
Abstract
Specific learning disability (SLD) is a neurodevelopmental disorder that is diagnosed by low educational competency in early primary school years (American Psychiatric Association [APA], 2013). Even though children with SLD face different problems in everyday occupations, such as playing, self-care, and academic achievement, only academic issues have received much attention. The role of occupational therapy for these children is to facilitate participation in different occupational areas (Spitzer et al., 1998). Executive function (EF) plays an important role in relation to participation in occupations (Cramm et al., 2013; Foster & Hershey, 2011), and occupational therapy practitioners should consider EF when designing interventions for children with SLD.
Many descriptive studies (e.g., Moura et al., 2015; Varvara et al., 2014) have documented executive dysfunction among children with SLD. People with executive dysfunction may experience difficulty in managing complex occupations with dynamic task demands, such as instrumental activities of daily living and social functioning, which can result in a restriction in their life roles (Cramm et al., 2013; Foster & Hershey, 2011). Some studies have suggested that certain educational computerized tasks may help to improve EF in children with SLD (Horowitz-Kraus, 2015; Staiano et al., 2012). Moreover, activities that incorporate play may efficiently improve EF skills (Shaheen, 2014).
Play as an occupational area is characterized by self-motivation (Andersen et al., 2005), which is important in EF (Pessoa, 2009). In addition, motivation is a basic construct of the Model of Human Occupation (MOHO; Kielhofner, 2008a). This occupation-focused model, which includes several outcome measurements, is widely used by researchers (Lee, 2010). The model posits that active participation will occur when valuable occupations are done in a sociocultural context. Participation in a constant environment contributes to the development of occupational competence and identity over time; however, this process is a dynamic transaction, and any changes in a person’s internal factors (e.g., volition, habituation, performance capacity) can alter the overall process (Kielhofner, 2008b).
No study to date has investigated values and competence in all occupational areas of children with SLD; previous work has been limited to their social competence (Nowicki, 2003). In general, less attention has been paid to play activities in these children. Therefore, researchers’ knowledge about the effect of such activities on improving EF skills is limited. In this intervention study, we examined the effect of peer-play activities on EF skills of behavior regulation and metacognition and perceived occupational values and competence.
Method
Research Design
This study was a single-blinded, randomized clinical trial. The participants were randomly assigned to the intervention (n = 25) and control (n = 24) groups using random-number tables by an official who was not connected with the study. Ethical approval was obtained from the Iran University of Medical Sciences ethics committee. Parents whose children assented to participate in the research signed the written informed consent.
Participants
Forty-nine children with SLD were selected from four educational centers for SLDs through convenience sampling. The sessions were held in play therapy clinics. The inclusion criteria were as follows: ages 7–11 yr; diagnosis of SLD based on the criteria in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; APA, 2013); parents’ mental health and ability to comprehend the questionnaires the questionnaires; and lack of comorbid psychiatric disorders, except for attention deficit hyperactivity disorder (ADHD). A pilot study showed that children with comorbid ADHD who were receiving a controlled dosage of methylphenidate under the supervision of a psychiatrist could be included.
Instruments
Child Symptom Inventory–4.
The Parent Checklist of the Child Symptom Inventory–4 (CSI–4; Sprafkin et al., 2002) was used to screen for comorbid disorders. This inventory is based on the fourth edition of the DSM (APA, 1994).
Play History.
The Play History (Behnke & Fetkovich, 1984) is a semistructured interview with parents, usually used as an intervention guideline in research and clinical practice (Bryze et al., 2008). The qualitative data from the Play History interview were used to determine the children’s play abilities, interests, and experiences for planning the intervention.
Behavior Rating Inventory of Executive Function.
The Behavior Rating Inventory of Executive Function (BRIEF; Parent version; Gioia et al., 2000), which contains 86 items, is used to investigate the EF components EF in the context of the natural environment of children ages 5–18 yr. It contains two indices consisting of eight scales. The Behavior Regulation Index (BRI) includes the Inhibit, Shift, and Emotional Control scales, and the Metacognitive Index (MCI) includes the Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor scales. The sum of the indices constitutes the Global Executive Composite (GEC). The BRIEF showed good internal consistency (Cronbach’s α = .80–.90). The test–retest coefficients of the BRI, MCI, and GEC scales in the Parent version were .81, .83, and .80, respectively (Gioia et al., 2000).
Child Occupational Self-Assessment.
The Child Occupational Self-Assessment (COSA; Card Sort version; Kramer et al., 2014) is a self-report assessment that is used to measure children’s perceived competence in and values regarding their participation in everyday occupations. It includes 25 items and 2 scales (Competence and Value) and can be used with children ages 6–17 yr. The COSA’s psychometric properties provide evidence that it is a reliable assessment tool with good content, structural, and substantive validity as an outcome measure (Kramer et al., 2014).
Intervention
The intervention was prepared and approved by a MOHO specialist and five professors in the fields of occupational therapy, psychology, and cognitive neuroscience. The study was piloted with 10 children. The intervention was conducted with groups of 3–5 children. Peer-group activities are essential to help children’s skills and competence in middle childhood (Florey & Greene, 2008).Two 3-hr sessions per week for 9 wk (a total of 18 sessions) were planned for each participant group. The mean number of sessions was 17.2, and the mean length of each session for each participant was 2.75 hr.
The intervention included practice play, symbolic play, and games with rules. It contained cooperative (shared materials for individual projects) and collaborative (adherence to responsibilities and rules for joint projects) play. The adaptation and compensation approach was used to grade the complexity of activities and modify the method and materials until the children succeeded in doing them. The intervention enhanced the children’s ability to participate in group play independently by fading therapists’ leadership role (as mentioned by Solomon, 2013). The activities of early sessions were selected on the basis of the information gathered through the Play History, and their complexity was gradually increased. Some activities that were extracted from a play activities book (Rezvanfar & Pormun, 2011) were added. The sessions targeted EF components including inhibition, shifting, emotional control, working memory, initiation, planning, organization of materials, and monitoring. MOHO strategies were used as general principles of the intervention during all sessions; in addition, a MOHO construct was emphasized in both of the two weekly sessions (Table 1).
Goals of the Peer-Play Intervention
Note. In Sessions 1–12, the therapist’s role was instructor, participant, and facilitator. In Sessions 13–18, the therapist’s role was chairperson and consultant.
During the intervention, the trial therapists received constant feedback from the trial manager (a pediatric occupational therapy practitioner who designed the intervention). They held daily meetings in which they discussed the day records and closed-circuit television recordings.
The control group received no treatment during this intervention phase. This group did receive five sessions of peer-play activities after the postintervention assessment (to adhere to ethical standards).
Data Collection
The CSI–4 and Play History data were collected by the trial manager. The outcomes were measured by means of the BRIEF and COSA before and after the intervention. These measures were administered, digitally scored, and analyzed by two occupational therapy practitioners who were trained and blinded to the study design and group allocation. The intervention was delivered by two trained and experienced occupational therapy practitioners.
Statistical Analysis
The data were analyzed on an intention-to-treat basis. We examined the normal distribution of the data using the Shapiro–Wilk test. To calculate the variation in multiple dependent variables and control the covariate effects, we used multivariate analysis of covariance (MANCOVA) between the groups (Tabachnick et al., 2001). The effect sizes were calculated on the basis of partial η2 estimation that is most frequently reported when using MANCOVA. The values of .01, .06, and .14 were considered as small, medium, and large effects, respectively (D’Amico et al., 2001). The statistical analyses were conducted using IBM SPSS Statistics (Version 19; IBM Corp., Armonk, NY). The level of significance was determined as p < .05.
Results
The disposition of the sample is shown in Figure 1. The intervention group included 25 children ages 8.5 ± 1.33 yr, and the control group included 24 children ages 8.77 ± 1.03 yr. The participants were well matched on demographic characteristics, and no significant differences were found between the two groups (p > .05). The male to female ratio was 2.5 (71.4% boys and 28.5% girls). Twenty children (40.8%) had comorbid ADHD. This information is summarized in Table 2 for the two groups. Before data analysis, the assumptions of MANCOVA were examined. All data were found to be normally distributed. The bivariate distribution of the data showed a linear relationship between the dependent variables. Tolerance coefficient and variance inflation factor were in the acceptable range. The results of M-Box tests for equality of covariance matrices and Leven’s test for equality of error variance suggested homogeneity of variance assumptions. Therefore, MANCOVA was possible.
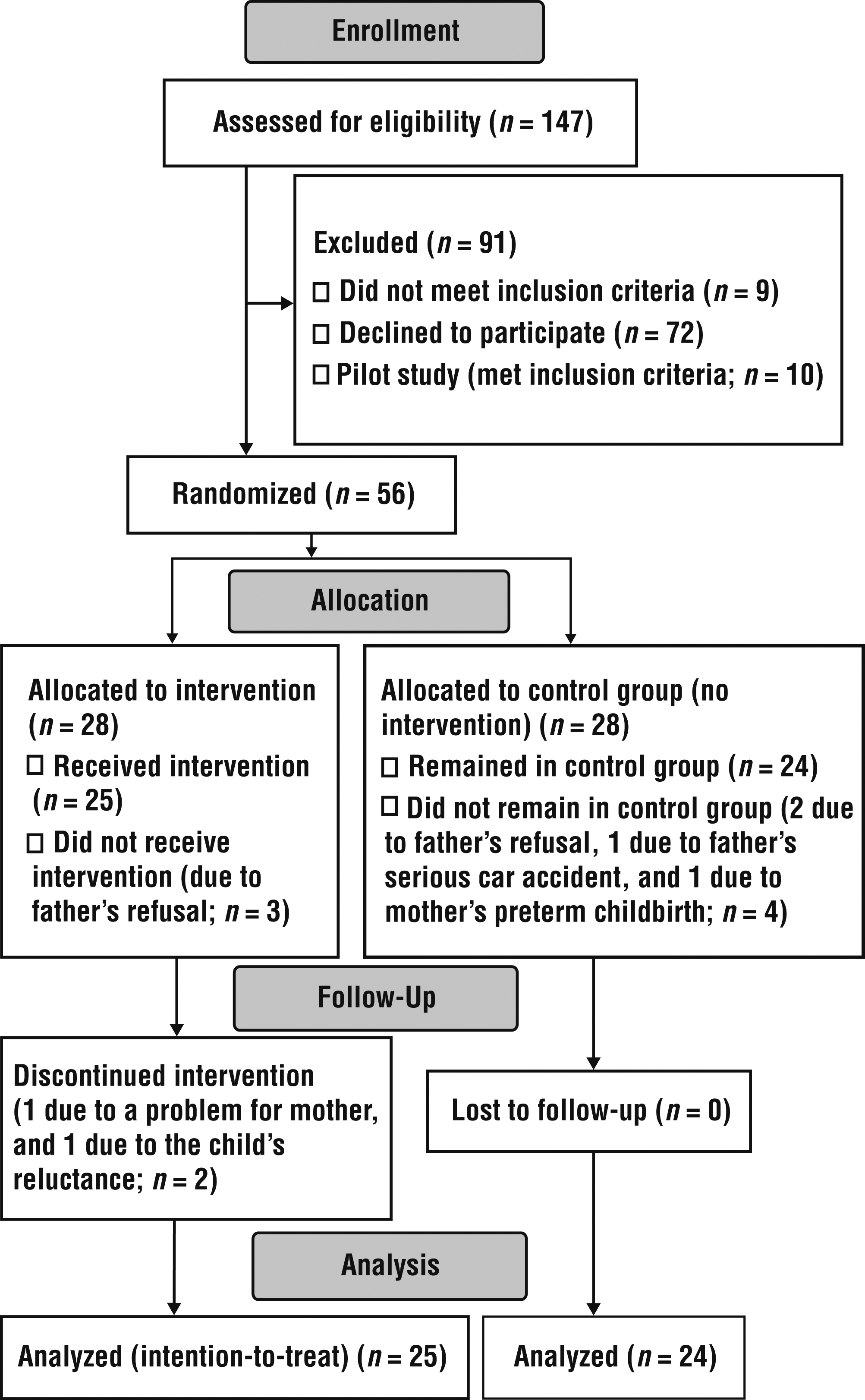
Participant flow.
Demographic Information
Means of the BRIEF indices significantly improved after the intervention. For the BRI and MCI, between-groups F(1, 45) = 11.16 and 6.24, respectively (Table 3). There was a slight change in the mean scores between the pre- and postintervention measurements in the control group (BRI = 0.16; MCI = 1.04); however, a much greater change was observed in the intervention group (BRI = 8.52; MCI = 15.32). Data analysis showed that, after controlling the pretest differences, the BRIEF profiles for both groups were significant (p < .05). The effect size was .12 for the BRI and .20 for the MCI. These are middle-to-large effects based on Cohen’s criteria (D’Amico et al., 2001).
Results of the Multivariate Analysis of Covariance Between the Groups
Note. BRIEF = Behavior Rating Inventory of Executive Function; COSA = Child Occupational Self-Assessment.
We found no statistically significant differences between the two groups (p > .05) on the COSA scales (Value and Competence). The change in Competence scale scores was greater in the intervention group, but it was not significant.
Discussion
In this study, we examined the effect of participation in peer-play activities on EF skills and perceived occupational values and competence for children with SLD. Findings showed that participation in peer play increased EF; however, it had no impact on the self-assessment of occupational values and competence of children with SLD.
In previous literature, researchers have not discussed perceived occupational values and competence as an intervention outcome measure in children. Pálsdóttir et al.’s (2014) study showed a change in occupational values in adults with disability. In their study, they used two quantitative tools and a qualitative interview for measuring the values. The duration of their intervention was 3 times longer than that of the current study. Hence, the results of the current study may be enhanced by increasing the intervention duration and using more than one assessment instrument. Presumably, it is difficult to change and measure values because they have already been absorbed from the environment during a lifetime.
A significant change in EF scores indicated that parents perceived that their children’s competence in performance of occupations increased; however, on the basis of the COSA, the children did not perceive this change. Concurrent with this assessment, Nobakht and Yazdani (2016) mentioned that children’s perception of their competence often differed from that of their parents. Note that children with SLD have deficits in metacognition abilities such as prediction and evaluation (cognitive estimation; Desoete & Roeyers, 2002); hence, the COSA, which involves mental judgment processes, may not have been a sensitive enough outcome measure for this study. In addition, even in children who have no comorbid psychiatric disorder, comorbid symptoms of SLD, such as anxiety and inattention, may have affected both the intervention and the administration of the COSA. Children with comorbid ADHD were unable to sustain focus and were disruptive in the final sessions (the therapists’ leadership role was minimal for habit training of peer play). Consistent with this, Murad et al. (2013) showed that negative emotional state had an inverse relationship with self-perception of occupational competence in administrating the Occupational Self-Assessment (the Adult version of the COSA).
According to the dynamic principles of human occupation in MOHO (Kielhofner, 2008b), developing a new occupational pattern requires support and constant repetition in the natural living environment. In the current study, the intervention did not occur in the children’s natural living environment. This limitation can influence the interpretation of the data collected by the COSA and shows that providing the intervention in the treatment environment was not sufficient to achieve occupational outcomes.
As we mentioned in our previous article (Esmaili et al., 2017), the findings of this study indicated that the peer-play intervention improved the metacognitive and behavior regulation skills of EF. Compared with the findings of the meta-analysis conducted by Swanson and Hoskyn (1998) of clinical trials in children with SLD, the effect size for our intervention was larger than that for other interventions on similar outcomes such as metacognition, problem solving, and social skills. Other interventions focusing on EF in SLD (Horowitz-Kraus, 2015; Staiano et al., 2012) have usually been structured and without meaning. In our intervention, the activities took the form of meaningful and purposeful cultural play activities and provided maximum emotional engagement.
Another strength of this study was that because of the length of the intervention, the posttest was done 2 wk after the end of the treatment to ensure that the findings were the result of the cumulative effect of all sessions. A similar study by Staiano et al. (2012) showed increased EF in adolescents without disorders who used Kinect video games. However, because their posttest was conducted immediately after the latest treatment session, the findings could have been influenced by result of the final sessions.
In this study, we used the BRIEF to explore parents’ perspectives and children’s outcomes in everyday life and in various activities. A significant change on this instrument indicated that the EF skills were transferred to the life situations. Consistent with the opinion of Shaheen (2014), we believe that a play-based treatment with generalization and long-term effects can be widely used in the clinical settings, especially with children with SLD.
Limitations
Some consent forms were completed only by the mother; in a few cases, the father refused to cooperate when he was informed of the project conditions. That is the main reason why the sample size decreased after initial randomization. To address this issue, we included MANCOVA and an intention-to-treat approach in our data analysis. Another limitation is that the project was carried out during the school holidays, and the researchers did not have the chance to gather the BRIEF data from the teachers.
Further Research
It is suggested that, in addition to the control group with no intervention, a group with a nonplay approach should be compared with the play intervention group.
Implications for Occupational Therapy Practice
The results of this study have the following clinical implications for occupational therapy practice:
Occupational therapy practitioners can enhance children’s behavioral and metacognitive EF skills by using peer play as a means of treatment.
In successful implementation of the MOHO, the living environment should be considered as an integral part of the treatment.
Metacognitive deficits in SLD may lead to inaccuracy in the self-assessment results. Therefore, it is better to use more than one instrument to assess mental concepts such as perceived values and competence.
Conclusion
According to parent reports, the peer-play intervention significantly improved the EF of children with SLD during occupational performance. Although the parents perceived change in accordance with their values, the children did not recognize any improvement in level of competence. Perhaps time may offer a great help to address this discrepancy. According to the MOHO, there is a strong probability that children receive more positive feedback from the environment over time, and such feedback consequently may change their perceived values or competence.
Footnotes
Acknowledgments
We thank Akram Parand and Saeed Akbari-Zardkhaneh for their helpful consultations. This project was completed as part of Samaneh Karamali Esmaili’s PhD thesis in occupational therapy, was supported by a grant from the Iran University of Medical Sciences (95/D/320/496), and was registered in the Iranian Registry of Clinical Trials (![]() ; IRCT2015022321208N1).
; IRCT2015022321208N1).