
Abstract
Occupational therapists have an established and important role in helping people work while living with an illness or a disability. Although workplace accommodations and rehabilitation efforts can extend paid work for workers with progressive health conditions, the reality is that these populations often cease work earlier in the life trajectory than expected. Evidence suggests that transitioning out of paid work is difficult for people with disabilities. For example, factors such as poor health, low income, and involuntary retirement put people with multiple sclerosis at risk for poor adjustment. Given society’s emphasis on paid work, the transition to unpaid work has received little attention. Occupational therapy practitioners are well positioned to contribute to enhancing the quality of life of people in work-cessation transitions who are not of traditional retirement age.
The concepts of adaptation and transition are central to the profession of occupational therapy. Occupational adaptation is “the extent to which persons are able to develop, change in response to challenges, or otherwise achieve a state of well-being through what they do” (Kielhofner, 2008, p. 106), and it occurs throughout the lifespan, encompassing transitions such as ceasing paid work. Occupational adaptation is embedded in occupation models (Kielhofner, 2008; Townsend & Polatajko, 2007), and the experience of transition has been a focus of research by occupational therapists for the past 15 yr (Crider et al., 2014). In regard to work transitions, occupational therapy practitioners have an established role in helping people adapt to working while living with illness or disability and facilitating transitions back to work after illness (Ellexson & Larson, 2011; Page & Braveman, 2012). However, given society’s emphasis on the importance of paid work, the transition and adaptation out of paid work for people with progressive health conditions has received little attention.
Retirement is defined as the “exit from the [labor] force taken by individuals after middle age, and taken with the intention of reduced psychological commitment to work thereafter” (Feldman, 1994, p. 287). The transition to retirement can be difficult given that it requires a shift in routines and daily social patterns, but after a period of adjustment most people maintain or have a slight temporary increase in their life satisfaction after retirement (Wang et al., 2011). Occupational therapists have contributed to knowledge of typical retirement by identifying that retirement influences one’s identity, routines, and roles and that adaptation to this new life stage requires engagement in occupations that have specific qualities (e.g., having an element of “work” and involvement in a community; Jonsson, 2011; Pettican & Prior, 2011).
Disability retirement, defined as work cessation that occurs earlier than expected in the life course because of a chronic health issue, presents greater challenges and is more likely to be associated with poor adjustment to retirement (Denton et al., 2013). At some point in the trajectory of a progressive condition, continuing to work can erode one’s quality of life (Johnson et al., 2004), but there is a dearth of literature with an occupation lens to guide practice on supporting early work cessation at individual and societal levels.
Regardless of workplace accommodations and rehabilitation efforts, the reality is that many people with progressive conditions, such as multiple sclerosis (MS), need to cease paid work earlier in the life trajectory than expected. Given the lack of literature on how to assist people with progressive conditions in the transition to nonpaid work roles, this article provides a springboard for discussion of research and practice about adjustment to early retirement for this population. I first draw on a multidisciplinary literature base to describe typical adjustment to retirement; I then discuss the difference between adjustment to disability-related retirement and adjustment to typical retirement. Last, I discuss models that exist to support occupational therapy engagement in this area of practice.
Adjustment to Retirement
Typical Adjustment to Retirement
Wang and colleagues (2011) proposed that adjustment to retirement is a longitudinal process that incorporates both the transition from work and the wellness trajectory that follows retirement. They identified three longitudinal patterns of retirement adjustment: Some people maintain a high level of well-being, some have a temporary decrease in well-being that returns to baseline over time, and a third group has a temporary increase in well-being that returns to baseline over time.
The factors that contribute to retirement adjustment and well-being have been well researched and were summarized in a systematic review by Barbosa et al. (2016). Their findings suggest that health and wealth are two of the strongest predictors of positive adjustment to retirement. Also found to be highly associated with positive adjustment were psychological health and personality attributes (e.g., optimism, an internal locus of control, humor, and extraversion), involvement and competence in leisure activities, social integration other than a marital relationship, and perceived voluntary retirement (i.e., the decision to retire is internal to the retiree). Other factors they found that are believed to contribute positively to retirement adjustment but require more study are preparation for retirement; being married; involvement in volunteer work; availability of community resources; maintaining a professional identity; engaging in physical activity; level of spirituality; and characteristics of the preretirement job, such as prestige and stability.
Qualitative research provides insight into the complexity of the psychological adjustment to retirement. Whereas retirees often welcome the lack of structure, routine, and external demands to be productive, they also struggle with how best to use their time (Jonsson, 2011). Retirees can experience a loss of meaning in their lives as they consider “Who am I now?” and “What is my purpose?” (van den Hoonaard, 2015, p. 54). Van den Hoonard (2015) proposed that the transition to retirement is challenging because the retiree is moving from a socially desirable space (a productive member of society) to a socially undesirable space (an unproductive member of society).
Adjustment to Disability Retirement
Research on adjustment to retirement for people with disabilities is much more limited. However, scholars have established that people with a disability are 8 times more likely to perceive their retirement as involuntary (Denton et al., 2013); that is, they perceive external pressure to cease work through direct (e.g., being asked to leave the job) or indirect (e.g., the employer does not accommodate the employee) means (Bradley et al., 2004). The link between disability and involuntary retirement is concerning, because involuntary retirement is strongly associated with poor transition factors, including economic disadvantage (Denton et al., 2013; Noone et al., 2013) and decreased social, psychological, and daily activity outcomes (Noone et al., 2013).
Although qualitative literature on disability retirement is scarce, two studies found that unfulfilled work roles contributed to a poor transition to retirement (Bradley et al., 2004; Markle et al., 2015). Relinquishing one’s work identity in midlife can be distressing, because this is a time of life during which an individual’s self-concept is directly related to work roles. Moreover, the job loss highlights the impact that the disability is having on the worker’s life, requiring two related psychological adaptations: (1) giving up a “nondisabled identity” and (2) relinquishing a “work identity” (Bradley et al., 2004, p. 251). People with disabilities also have increased challenges with replacing work roles. Whereas people who retire at a typical age tend to increase the amount of time they spend on moderately intense activity and exercise, those who retire because of disability have low levels of participation in leisure activities (Lahti et al., 2011).
The little evidence that exists on adapting to disability retirement suggests that two factors can positively affect the transition. One factor is the belief that the work cessation is resulting in improved health (van Solinge & Henkens, 2007). The other factor involves financial and social planning for retirement in multiple spheres, just as for typical retirement (Noone et al., 2013). Occupational therapy practitioners who focus their efforts only on helping clients maintain work roles rather than balance the continuation of work with preparations for leaving the work force could be contributing to clients’ poor adjustment to nonwork roles.
Example: Multiple Sclerosis
People living with MS experience the highest unemployment rates among people living with chronic health conditions. High unemployment among people with MS occurs because the diagnosis is typically received mid-career and because multiple systemic, physical, and cognitive symptoms are associated with the condition (Sweetland et al., 2012). Compounding the challenges of ceasing work early in the life trajectory are health condition–related psychological, physical, and cognitive factors.
The psychology literature has demonstrated that the psychological adjustment processes for people with MS are more likely to be maladaptive than those of the general population (Dennison et al., 2009). People with MS more often adopt maladaptive, emotion-oriented coping (e.g., wishful thinking, detachment) instead of problem-solving coping styles. In addition, people with MS tend to have lower self-esteem than the general population, regardless of their health and employment status (McCabe & DiBattista, 2004). These features parallel factors identified to be strongly related to poorer adjustment to retirement, such as high levels of perceived stress, appraisal of stressors as a threat (rather than as a challenge or controllable), and use of emotion-focused rather than problem-solving coping strategies (Dennison et al., 2009). Finally, approximately 50% of the population with MS experience cognitive impairment that can interfere with efforts to adopt new coping strategies (Chiaravalloti & DeLuca, 2008).
Qualitative work has highlighted that occupational adaptation is challenging for people with MS (Cahill et al., 2010; Lexell et al., 2009). Participants in these studies were able to maintain leisure occupational identity if they could find ways to adapt or maintain their current interests or develop new interests that accommodated their symptoms. However, many participants experienced a reduction in activities because of person factors and environmental barriers that ultimately affected their quality of life. The unpredictable nature of the condition made adaptation difficult for all the participants, but participants with the relapsing–remitting form of MS had more success with occupational adaption than did those with progressive forms, because their occupational disruptions were temporary (Cahill et al., 2010). Although home, work, and leisure roles were all important for the maintenance of occupational identity, work and caregiving roles were more difficult to adapt in a satisfactory way (Lexell et al., 2009).
Retirement Adjustment Models: Working Toward Occupation-Based Models
Many theories have been applied to the concept of retirement adjustment. Activity theory is supported by findings that engaging in part-time work, volunteer activities, and a variety of leisure activities can improve retirement adjustment (Nimrod, 2007). Continuity theory helps us understand why maintaining a link between pre- and postretirement life promoted adjustment to retirement for men living in rural areas (Wiseman & Whiteford, 2009). Role theory helps explain why higher role complexity acts as a buffer to job loss, because retirees who miss their job can maintain a high level of satisfaction from other identity domains (Teuscher, 2010). Moreover, a resource perspective can be used to understand why retirees with strong internal resources can redefine or expand their roles and activities after ceasing work (Carter & Cook, 1995). Although these theories are useful for understanding the transition to retirement, none is sufficiently robust to enable an understanding of the whole phenomenon (Wang et al., 2011).
To address the need for increased model complexity to explain retirement transition, Wang and colleagues (2011) introduced a resource-based dynamic longitudinal perspective, an evidence-based model positing that six types of resources—physical, cognitive, motivational, social, financial, and emotional—contribute to individual adjustment. With a change in resources (due to personal or institutional factors) comes a change in adjustment levels. This model provides a framework for the hypothesis that ceasing work early in the life trajectory because of a disability would negatively affect retirement adjustment for people with progressive health conditions given that they likely already have strained resources, such as physical and cognitive symptoms (Sweetland et al., 2012), a poor financial situation (Pfleger et al., 2010), poor emotional coping strategies (Dennison et al., 2009), and strained social relationships (Pakenham & Samios, 2013).
Similar to occupation-based theories, such as the Model of Human Occupational Performance (MOHO; Kielhofner, 2008) and the Canadian Model of Occupational Performance and Engagement (CMOP–E; Townsend & Polatajko, 2007), Wang et al.’s (2011) model considers both person- and environment-related resources. However, a side-by-side comparison of the resource-based longitudinal perspective, the MOHO, and the CMOP–E with regard to the factors that contribute to successful retirement adjustment (Figure 1) highlights the lack of occupation focus in the resource-based longitudinal perspective. Occupational therapy practitioners need to consider combining these models in order to examine the important relationship between occupation and the transition to retirement and how person- and environment-level factors moderate occupation factors in that context.
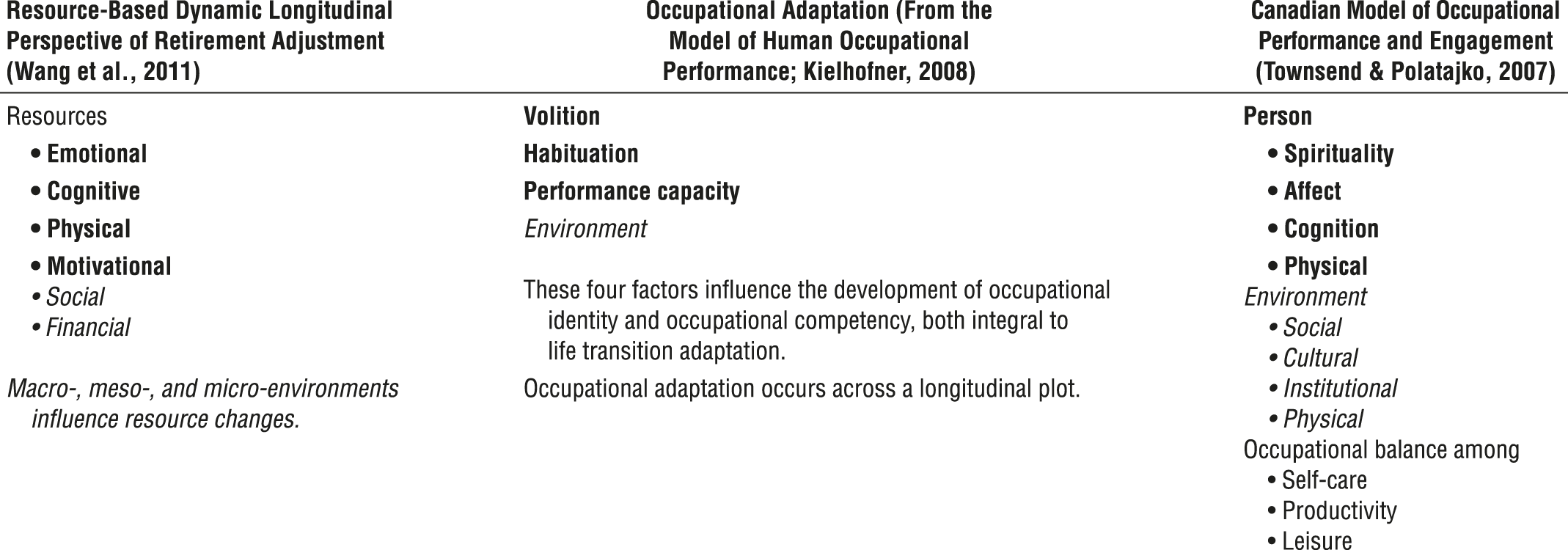
Factors contributing to successful retirement transition according to three theoretical perspectives.
Implications for Occupational Therapy Practice and Research
There is still much to learn about the work-to-retirement transition from an occupational perspective (Eagers et al., 2016). Considering this transition in the context of progressive health conditions is particularly important because of the many individual and environmental risk factors for poor adjustment to retirement in populations with such conditions.
Until more specific evidence on early work cessation for people with progressive conditions is available, occupational therapy clinicians can be guided by research on general and involuntary retirement. They can talk to their clients about planning ahead for work cessation, help their clients find ways to meaningfully participate in retirement activities, and support the maintenance of social relationships outside of the immediate family. Occupational therapists are well positioned to ensure success with planning and carrying out transition plans because of our unique skills in tailoring education and support to the individual needs of people with illness or disability. Finally, practitioners should consider working with employers to provide a satisfactory work-to-nonwork transition that reduces the likelihood of perceived involuntary work cessation.
Important areas for future research include determining the retirement adjustment patterns in populations that typically need to cease work earlier than anticipated and the factors that contribute to these patterns. Wang et al.’s (2011) resource-based dynamic longitudinal perspective complements occupational therapy models, and the two should be integrated to develop a multifactorial occupational view of retirement adjustment. At a more macro level, exploring societal narrative attitudes and values surrounding nonpaid work is important in addressing stigma toward nonpaid work roles that may be stifling clients’ ability to find self-fulfillment in nonpaid work roles (Jonsson, 2011).
Opportunities exist for the occupational therapy community to advocate for policy that promotes positive adjustment to retirement for people with progressive health conditions. Incentives should be provided for employers to encourage retirement planning, allow for gradual work cessation without pensions being penalized, and provide retirement support services that extend beyond the work cessation date (Noone et al., 2013). Policy that supports barrier-free leisure and volunteer opportunities would promote engagement in meaningful activity (Jonsson et al., 2001).
Conclusion
Occupational therapy is well positioned to contribute to enhancing the quality of life of people who need to cease paid work earlier in the life trajectory than expected, with practitioners’ expertise in negotiating life transitions, promoting engagement in meaningful activity, and applying holistic models.
Footnotes
Acknowledgments
I thank the former University of Manitoba Master of Occupational Therapy independent-study students whose literature reviews on the topic of early work cessation motivated this article: Megan Barrie, Jessi-Beth McCannell, Shanna Pycko, Alix Tessler, Bency Thekkineth, Danielle Vigier, and Teresa Wong. I am grateful to Verena Menec, Joanie Sims-Gould, Leslie Johnson, and the peer reviewers for their encouragement and helpful feedback on drafts of this work. A poster related to this work, “Development of a Survey to Understand the Experience of Disability Retirement in Men With MS,” was presented at the Consortium for Multiple Sclerosis Conference in Dallas in 2013.