
Abstract
The number of older adults engaging in health promotion, management, and maintenance programs has increased over past decades. More than 90% of older adults are currently living with at least one chronic condition, and about 75% live with multiple chronic conditions (National Council on Aging, 2016). Multiple chronic conditions in older adults are associated with decreased health-related quality of life (QOL; Barile et al., 2013) and decreased occupational performance (Barstow, Warren, Thaker, Hallman, & Batts, 2015). In 2010, 86% of all health care spending in the United States went to treatment of adults living with one or more chronic medical conditions (Agency for Healthcare Research and Quality, 2010; Centers for Disease Control and Prevention, 2016).
Health promotion, maintenance, and management interventions are important for older adults, especially considering the adverse effects of chronic conditions on QOL, occupational performance, and health care costs. However, some people with chronic conditions have difficulty following through with self-management health promotion recommendations (Spaling, Currie, Strachan, Harkness, & Clark, 2015). Occupational therapy practitioners are important members of health care teams working with people with multiple chronic conditions, supporting them to engage in self-management activities (Leland, Fogelberg, Halle, & Mroz, 2017). Practitioners can assist clients in establishing, restoring, and maintaining self-management techniques with a focus on health-promoting routines and habits (American Occupational Therapy Association [AOTA], 2014).
A previous review of the literature looked at articles published from 1990 to 2008 on occupation- and activity-based health management and maintenance interventions. That review found moderate to strong evidence that client-centered occupational therapy improves occupational performance related to health management for community-dwelling older adults (Arbesman & Mosley, 2012). The current systematic review is an update and expansion of the previous review and addresses the question, What is the evidence for the effect of health promotion, management, and maintenance interventions within the scope of occupational therapy on the occupational performance, QOL, and health care utilization of community-dwelling older adults?
Method
Reviews of the literature on productive aging were conducted through AOTA’s Evidence-Based Practice (EBP) Project and focused on intervention effectiveness studies relevant to community-dwelling older adults and within the scope of occupational therapy practice. The method for the reviews was specified in advance and documented in a protocol. The authors—two occupational therapy faculty and two occupational therapy graduate students—conducted the review described in this article through an academic partnership.
Literature Search
Search terms for the review were developed by the methodology consultant to the EBP Project and AOTA staff, in consultation with the review authors and an advisory group. The search terms were developed not only to capture pertinent articles but also to make sure that the terms relevant to the specific thesaurus of each database were included (See Supplemental Table 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). A medical research librarian with experience in completing systematic review searches conducted the search and confirmed and improved the search strategies.
Databases and sites searched included Medline, PsycINFO, CINAHL, and OTseeker. In addition, consolidated information sources, such as the Cochrane Database of Systematic Reviews, were included in the search. Moreover, reference lists from articles included in the systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included. Search results from the other review questions in the productive aging EBP Project were also included for screening.
Screening and Selection
The review was limited to peer-reviewed scientific literature published in English. The intervention approaches examined were within the scope of occupational therapy practice and were provided to older adult participants with an average age ≥65. To determine whether the intervention was within the scope of occupational therapy practice, we focused on the definition of health management and maintenance in the Occupational Therapy Practice Framework: Domain and Process (AOTA, 2014): “developing, managing, and maintaining routines for health and wellness promotion, such as physical fitness, nutrition, decreased health risk behaviors, and medication routines” (p. S19). This definition focuses on the incorporation of routines into the intervention. Therefore, we did not include studies that looked at interventions that, for example, involved only teaching exercise. However, if studies focused on incorporating exercise into daily routines, and if the outcomes and other inclusion criteria were appropriate, we included them in this review.
All participants in selected studies were older adults living in the community, including a retirement home or assisted living facility, or in a hospital setting (i.e., acute, subacute, rehabilitation) if they were being discharged to a community-based dwelling. Included studies also had participants who were older adults with diabetes, arthritis, cardiac disease, or other chronic conditions, including mild cognitive impairment and mild Alzheimer’s disease. Finally, studies that measured QOL, health care utilization, or any area of occupational performance were included. In this article, we use the phrase health promotion to convey all of the intervention areas within health promotion, management, and maintenance. The literature included in the review was published between October 2008 and December 2015.
The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Studies were excluded if the average age of participants was <65 or if the participants were living in a hospital setting but not being discharged to the community. In addition, articles on older adults were excluded if participants had acute or chronic conditions covered in an AOTA Practice Guideline, such as stroke, moderate or severe Alzheimer’s disease, or low vision.
Levels of Evidence
Our team reviewed the articles according to their quality (scientific rigor and lack of bias) and levels of evidence. AOTA uses standards of evidence modeled on those developed in evidence-based medicine (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). This model standardizes and ranks the value of scientific evidence for biomedical practice. In this system, the highest level of evidence, Level I, includes systematic reviews of the literature, meta-analyses, and randomized controlled trials (RCTs). Other levels of evidence include Level II studies, in which assignment to a treatment or a control group is not randomized (cohort study); Level III studies, which do not have a control group; Level IV studies, which use a single-case experimental design, sometimes reported over several participants; and Level V studies, which are case reports and expert opinions that include narrative literature reviews and consensus statements. Level IV and V studies were not included in this systematic review because they did not provide additional information beyond the Level I, II, and III studies retrieved.
Data Abstraction and Risk of Bias
Each article included in the review was abstracted in an evidence table that provides a summary of the method and findings of the article. AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. All studies are summarized in Supplemental Table 2 (online). The risk of bias of individual studies was assessed using the methods described by Higgins, Altman, and Sterne (2011; see Supplemental Table 3, online).
We adapted the strength-of-evidence designations in the system proposed by the U.S. Preventive Services Task Force (2012). Consistent results from well-conducted studies, usually at least 2 RCTs, were graded as strong. When there was only 1 RCT or 2 or more studies at lower levels of evidence, we graded the evidence as moderate. When there were only a few studies with low levels of evidence, we graded the evidence as limited. When some studies supported the intervention but others did not, we graded the evidence as mixed. Finally, when there were not enough studies or studies were of too low quality to make any clear statement, we graded the evidence as insufficient.
Results
A total of 12,243 citations and abstracts were initially obtained. The methodology consultant to the EBP Project completed the first step of eliminating references on the basis of duplicates and titles. This screening yielded 449 citations. In addition, 1,000 additional potential citations were obtained from other review questions, and 7 abstracts were retrieved through hand searching reference lists. Our review team screened these 1,456 citations and abstracts, which resulted in 154 potential articles. The full text of these potential articles was reviewed, and 38 articles (covering 36 studies) were included in the review (Figure 1).
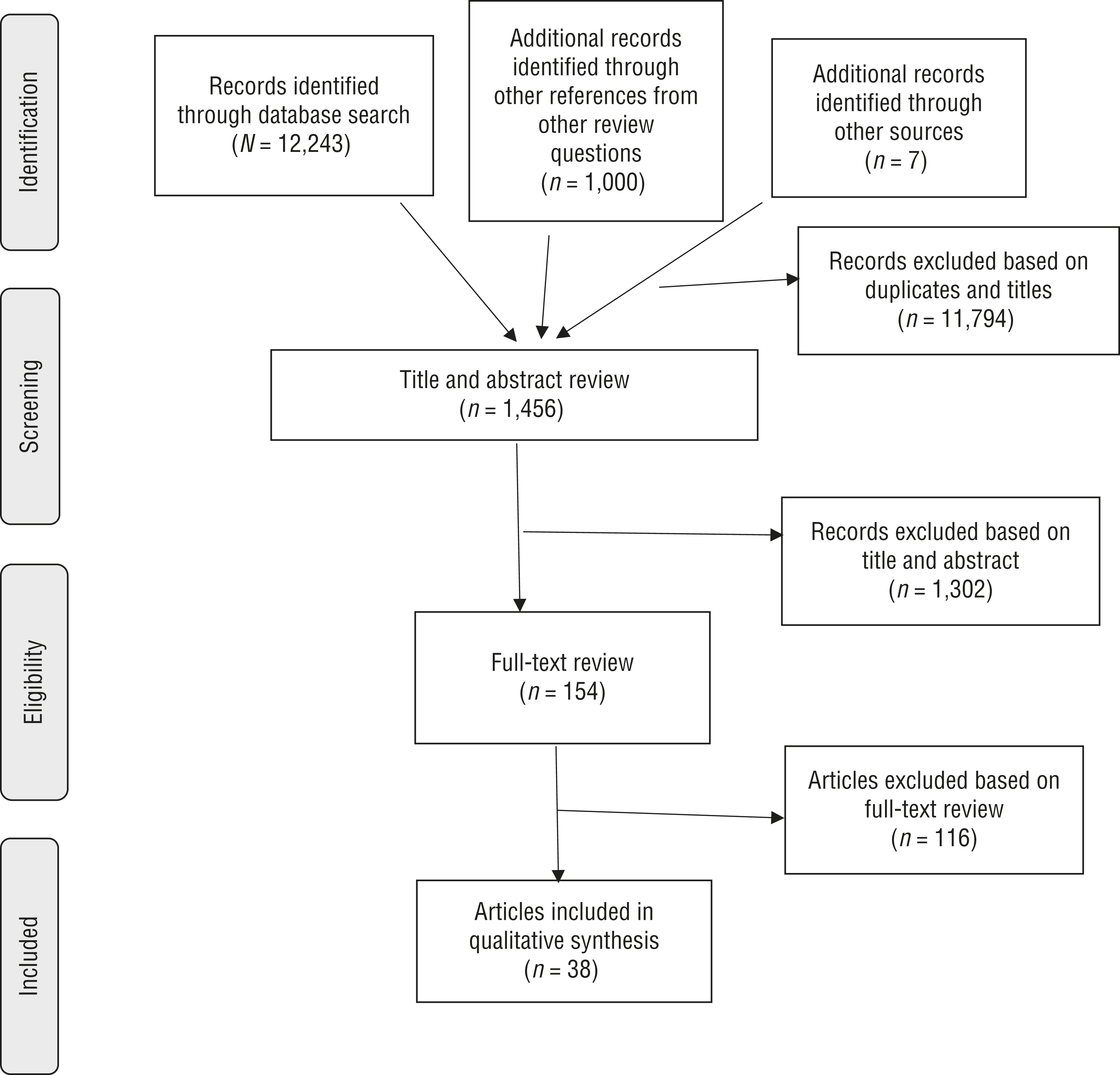
Flow diagram for studies included in the systematic review.Figure format from “Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement,” by D. Moher, A. Liberati, J. Tetzlaff, and D. G. Altman; PRISMA Group, 2009, PLoS Medicine, 6(6), e1000097. https://doi.org/10.1371/journal.pmed.1000097
Of the 36 studies, 19 were Level I RCTs, 6 were Level II studies, and 11 were Level III studies. The studies occurred throughout the world, including 8 in the United States, 5 in Canada, 10 in Europe, 6 in Asia, and 7 in Australia, providing breadth in ethnic diversity. Whereas 4 of the studies explored the effectiveness of interventions for well older adults and 12 for older adults living with any chronic disease, the other studies focused on older adults with specific diseases including diabetes, cardiac conditions, pulmonary conditions, arthritis, and pain. Thirteen studies included an occupational therapist either as the primary interventionist or as part of a multidisciplinary team.
These 36 studies, which explored the effectiveness of health promotion interventions within the scope of occupational therapy practice, all measured occupational performance, QOL, or health care utilization. Occupational performance outcome measures varied but included basic activities of daily living (ADLs) and instrumental activities of daily living (IADLs), leisure, and social participation (e.g., ADL Staircase [Jakobsson, 2008]; Nottingham Extended ADL Scale [Nouri & Lincoln, 1987]; Impact on Participation and Autonomy questionnaire [Cardol et al., 1999]; social activity questions such as how far and how often they go out). QOL measures included either the 36-item Short Form Survey (SF–36; Ware & Sherbourne, 1992) or diagnosis-specific QOL measures (e.g., St. George’s Respiratory Questionnaire; Jones, Quirk, Baveystock, & Littlejohns, 1992). Health care utilization outcome measures most often consisted of self-reported number of days in the hospital, number of emergency room visits, or number of visits to a primary care physician.
All studies included in this systematic review implemented multicomponent health promotion interventions. The qualitative synthesis of the 36 studies addressed four key categories of intervention format: (1) standard and modified Stanford Chronic Disease Self-Management Programs, (2) group interventions other than the Stanford Chronic Disease Self-Management Programs, (3) individual interventions, and (4) combined group and individual interventions. Because the synthesis of data was based on intervention format, the categories were mutually exclusive. Initially, we explored synthesizing the data on the basis of participant condition, intervention component, and interventionist, but none of these features appeared to make a difference in outcomes. Therefore, findings are summarized by type of intervention and then by type of outcome.
Standard and Modified Stanford Chronic Disease Self-Management Programs
Sixteen articles reporting on 14 studies explored the impact of the manualized Stanford Chronic Disease Self-Management Program (CDSMP) or a modified version of this program (mCDSMP) on occupational performance, QOL, or health care utilization of older adults. CDSMP is a group intervention for people with any type and number of chronic conditions and is led by at least one peer leader who is living with one or more chronic conditions.
Participants in a CDSMP group are taught disease-related problem solving, action planning, and decision making. CDSMP also focuses on skill mastery related to topics such as medication management, communication with health care providers and family members, nutrition, and exercises to improve physical functioning. In addition, the program highlights individualized goal setting. Coping strategies are discussed in psychoeducational groups to address experiences such as pain and fatigue. CDSMP focuses on increasing participants’ confidence in managing their chronic conditions. The program is held once a week for 2.5 hr over 6 wk (Stanford Medicine, 2017).
The studies using mCDSMP modified the program by making the program disease specific, replacing the peer leader with a trained health professional, or changing the duration of the session (range = 1.5–3 hr). Additionally, 1 study used a virtual format for the group (Jaglal et al., 2014). Otherwise, the components of CDSMP were retained in the modified versions of this program.
Occupational Performance.
Strong evidence demonstrates the effectiveness of using CDSMP or mCDSMP to improve occupational performance. Two Level I studies, 1 Level II study, and 4 Level III studies demonstrated statistically significant results supporting the use of CDSMP or mCDSMP with older adults to improve occupational performance (Garvey, Connolly, Boland, & Smith, 2015, Level I; Klug, Toobert, & Fogerty, 2008, Level III; Lorig, Ritter, Ory, & Whitelaw, 2013, Level III; Melchior et al., 2013, Level III; Ory et al., 2014, Level II; Rose et al., 2008, Level III; Smeulders et al., 2009, Level I). Only 1 study that looked at improvement in occupational performance as one of the outcomes did not find statistically significant improvement (Lorig, Ritter, Villa, & Armas, 2009, Level I).
Quality of Life.
The evidence for the effectiveness of CDSMP or mCDSMP in improving QOL was mixed. Two Level I studies and 1 Level III study demonstrated significant results (Lorig et al., 2013, Level III; McGillion et al., 2008, Level I; Smeulders et al., 2010, Level I). All 3 studies used a modified version of the CDSMP, including participants with the same condition (e.g., diabetes, chronic angina). Six studies that measured QOL as one of the outcomes did not find significant results (Ackerman, Buchbinder, & Osborne, 2012, Level I; Garvey et al., 2015, Level I; Kim & Youn, 2015, Level II; Ory et al., 2014, Level II; Packer et al., 2012, Level III; Taylor et al., 2012, Level I).
Health Care Utilization.
Strong evidence indicates that CDSMP or mCDSMP is not effective in decreasing health care use. Only 1 of the 8 studies that measured health care use demonstrated a significant decrease in participants’ emergency room visits and hospitalizations (Ory et al., 2013, Level III). The other studies showed no significant improvement in reducing health care utilization (Ackerman et al., 2012, Level I; Garvey et al., 2015, Level I; Jaglal et al., 2014, Level III; Lorig et al., 2009, Level I; Lorig et al., 2013, Level I; Rose et al., 2008, Level III; Smeulders et al., 2009, Level I).
Group Interventions Other Than Stanford Chronic Disease Self-Management Programs
Five studies looked at health promotion group interventions for older adults that were not directly related to the CDSMP model. These studies evaluated the effectiveness of a manualized pain self-management group (Nicholas et al., 2013, Level I), an occupation-based self-management group (O’Toole, Connolly, & Smith, 2013, Level III), a group based on the Model of Human Occupation (Yamada, Kawamata, Kobayashi, Kielhofner, & Taylor, 2010, Level I), a joint protection group (Dziedzic et al., 2015, Level I), and a self-management group for people with osteoarthritis of the knee (Coleman et al., 2012, Level I).
These group interventions did incorporate some CDSMP components. For example, some included problem solving and skill mastery, and others focused on goal setting. All 4 Level I studies focused on a specific group of participants, including those with osteoarthritis of the knee, osteoarthritis of the hand, non–cancer-related pain, or well older adults. The Level III study addressed intervention effectiveness for a broader group, including older adults with two or more of any chronic health condition.
Occupational Performance.
Strong evidence demonstrates the effectiveness of group health promotion interventions other than CDSMP or mCDSMP to improve occupational performance. Two Level I studies (Coleman et al., 2012; Nicholas et al., 2013) and 1 Level III study (O’Toole et al., 2013) demonstrated significant results supporting the effectiveness of these interventions in improving occupational performance for older adults.
Quality of Life.
Strong evidence was found for the effectiveness of group health promotion interventions other than CDSMP or mCDSMP to increase QOL in older adults, supported by 3 Level I RCTs (Coleman et al., 2012; Dziedzic et al., 2015; Yamada et al., 2010). O’Toole et al. (2013, Level III) did not find a significant improvement for this outcome. All 4 studies included goal setting and psychoeducation. The 3 studies that found significant improvement in QOL, however, also included a skill mastery or practice component.
Health Care Utilization.
None of the studies of group interventions other than Stanford Chronic Disease Self-Management Programs measured health care utilization.
Individual Interventions
Twelve studies examined health promotion interventions delivered in an individual format. Although the interventions varied greatly in number of visits and length of time, interventionist (occupational therapist, other health professional), format (face to face, telephone, both face to face and telephone), location of study (Europe, Asia, Australia, North America), and condition (e.g., cardiopulmonary disorder, diabetes, chronic illness), the interventions had some noteworthy similarities. Nine of the 12 studies included goal setting and an educational component, and many of the studies also included a problem-solving component, addressed coping skills, or provided opportunity for practice and skill mastery during the sessions.
Occupational Performance.
Strong evidence was found for the effectiveness of one-to-one health promotion interventions over an extended period in improving occupational performance. Four studies found significant improvement in occupational performance (Jonkers, Lamers, Bosma, Metsemakers, & van Eijk, 2012, Level I; Lewin, Alfonso, & Alan, 2013, Level I; Lewin & Vandermeulen, 2010, Level II; Moriyama, Takeshita, Haruta, Hattori, & Ezenwaka, 2015, Level II). These studies provided multiple visits over a period of time ranging from 3 mo to 1 yr. Two Level I studies did not show improvement (Sundsli, Söderhamn, Espnes, & Söderhamn, 2014; Wetzels, van Weel, Grol, & Wensing, 2008); both provided a much briefer intervention (one home visit and one follow-up phone call; Wetzel et al., 2008) or no face-to-face visits (five telephone sessions; Sundsli et al., 2014).
Quality of Life.
Mixed evidence was found for one-to-one health promotion interventions to improve QOL. Of the 6 studies that provided individual intervention and measured QOL, 2 Level I studies (Moriyama et al., 2009; Song, Yong, & Hur, 2014) demonstrated positive results, whereas 1 Level I study (Azad, Molnar, & Byszewski, 2008), 2 Level II studies (Moriyama et al., 2015; Wood-Baker, Reid, Robinson, & Walters, 2012), and 1 Level III study (Kazawa & Moriyama, 2013) did not demonstrate significant improvement in QOL.
Health Care Utilization.
The evidence is mixed for one-to-one intervention to decrease health care utilization. Three studies showed a significant decrease in health care utilization (Lewin, Alfonso, & Alan, 2013, Level II; Lewin, De San Miguel, et al., 2013, Level I; Lewin & Vandermeulen, 2010, Level II), whereas the other 4 studies did not demonstrate significant improvement (Azad et al., 2008, Level I; Moriyama et al., 2015, Level II; Wetzels et al., 2008, Level I; Wood-Baker et al., 2012, Level II).
Combined Group and Individual Interventions
Five studies involved interventions that combined both group and individual sessions. The group component in these studies ranged in total number of hours from one 2-hr workshop to twice-weekly sessions over 10 wk. The individual aspect was widely different across studies as well, including two individual telephone calls, one 30-min appointment to set goals, one home visit, a weekly session for up to 6 wk, and up to 10 1-hr sessions depending on individual need. Intervention components common to all of these studies were inclusion of group process and a psychoeducational component. Skill mastery was included in 4 of the 5 studies. Additionally, 4 of the 5 studies had an occupational therapist as either the only interventionist or a member of a multidisciplinary team.
Occupational Performance.
Moderate evidence supports the effectiveness of a combined group and individual intervention to improve occupational performance in older adults. Only 2 studies measured occupational performance outcomes, and both demonstrated significant improvement in this area (Dugow & Connolly, 2012, Level III; Gustafsson et al., 2012, Level I).
Quality of Life.
Mixed evidence was found for the effectiveness of a combined group and individual intervention to improve QOL. Two studies showed a significant improvement in QOL (Clark et al., 2012, Level I; Mendelson, McCullough, & Chan, 2011, Level III) and 1 study (Hochhalter, Song, Rush, Sklar, & Stevens, 2010, Level I) did not. Hochhalter et al. (2010) used a “coach” as the interventionist, whereas the other studies included an occupational therapist. Hochhalter et al. also provided the least amount of intervention time, a 2-hr workshop and two follow-up telephone calls.
Health Care Utilization.
None of the studies that focused on group and individual health promotion interventions measured health care utilization.
Discussion
This systematic review builds on the results of a past review (Arbesman & Mosley, 2012) by including evidence through 2015 and studies that examined QOL and health care utilization along with occupational performance. A solid body of evidence relates to health promotion interventions specific to chronic conditions. The evidence-based Stanford CDSMP appears often in the literature in studies using the program in a variety of ways, including with groups of individuals with specific chronic conditions, professional leaders instead of or with peer leaders, and adaptations to the length of the program. It appears that CDSMP, no matter how it is modified, is effective in improving occupational performance for older adults living in the community. All formats of health promotion interventions were effective in improving occupational performance, and group programs other than CDSMP or mCDSMP were also effective in improving QOL. The 1 Level I study that provided intervention in a one-to-one format that did not demonstrate positive effects for occupational performance focused on well older adults (Sundsli et al., 2014); there may be less room for change for healthy older adults than for those living with multiple chronic conditions.
Many of the studies used particular mechanisms to support behavior change, and occupational therapy practitioners should consider the use of these mechanisms when working with older adults in the area of health promotion. In particular, in addition to ensuring that clients incorporate a health behavior into their routine, setting individualized goals, teaching coping strategies, using problem solving, and practicing skills likely facilitate goal attainment.
When providing individual health promotion interventions to older adults, occupational therapy practitioners should consider doing so over an extended period of time (e.g., at least 3 mo, with multiple visits). None of the studies that applied individual interventions used a peer leader or a group format, both key components of CDSMP programs. Therefore, although peer support and modeling appear to be important features of group programs, significant improvement in outcomes can also be made during individual sessions.
This systematic review has several limitations. Different mechanisms to support behavior change were used to develop interventions in the reviewed studies. Therefore, it is difficult to determine which specific components of the interventions led to the positive outcomes. In addition, a variety of outcome measures were used, making meaningful comparisons across studies challenging. The studies occurred throughout the world, demonstrating the broad effectiveness of health promotion programs; however, the feasibility of implementation may be affected by differences in health care systems among countries. Although the variety of populations studied suggests ethnic diversity, the data regarding racial diversity are limited. Most of the studies had low reporting bias, but because almost half (17 of 36) were not RCTs, they had relatively high selection bias (Supplemental Table 3). Finally, because of the nature of the interventions, blinding of participants rarely occurred, leading to high performance bias. Despite these challenges, this systematic review provides strong support for occupational therapy practitioners to consider using health promotion, management, and maintenance interventions when working with older adults living in the community.
Implications for Occupational Therapy Research
Future research is needed to determine whether a group intervention is more effective when participants all have the same condition, so that content can be disease specific, or different diagnoses, to benefit from the variety of experiences. In addition, the benefits and challenges of different group leaders were not addressed in the reviewed studies. Many of the studies included a nurse or health professional other than an occupational therapy practitioner as the interventionist. It would be beneficial to further explore the unique contribution of an occupational therapy practitioner in health promotion interventions.
Only 2 studies in this systematic review provided intervention completely by means of a virtual format (Jaglal et al., 2014; Sundsli et al., 2014). Additional research is needed to explore the effectiveness of telehealth health promotion interventions with older adults. As health care costs continue to rise, occupational therapy practitioners need to use evidence-based interventions that are cost effective.
The programs reviewed did not demonstrate decreased health care utilization. Further research is needed to understand the health care utilization implications of health promotion interventions. For example, it is possible that an intervention might facilitate clients’ ability to navigate the health care system and, therefore, result in increased use of the health care system.
Finally and, possibly, most important, future research is needed to determine how best to tailor programs to meet the health promotion needs of older adults by clarifying which intervention components are most effective. For example, is goal setting the key factor, or does the use of problem solving make the most difference in achieving outcomes?
Implications for Occupational Therapy Practice
Occupational therapy practitioners working with older adults in the community must understand the influence of aging and chronic illness on occupational performance, QOL, and health care utilization. Practitioners should consider
Providing group or individual health promotion, management, and maintenance interventions to improve occupational performance;
Providing group health promotion, management, and maintenance interventions to improve QOL; and
Including individualized goal setting, coping strategies, problem-solving techniques, and skill-specific practice in health promotion, management, and maintenance interventions with older adults.
Most important, occupational therapy practitioners must remember that older adults bring their unique background, strengths, and needs to the therapy session and that interventions must be tailored accordingly.
Supplemental Material
Supplementary material for Effectiveness of Health Promotion, Management, and Maintenance Interventions Within the Scope of Occupational Therapy for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.030346.pdf for Effectiveness of Health Promotion, Management, and Maintenance Interventions Within the Scope of Occupational Therapy for Community-Dwelling Older Adults: A Systematic Review by Sue Berger, Anne Escher, Emily Mengle and Nicole Sullivan in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman and Marian Arbesman for their consistent support and guidance in the methodology of this review.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.