
Abstract
The Individuals With Disabilities Education Act of 1990 (Pub. L. 101-476) Early Intervention program supports healthy development and improved short- and long-term outcomes for young children (ages 0–3 yr) at risk for developmental delay (Adams & Tapia, 2013). The benefits of its family-centered services are numerous, but identifying effective intervention strategies is difficult because of the great variation in service delivery among programs and providers (Spiker et al., 2000).
Training parents to incorporate strategies into a child’s natural environment has been endorsed as best practice, yet evidence to support methods of parent training is limited (Shapiro et al., 2014). Additionally, parents report difficulty intervening on a daily basis and building new routines (Golley et al., 2011). Effective and replicable methods of parent training are needed to maximize the benefits of early intervention.
Incorporating elements of behavioral activation (BA) into parent training may allow parents to enrich a child’s natural environment and alter daily routines incrementally. BA provides a framework to motivate the adoption of new routines by establishing small, attainable goals and building confidence as each goal is met (Wallbridge et al., 2008). It is an effective intervention for changing behavior to help people establish new, healthy routines (Cuijpers et al., 2007). Originally used to treat depression, BA has been modified to meet the needs of a variety of populations, from veterans with posttraumatic stress to people with chronic pain (Cano-García et al., 2017; Jakupcak et al., 2006).
Although BA is acknowledged as a robust mechanism of change in rehabilitative interventions (Wallbridge et al., 2008), its application to parent training is innovative. There are four main elements of BA: goal setting, skill training, activity scheduling, and activity monitoring (Kanter et al., 2010). These elements provide a structure to systematically alter family routines and promote child health every day.
We selected child meals as a practical venue to test the BA approach because of their repetitive and scheduled nature. Mealtime friction often results when young children will accept only a narrow range of foods (Jacobi et al., 2003). Physicians frequently recommend early intervention services for families who are concerned about their child’s limited dietary variety. These children fall under the umbrella diagnosis of avoidant, restrictive, food intake disorder, which covers a wide range of clinical feeding issues (American Psychiatric Association, 2013). Young children who avoid foods because of sensory characteristics are often described as having sensory food aversions (SFA; Bryant-Waugh & Kreipe, 2012). Children with SFA usually eat alone (Chatoor, 2009), which limits opportunities to interact with positive role models that could shape mealtime behaviors (Cruwys et al., 2015). Current therapist-led interventions have improved acceptance of specific foods but have failed to increase overall dietary variety (Marshall et al., 2015).
The purpose of this study was to examine the feasibility of a BA approach to train parents to alter the mealtime routines of children with SFA. Specifically, this study aimed to describe parental adherence to and acceptance of the novel intervention Promoting Routines of Exploration and Play During Mealtime (Mealtime PREP; Caldwell, 2017). We predicted that application of this innovative approach to parent training would create opportunities to incorporate treatment strategies daily when it matters most, during mealtimes. By incrementally introducing treatment strategies, we anticipated that parents would build confidence to deliver a complex intervention while gradually increasing their skills.
Method
We used a nonprobability, convenience-sampling method to recruit participants through countywide early intervention providers, primary care physicians, and social media advertisements. We obtained informed consent from parents for participation (self and child) in the study using approved institutional review board procedures. Inclusion criteria were (1) at least one parent fluent in English and able to read English at the sixth-grade level to follow written and verbal protocol instructions, (2) child aged 18–36 mo, and (3) child meeting all four criteria of SFA as determined by a licensed occupational therapist with more than 8 yr of clinical experience in pediatrics (this study’s principal investigator, Angela R. Caldwell; hereinafter, the occupational therapist). The four criteria of SFA are
Consistently refuses to eat specific foods with specific tastes and textures or smells,
Onset of food refusal occurs during the introduction of a novel type of food,
Child eats without difficulty when offered preferred foods, and
Food refusal leads to nutritional deficiencies or an oral–motor delay (Zero to Three, 2005).
The occupational therapist confirmed at least moderate risk of nutritional deficiency using established cutoffs on the Nutrition Screening Tool for Every Preschooler–Toddler version (Randall Simpson et al., 2008). We excluded children currently receiving occupational therapy services for feeding issues.
We used a single-case experimental design with multiple replications to collect rich data to inform modification of this innovative approach. Because carryover of effects was not only expected but also desired, our study consisted of three phases: baseline, parent training, and family autonomy. Each phase consisted of 10 video-recorded meals completed within a 2-wk period. During baseline, parents recorded typical child mealtimes. During the parent-training phase, the occupational therapist led four parent-training sessions, using the principles of BA to facilitate behavior change and implementation of new routines. Parents recorded meals as they practiced incorporating treatment strategies, one at a time. Therapist support was withdrawn during the family autonomy phase, and parents continued to video record new mealtime routines and deliver treatment strategies independently.
Intervention
The occupational therapist led all parent-training sessions in the home of each participant. During the first session, the therapist and parents collaborated to categorize commonly offered foods as either preferred or targeted. Preferred foods are those that the child accepts most of the time, whereas targeted foods are those that the child refuses immediately or after the first bite. Parents were instructed to offer at least one preferred and one targeted food per meal and to refrain from offering food in the hour directly before mealtime. Parents were also asked to refrain from using the television or cell phones during meals.
Mealtime PREP is a two-pronged intervention that promotes behavior change in the parent participant and the child participant. Because parents play a primary role in determining a young child’s food options and establishing a mealtime environment, changing the way they organize mealtimes is necessary to achieve successful feeding outcomes. Mealtime PREP provides a framework to train parents to embed strategies into scheduled family meals.
Parent Experience.
Each Mealtime PREP parent-training session included the following BA elements:
Goal setting. Initially, the parents and occupational therapist collaborated to formulate an overarching functional goal. They also determined a unique goal each session for parents to practice incorporating new skills into mealtimes.
Skill training. During each session, parents learned to deliver a new intervention component (family meals, positive reinforcement, and food exploration and play). The occupational therapist provided feedback as appropriate.
Activity scheduling. The parents scheduled meals over the next 3–4 days to practice.
Activity monitoring. Parents video recorded scheduled meals and kept a daily log of foods offered during each recorded meal.
Consistent with BA, parents learned to deliver one intervention component at a time to provide opportunities for success before adding complexity (Figure 1).
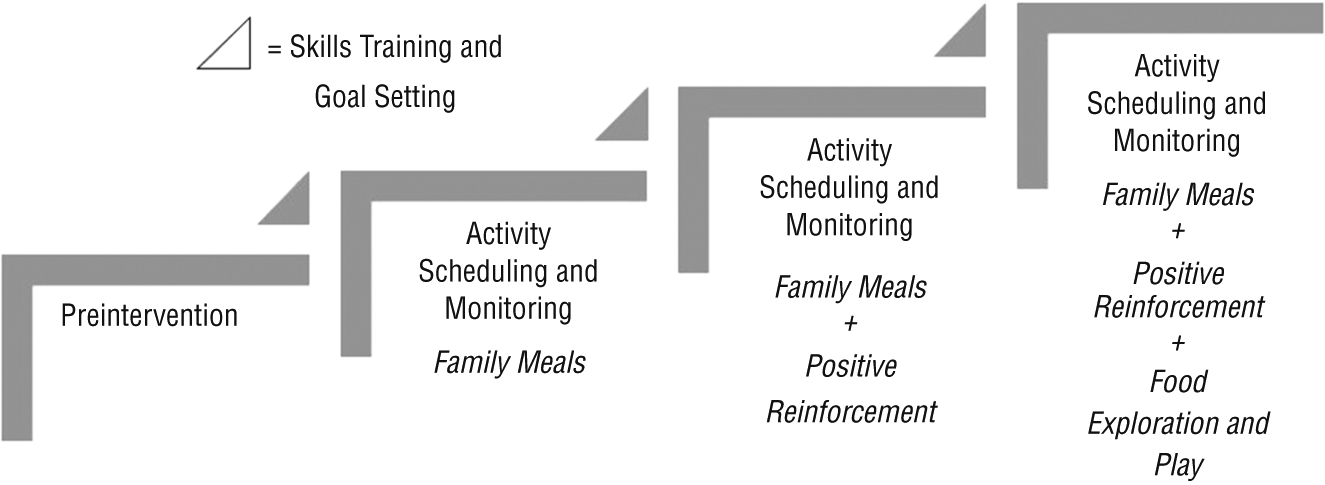
A behavioral activation approach to parent training.
During each parent-training session, the occupational therapist and parents set a realistic goal to alter mealtime routines. Though we anticipated that each family would achieve this goal and create another at the following session, the flexibility of single-case experimental design allowed families to progress through goals at their own pace. Parent training included direct instruction, discussion, written education, demonstration, and practice with immediate and delayed verbal feedback. When practice in the presence of the therapist was not possible, feedback was provided based on parent report. During the fourth session, the therapist reviewed all intervention components and brainstormed with the family to overcome potential barriers. For consistency, the therapist led all sessions and used workbook-style written education and a daily checklist to guide intervention. Each parent-training module was designed to last 1 hr.
Child Experience.
During Mealtime PREP, children participated in mealtimes enriched with the active ingredients of family meals, positive reinforcement, and repeated exposure through food exploration and play. Parents embedded these intervention components into their routine one at a time, in parallel with parent-training sessions. In other words, initially, social modeling during a new family mealtime routine was the only intervention component incorporated into child meals. Once the parent completed this routine, he or she learned to integrate positive reinforcement into the newly established family mealtime. Finally, parents learned to incorporate food exploration and play.
The parents and occupational therapist developed a structured family mealtime in concert to promote interaction with food in a predictable environment. We customized each routine to meet the unique needs of the family. All routines included a predictable schedule of events for a family-style meal (i.e., food placed within sight in community serving bowls), active child participation in food preparation or cleanup, and specified activities to signal the beginning and end of the meal. When a child refused to self-serve a food onto his or her plate, the therapist introduced the learning plate technique, developed by Toomey (2013). This technique gave the child the option to serve a portion onto a community plate (learning plate) in the middle of the table. The learning plate provided an opportunity for the parent to teach his or her child about the size, shape, color, and texture of the food.
We managed child mealtime behaviors using positive reinforcement, the concept that behavior is reinforced by consequences that are rewarding (Skinner, 1938). Positive reinforcement is effective at improving feeding outcomes in children (Horne et al., 2004). We trained parents to reinforce all food acceptance and appropriate mealtime behavior with verbal praise, smiling, and eye contact. We also trained parents to redirect inappropriate behaviors to acceptable alternatives and reinforce this alternative behavior. For example, if a child threw food during meals, the parent would redirect him or her to push the food away or put it in a scrap bowl instead. If the child chose to complete this alternative behavior, he or she received positive reinforcement. Parents were instructed to avoid negative language, punishment, and threats.
Repeated exposure is effective at improving food acceptance in children (Cooke, 2007). We incorporated repeated exposure into our intervention using food exploration and play. In typical children, availability of and exposure to a wide variety of foods are important for building healthy eating patterns (Couch et al., 2014). Children with SFA may respond better to a modified exposure plan that gradually increases the intensity of experiences with new or refused foods. Systematic graded exposure is a common tool used by occupational therapy practitioners to increase a child’s ability to interact with food (e.g., from exposure across the table to exposure passing a serving dish to exposure on a plate; Toomey, 2010). We trained parents to increase interaction with food gradually, through exploration of sensory characteristics and play to facilitate positive, child-initiated food acceptance. We provided a list to parents of different ways to interact with food and the relative intensity of each type of exposure (Toomey, 2010).
Primary Feasibility Measures
Parent-led intervention feasibility was determined by our ability to collect data in the home, adherence to intervention protocol, and intervention acceptance. For each of these measures, we set a feasibility benchmark a priori to help us decide whether the Mealtime PREP intervention package was feasible and acceptable for children with SFA and their parents.
Ability to collect data in the home was calculated as the number of video-recorded child meals per phase that we coded for fidelity. We instructed parents to record one child meal per day during each phase. We set the following benchmark: “Each parent participant will record ≥8 child mealtime sessions each phase with sufficient clarity for coding.”
Intervention adherence was determined using a parental Fidelity Checklist, developed by the study authors to reflect the main concepts of each parent-mediated active ingredient. The treating occupational therapist (64%), a trained occupational therapy graduate student (26%), or both raters (10%) completed Fidelity Checklists through video review of child meals. The Fidelity Checklist was refined for reliability after both raters coded five meals and compared results. Revisions improved clarity and eliminated repetition of overlapping concepts. The two raters were able to come to a consensus for all items on the revised Fidelity Checklist for all five initial videos. One video per phase was randomly selected (using a random number generator) to be coded by both raters to determine interrater reliability. We set the following benchmark: “Parent participants will adhere to 75% of learned intervention techniques during the family autonomy phase.”
We assessed intervention acceptance using the Treatment Acceptability Questionnaire (TAQ) after the parent-training and family autonomy phases. The TAQ is an adapted version of the Abbreviated Acceptability Rating Profile (Tarnowski & Simonian, 1992) that was modified for improved applicability to parents (as opposed to educators). The TAQ has good internal (α = .97) and construct validity (Krain et al., 2005). Higher scores on the TAQ signify better intervention acceptance. We set the following benchmark for acceptability: “Parents will rate the Mealtime PREP as >28/48 to signify an acceptable treatment (Tarnowski & Simonian, 1992).”
Secondary Feasibility Measures
We assessed occupational therapist–led intervention feasibility as the number and duration of each parent-training session. We also collected feasibility data on recruitment and duration of child meals. To evaluate whether the parent-mediated strategies were changing child mealtime behaviors, parents completed the Behavioral Pediatrics Feeding Assessment Scale (BPFAS; Crist & Napier-Phillips, 2001) at baseline and at study completion. This 35-item scale is a valid measure of child feeding issues (Crist & Napier-Phillips, 2001). The BPFAS has adequate sensitivity and specificity to discriminate between children with and without clinical feeding disorders (Dovey et al., 2013).
Data Analysis
We first described our ability to collect data in the home, parental intervention adherence, and treatment acceptance using raw scores, percentages, and frequencies, respectively. The intraclass correlation coefficient (ICC) was then calculated to determine the interrater reliability of the parental Fidelity Checklist. All statistical procedures were completed using IBM SPSS Statistics (Version 23; IBM Corp., Armonk, NY). We also summarized changes in child mealtime behavior using established clinical cutoffs.
Results
We recruited and screened 13 families over a 7-mo period. One family did not meet inclusion criteria (child did not demonstrate an oral–motor delay or risk of nutritional deficiency), and one family decided not to participate after eligibility was confirmed. Therefore, 11 children, ranging in age from 19 to 35 mo, and their parents participated. All 11 participant families completed the study. The children in our sample were White (100%), resided with both parents (100%), and were nearly equally distributed between genders (64% male). About half of the child participants demonstrated an oral–motor delay (55%), and most child participants were at risk for nutritional deficiency (73%). The parents in our sample were highly educated, with 95% having a bachelor’s degree or higher, and household income ranged from middle to high (55% earning >$100,000 annually; Table 1).
Child Participant Demographics (N = 11)
Note. Risk of nutritional deficiency was determined using the Nutrition Screening Test for Every Preschooler–Toddler version. Oral–motor delay was determined by an occupational therapist using established oral–motor milestones.
Primary Feasibility Measures
The primary feasibility measures were ability to collect data on child meals in the home, intervention adherence, and intervention acceptance. Table 2 lists descriptive statistics for each.
Descriptive Statistics of Intervention Feasibility (N = 11)
Note. M = mean; Meal PREP = Promoting Routines of Exploration and Play During Mealtime; SD = standard deviation; TAQ = Treatment Acceptability Questionnaire. — = not applicable. Feasibility benchmarks set a priori.
Benchmark: Each parent participant will record ≥8 child meal sessions/phase. bBenchmark: Parent participants will adhere to 75% of techniques in the family autonomy phase. Fidelity Checklist used to assess percent of techniques used per meal. cBenchmark: Parent participants will score the Mealtime PREP >28/48. TAQ used to assess score for intervention acceptance.
Ability to Collect Data in the Home.
On average, parents recorded approximately 10 mealtime sessions per phase. This number surpassed our target of 8 mealtime sessions per phase. Every family met this benchmark.
Intervention Adherence.
On average, parents used approximately 64% of learned techniques during the family autonomy phase. Although this number did not meet our benchmark of 75%, it was an increase of 36 percentage points from baseline, when parental adherence to intervention strategies was only 28%. This increase equates to parents using, on average, three more intervention strategies after parent training than they did at baseline. Interrater reliability of parental adherence was excellent (Hallgren, 2012), with an ICC of 0.791 (95% confidence interval [0.575, 0.897]).
Intervention Acceptance.
At study end, parents rated intervention acceptance at 43/48 points on average, which surpassed our intervention acceptability benchmark of 28/48. Individual intervention acceptance scores ranged from 26 to 48.
Secondary Feasibility Measures
Each parent participant completed all four parent-training sessions and progressed as expected through all three parent-training modules (family meals, positive reinforcement, and food exploration and play). Six families had more than one caregiver participate in parent training. On average, each session lasted 63 min (range = 40–80 min). The session on family meals tended to be the longest (mean = 71 min), and the session on positive reinforcement was shorter (mean = 52 min). Average mealtime length was similar for both intervention phases: approximately 18 min per meal (range = 2 min 31 s to 52 min 12 s).
BPFAS scores decreased from an average baseline score of 82 to an average score of 71 at the end of the study. Three child participants demonstrated improvement in behavior sufficient to shift from the categorization of a clinical feeding disorder at baseline to the categorization of typical feeding behaviors at study end. In addition, all 6 participants that exceeded the clinical cutoff for a feeding disorder based on the number of parent-identified problems shifted below this cutoff after the Mealtime PREP intervention.
Discussion
Our data suggest that it is feasible to deliver the Mealtime PREP intervention in the home to a sample of children with SFA and their parents. In addition, it is feasible to collect data on child feeding outcomes within the natural context of daily meals. Each family met our feasibility benchmark of video recording at least 8/10 planned child meal sessions in each phase. The occupational therapist completed all parent training within the home environment and provided feedback on intervention delivery to the parent participants of 5 children during actual family meals. Providing intervention and feedback in the natural context, during mealtimes, allows the therapist to observe and troubleshoot real-world barriers to intervention delivery. Similar benefits associated with home-based intervention and direct observation have been reported in previous parent-training intervention studies (Crockett et al., 2007; McIntyre & Abbeduto, 2008). Parent participants were open to this approach and rated the Mealtime PREP intervention package as an acceptable treatment option.
Although we did not meet the parental intervention adherence benchmark, our data suggest that mealtimes were different because parents, on average, were using more mealtime intervention strategies during the parent-training and family autonomy phases than at baseline. Each family demonstrated increased adherence to the Mealtime PREP techniques after parent training was initiated. These fidelity data led to several hypotheses regarding best practice in parent-training methods. Slight decreases in adherence observed during the family autonomy phase, compared with the parent-training phase, suggest that frequent contact with a therapist may be an important component to maintaining newly established routines. Research is needed to examine methods to improve adherence during the follow-up period, such as a booster session, increased training, or more opportunities for feedback. Identifying such methods may be of particular importance when working with families with demographic factors associated with nonadherence, such as single parenthood, low income, and young parental age (Gearing et al., 2014). Although it was not a significant change, this slight decline in adherence may foreshadow limited carryover of techniques over time. Longitudinal surveillance could elucidate whether certain intervention components assimilate into daily routines long term and others fade over time.
We intentionally decided not to structure the length of mealtimes during this study in an effort to gain a better understanding of how the Mealtime PREP intervention meshed into different routines. We learned that there is great variability in the length of mealtimes both within and between families. Typical mealtimes of toddlers are, on average, 20 min long (Reau et al., 1996), and although our average mealtime during intervention was just under this time (18 min), we observed meals that ranged in length from 2 to 52 min. Future research is necessary to determine whether outcomes are associated with mealtime duration.
Study Limitations
Our study is not without limitations. Foremost, we are unable to generalize the results of this study to the population because of the small sample size. Additionally, prior research has highlighted the unique barriers to behavior change that families in both rural and urban neighborhoods face (Kottyan et al., 2014; Lim & Janicke, 2013). Future studies should prioritize increasing not only the sample but also the diversity of participants because the feasibility of training parents in the home environment may vary on the basis of sociodemographic characteristics. Moreover, it would be beneficial to assess parental competence in addition to adherence to the intervention. Measuring each parent’s level of competence would provide better insight into the potency of this approach to parent training. We also recognize a risk of response bias on parent-report measures from parent participants desiring to observe changes because of participation in a research study.
Implications for Occupational Therapy Practice
Clinical implications gleaned from this research may shift the way occupational therapy practitioners frame parent and caregiver training to alter the daily routines of clients. They include
It is feasible for occupational therapy practitioners to use elements of BA to organize and deliver components of complex interventions.
By using an incremental approach to parent or caregiver training, occupational therapy practitioners may be able to alter daily routines in the home environments of the families they serve.
Conclusion
The results of our feasibility study suggest that the Mealtime PREP feeding intervention is feasible and acceptable to parents of children with SFA. Our study was innovative because we used a novel approach to parent training and collected data on parental intervention delivery in the home, without the presence of research personnel. Clinically relevant shifts in child mealtime behavior signal that Mealtime PREP is a promising treatment to improve child feeding outcomes. Larger scale trials are warranted to determine the effectiveness of the Mealtime PREP intervention for children with limited dietary variety. If successful in children with SFA, this intervention could potentially promote improved nutrition and minimize risks associated with limited dietary variety among children in general. Research is needed to determine the optimal frequency and duration of occupational therapy services to promote healthy, long-term changes in individual and family routines.
Footnotes
Acknowledgments
The authors acknowledge Kaitlin Debar for her dedicated assistance with video review and coding of data for analysis. We also acknowledge the School of Health and Rehabilitation Sciences Dean’s Research Development Fund and Department of Occupational Therapy at the University of Pittsburgh for funding this project. This study is registered under Identifier NCT03138551 at ![]() .
.