995). It uses 20 filaments with different hair diameters indicating different sensitivity thresholds. During the test, the filament exerts a constant force onto the skin area for 1–1.5 s. The threshold is defined as the lightest filament for which the participant can respond to the stimuli correctly in at least one out of three trials. The testing sites were located at the proximal phalanx of the index finger for the hands with median nerve injuries, and the pulp of the little finger for those with ulnar nerve injuries (Bell-Krotoski, 2002). The applied force determined from the SNS test was used to define the pressure threshold of hands.
Static 2-point discrimination test. The 2-point discrimination test was used to determine the smallest distance between two prongs of a discriminator that a participant could perceive, and the results correlated with the hand’s grasp ability (Dellon, 1978). During the test, the fingertip was supported by the examiner, and the discriminator was placed on the finger pulp with either a 1- or 2-point stimulus, which was given randomly.
PPT. The PPT (Amirjani et al., 2011) is a fine fingertip dexterity test with acceptable validity and reliability. The participants were timed as they arranged pins and assembled pins, washers, and collars. The results of the Unilateral Pin Insertion, Bilateral Pin Insertion, and Assembly subtests were consistent with one another.
Minnesota Manual Dexterity Test (MMDT; Desrosiers et al., 1997). The MMDT is used to measure the gross motor skills of the upper extremities. The time it took for the participants to complete the Placing and Turning subtests was recorded in this study.
Pinch-holding-up-activity test. The pinch-holding-up-activity test is used to determine the sensorimotor control of a hand (Chiu et al., 2014). This test was conducted with a reliable pinch apparatus (Chiu et al., 2009). The participants pinched this apparatus using the pulps of the thumb and index finger. They were then asked to lift the apparatus to about 5 cm above the table and hold it at this position for 5 s (holding phase). Afterward, they lifted the apparatus from a height of 5 cm to 30 cm (lifting phase). After three trials of the test, the participants performed a pinch with their maximal pinch force exertion at a height of 30 cm above table to determine the static maximal pinch force. The ability of adjusting pinch force according to changes in the inertial load (Figure 1) during the lifting phase is a sensitive parameter that can be used to assess sensorimotor control in the hand (Flanagan & Wing, 1995; Hsu et al., 2009). The following parameters were analyzed in the pinch performance: (1) FRPeak: the ratio between peak pinch force and maximum load force of the pinch apparatus during the lifting phase; (2) FRMean: the mean force ratio (pinch force/load force) at each time frame during the lifting phase; and (3) percentage of maximal pinch strength: peak pinch force divided by maximal static pinch force, which gives the percentage of maximum voluntary contraction.
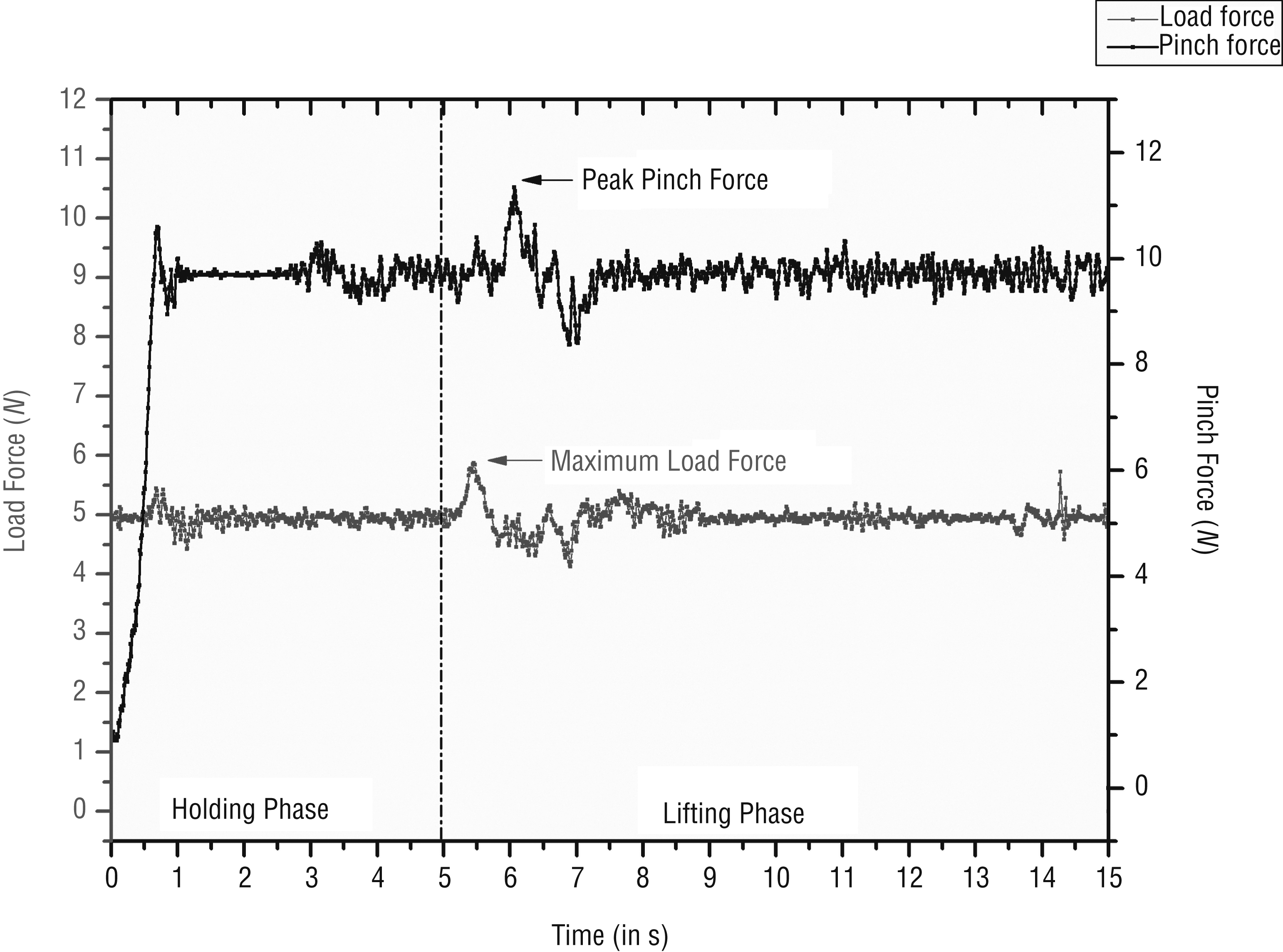
Pinch force and load force in a force–time relationship.
Statistical Analysis
IBM SPSS Statistics (Version 17; IBM Corp., Armonk, NY) was used for all statistical analyses. Descriptive statistics were used to describe the clinical characteristics of the participants with nerve repair and the results of the SWM test, pinch-holding-up-activity test, PPT, and MMDT. Friedman’s test (a nonparametric, repeated-measures comparison) was used to compare the testing outcomes across T1, T2, and T3 for each group. The Wilcoxon signed-rank post hoc test was used to examine whether any differences existed among the time points. The Mann–Whitney U test was used to indicate the difference in the treatment effects between the experimental and control groups. The level of significance was set at p < .05.
Results
A total of 12 participants were recruited in this study from December 2014 to May 2015. Four had injuries to their dominant hands. Details of their demographic and clinical features are presented in Table 1. All 12 participants completed the training, and 11 participants were assessed 12 wk after the training period. A flowchart giving details of the enrollment of the participants is shown in Figure 2.
Demographic Data and Clinical Features of the Recruited Patients at T3
Note. M = mean; SD = standard deviation; T3 = Time 3, 12 wk after the last treatment.
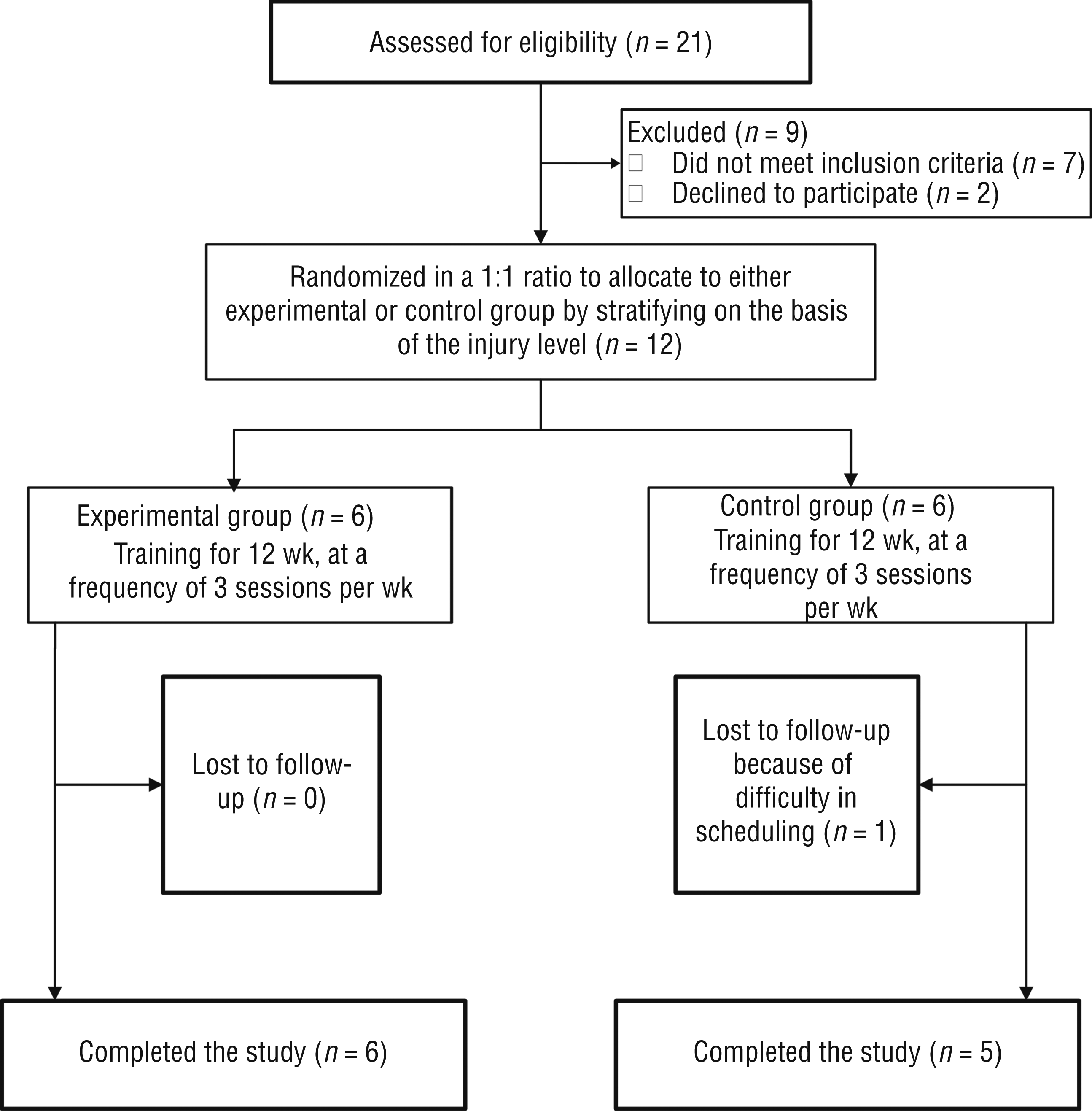
Flowchart of participant recruitment and the experimental process.
Sensibility
There was significant improvement in touch-pressure thresholds for both groups (p < .05). However, the change in the SWM test revealed no significant differences between groups (p = .240 and .310 for T1–T2 and T1–T3, respectively; Table 2). With regard to the discriminative sensation, no participant could discriminate 1- or 2-point stimuli for the static 2-point discrimination test at T1. In the experimental group, 2 patients at T2 and 4 patients at T3 had their discriminative sensation return (<15 mm) in the 2-point discrimination test. In the control group, 2 patients at T2 and 3 patients at T3 had their discriminative sensibility return.
Change Differences in the Results of Touch Sensibility, the Pinch-Holding-Up-Activity Test, and Hand Function Tests Between Different Treatment Groups and Within the Groups at T1, T2, and T3
Note. Values represent mean ± standard deviation. Friedman’s test was used to compare testing outcomes across T1, T2, and T3 for each group. The Mann–Whitney U test was used to assess the differences in the treatment effects between the experimental and control groups. FRMean = the mean force ratio (pinch force/load force) at each time frame during the lifting phase; FRPeak = the ratio between peak pinch force and maximum load force of the pinch apparatus during the lifting phase; MMDT = Minnesota Manual Dexterity Test; PPT = Perdue Pegboard Test; SWM = Semmes–Weinstein monofilament test; T1 = Time 1, pretreatment; T2 = Time 2, immediately after treatment; T3 = Time 3, 12 wk after the last treatment.
Indicates Purdue Pegboard Test.
Indicates statistical significance at p < .05.
Sensorimotor Control
The effects of the mirror therapy are seen in the results of the pinch-holding-up-activity test. The changes in the parameters of FRPeak (FRPeak = 3.64 ± 0.56, 3.16 ± 0.34, and 3.10 ± 0.26 for T1, T2, and T3, respectively, p = .0011), FRMean (FRMean = 2.79 ± 0.39, 2.44 ± 0.42, and 2.31 ± 0.32 for T1, T2, and T3, respectively, p = .0016; see Table 2), and percentage of maximal pinch strength (60.67% ± 20.04%, 49.17% ± 19.43%, and 42.50% ± 13.81% for T1, T2, and T3, respectively, p = .0030; see Table 2) all reached significance for the experimental group. However, the parameters of FRPeak, FRMean, and percentage of maximal pinch strength did not show any statistical significance for the control group. In addition, although there was a significant difference in the change of percentage of maximal pinch strength (p = .015 for T1–T2, and p = .093 for T1–T3) between the experimental and control groups, there were no significant differences in the changes in FRPeak (p = .31 for both T1–T2 and T1–T3) and FRMean (p = .485 and .818 for T1–T2 and T1–T3, respectively).
Hand Function
Both groups revealed significant improvements in the unilateral (p = .03 for both groups) and bilateral (p = .03 for the experimental group, p = .04 for the control group) Pin Insertion subtests. The results of the Assembly subtest improved significantly in the experimental group but not in the control group. In addition, the mirror therapy program indicated better treatment efficacy in the results for the PPT Unilateral Pin Insertion (p = .015), Bilateral Insertion (p = .041), and Assembly (p = .041) subtests from T1 to T2 (see Table 2). The changes in the PPT Unilateral Pin Insertion (p = .015) and Assembly (p = .041) subtests from T1 to T3 also showed a significant group difference. The change in the results of the Placing and Turning subtests of the MMDT from T1 to T2 did not show any significant differences between groups, but there was a statistically greater change in the Turning subtest for the experimental group from T1 to T3 (p = .026; see Table 2).
Discussion
The results obtained in this work were partially consistent with our hypothesis. Our findings showed that early mirror therapy provided better treatment effects with regard to the function and sensorimotor control of the hand in patients with nerve injuries than among those who received a classical reeducation program. However, the mirror therapy did not have better effects with regard to sensation recovery in the injured hand than in patients treated with with the classical sensory reeducation program. Our findings were thus different from the results in a previous experiment (Rosén et al., 2015). We should note that the injury levels of the recruited patients were quite different in these two studies. In the current work, the injured sites were between the level of the midpalm and elbow, whereas in the previous study, they were in locations distal to the forearm, and thus the processes of nerve regeneration in the current study were relatively complex. Several irreversible changes, such as atrophy in sensory target organs (Grinsell & Keating, 2014; Sunderland, 1978) and reduced releasing of neurotrophic factors (Höke et al., 2002), are likely to have caused the nerves not to innervate in a timely manner in the current study. In addition to the maintenance of the functions of the cortical representation area, the sensory outcomes must be affected by additional factors for patients whose injury level was more proximal than midpalm, and thus there was no notable difference in the sensory improvement between the two groups.
According to the outcomes of FRPeak and FRMean, the patients’ capability regarding the adjustment of the force interactions between the object and hand became much better along the regeneration course in the experimental group, but not in the control group. Although the improvements in FRPeak and FRMean seen in the patients did not reveal any notable difference between the two groups, the parameter of percentage of maximal pinch strength detected by the pinch-holding-up-activity test demonstrated the better results found in the experimental group. To our knowledge, loss of nerve integrity for either the median or ulnar nerve at the level of the elbow, forearm, and proximal part of the hand results in sensory and motor impairments; specifically, the performance of pinch strength would be affected by this occurrence, and thus the parameter of percentage of maximal pinch strength, which uses the peak pinch force normalized with the maximum pinch strength, could be a better indicator for monitoring the sensorimotor control of the hand for patients with nerve injury (Shieh et al., 2011). The underlining mechanism of mirror therapy, as used in clinical practice, is associated with the function of mirror neurons (Rothgangel et al., 2011). Because motor skills were involved in the task-based mirror therapy phase of the current work, the motor neurons were thus discharged through the observation of actions performed by the patients themselves, and this manifestation then modulated their motor behaviors (Rizzolatti et al., 2009).
Along with the measures of the sensorimotor functions, considerable differences were also found in the improvements of the Pin Insertion and Assembly subtests of the PPT between the experimental and control groups. Task-based mirror therapy has been proven effective in improving hand function in patients with chronic stroke (Arya & Pandian, 2013), but its effects in patients with nerve injury have not yet been analyzed. In this study, the use of early mirror therapy revealed clinical benefits with regard to both the sensorimotor control and dexterity of the hand, with the results being better than those seen with classical sensory reeducation programs. The reason for the better treatment outcomes with the touch-observation and task-based mirror therapy may be the greater activation of the mirror neurons during task execution (Arya et al., 2012). In particular, the use of mirror therapy with a specific sensory activity provides both sensory and motor input, which has more positive effects on the motor responses (Shadmehr et al., 2010). The positive changes in hand function not only provide objective evidence of the training effects of early mirror therapy for a hand with nerve injury but also meet the goal of providing a new strategy for nerve injury intervention (Grinsell & Keating, 2014).
Mirror therapy, through the use of a visual illusion, alters the processing of the neural network and then facilitates interlinkages between areas of the sensory and motor cortices in the brain (Arya, 2016). However, there is little evidence regarding the effects of mirror therapy on hand function for patients with traumatic nerve injury. The results of this study show that the practical mirror therapy protocol has the potential to have better treatment effects on the motor and functional performance of the hands of patients with nerve injury than those seen with the classical sensory reeducation program. However, lack of the measures regarding the patient-reported outcomes to assess the patient’s perception of improvement is one of this work’s limitations. The relatively small sample size used in this work is another limitation. Finally, the duration of follow-up used in the current work might have been too short to obtain the final results of nerve regeneration. Thus, a longer duration of follow-up is required in future studies.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Touch-observation and task-based mirror therapy may improve sensorimotor control and functional capability of hands for patients with peripheral nerve injury.
Touch-observation and task-based mirror therapy can provide a practical sensorimotor reeducation program for the early phase after nerve repair.
Conclusion
The findings in this study indicate that the touch-observation and task-based mirror therapy program has potentially positive effects on the sensorimotor and functional performance of hands with nerve injuries.
Footnotes
Acknowledgments
This work was financially supported by the Medical Device Innovation Center, National Cheng Kung University, from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education in Taiwan. This work was also supported by Ministry of Science and Technology Grant 103-2314-B-384-005. We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated. This study was approved by the institutional review board of the National Cheng Kung University Hospital (clinical trial registration number: B-ER-102-389).