
Abstract
More than 1 in 4 adults aged ≥65 experience a fall each year (Stevens et al., 2012), and an estimated 2.8 million older adults are treated in the emergency room annually as the result of a fall (Centers for Disease Control and Prevention [CDC], 2016). Devastating consequences of falls include hip fracture, traumatic brain injury, and reduced ability to perform daily living tasks (CDC, 2016). Direct medical costs of fall-related injuries exceed $31 billion each year (Burns, Stevens, & Lee, 2016).
Research has demonstrated that most falls among older adults are multifactorial in nature, resulting from the interaction of fall risk factors (Deandrea et al., 2010) such as impaired mobility skills, medication side effects, impaired vision, improper footwear, and environmental hazards (Bloch et al., 2010; Deandrea et al., 2010). The number of studies examining strategies to prevent falls has grown exponentially. Identifying the most effective fall prevention intervention strategies to implement requires a holistic approach because of the interplay among clients’ medical status and physical abilities, environments, and desired occupations.
Occupational therapy practitioners have the skills and knowledge to prevent falls among older adults through a variety of evidence-based interventions. However, research on the effectiveness of fall prevention interventions within the scope of occupational therapy is limited. A systematic review of research on the effectiveness of home modification and fall prevention programs for community-dwelling older adults sponsored by the American Occupational Therapy Association (AOTA) Evidence-Based Practice (EBP) project was an initial step in demonstrating occupational therapy’s value in this area (Chase, Mann, Wasek, & Arbesman, 2012).
Since that review, numerous research studies have been conducted on fall prevention interventions. The previous review was limited to interventions delivered solely in the community, omitting those delivered during transitions from health care settings back to the community (Chase et al., 2012). Therefore, an updated review was needed, one that incorporated the increased availability of literature on fall prevention interventions that are within the scope of occupational therapy. Moreover, preventing falls is essential because accidental falls are often a reason for hospital readmission (Hill, Hoffmann, & Haines, 2013; Mahoney et al., 2000), and reducing readmissions is a high priority for health systems given the financial incentives associated with the Centers for Medicare and Medicaid Services (CMS; 2016) 30-day hospital readmission quality measure and because major falls are a mandated postacute care quality indicator.
Objective
The objective of this systematic review was to update the current knowledge base to reflect emerging evidence and broaden the evidence to include not only community-based fall prevention studies but also interventions delivered within the health care system when outcomes are captured after community discharge. This review excluded research on home modification interventions because these were included in a separate AOTA systematic review (Stark, Keglovits, Arbesman, & Lieberman, 2017) and are discussed extensively in the AOTA Practice Guideline on this topic (Siebert, Smallfield, & Stark, 2014). The current review question was, What is the evidence for the effect of fall prevention interventions on fall-related outcomes, occupational performance, quality of life (QOL), and health care facility readmissions for community-dwelling older adults?
Method
This systematic review was supported by AOTA’s EBP Project (Lieberman & Scheer, 2002). It is one of six studies reviewing the productive aging literature for the EBP Project. The study was executed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009). The fall prevention intervention research question and search terms were developed through a collaborative process with the AOTA methodologist, staff, and medical research librarian and an advisory group that included the review authors (search terms are listed in Supplemental Table 1, available at http://otjournal.net; navigate to this article, and click on “Supplemental”).
An experienced medical research librarian conducted and modified the search using Medline, PsycINFO, CINAHL, and OTseeker. Additional sources, such as the Cochrane Database of Systematic Reviews, reference lists of included articles, and hand searches, were used to ensure that appropriate articles were included. Citations of articles were initially reviewed by the EBP Project consultant and then by the review authors. Review authors and the EBP Project consultant determined whether the articles met the inclusion criteria, identified the level of evidence for each article, and characterized the quality of the evidence (i.e., risk of bias).
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: intervention studies that were published in English in peer-reviewed journals between 2008 and 2015; that evaluated fall prevention interventions within the scope of occupational therapy; and that included fall-related outcomes, QOL, occupational performance (e.g., activities of daily living [ADLs] or instrumental activities of daily living [IADLs]), or hospital readmissions as a primary outcome. QOL, occupational performance, and hospital readmissions were included as additional outcomes for fall interventions given that falls among older adults often result in increased morbidity, decreased QOL, and heightened risk of readmission to the health care system. Examples of fall-related outcomes identified in the appraised articles included fall risk, fall events (e.g., number, rate, injuries), falls efficacy (e.g., measured by the Activities-Specific Balance Confidence Scale [Powell & Myers, 1995]), fear of falling, awareness of strategies to reduce fall risk, implementation of changes to reduce fall risk, and improved mobility assessed by performance-based measures (e.g., Berg Balance Scale, Timed Up and Go test; Berg, Wood-Dauphinee, Williams, & Gayton, 1989; Hill et al., 2013; Podsiadlo & Richardson, 1991).
Additional inclusion criteria were that the study participants had to have a mean age of ≥65 and that the intervention had to be provided in the community or in a health care setting with fall outcome measures captured after community discharge (e.g., home, assisted living facility). Articles were excluded if they were case series, pilot studies, case reports, expert or consensus opinions, conference proceedings, non–peer-reviewed research literature, and dissertations or theses; if they examined interventions outside the scope of occupational therapy; if they were published outside the inclusion dates; and if the topics were covered in other AOTA Practice Guidelines (e.g., home modifications).
AOTA uses the following levels of evidence, modeled from those used in evidence-based medicine (Lieberman & Scheer, 2002; Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996):
Level I—systematic reviews, meta-analyses, randomized controlled trials (RCT)
Level II—two groups, nonrandomized studies (e.g., cohort, case-control)
Level III—one group, nonrandomized studies (e.g., before–after, pretest and posttest)
Level IV—single-subject design, case series
Level V—case reports and expert opinion, including narrative literature reviews and consensus statements.
These categories were applied by the authors with guidance from the AOTA methodologist and staff to each of the appraised research studies. The AOTA methodologist worked with the authors to make final determinations if there was uncertainty.
Data Extraction, Risk of Bias, and Data Analysis
Before reviewing articles, the authors reviewed the Scope of Practice (AOTA, 2014b) and the Occupational Therapy Practice Framework: Domain and Process (AOTA, 2014a) to help identify whether articles fell within the occupational therapy scope of practice. Then, two reviewers (the authors), one researcher and one clinician, individually evaluated each article, first by title and abstract and then by full text, to determine whether it met the inclusion criteria. At each stage of the review process (i.e., title, abstract, full manuscript review), the review authors discussed their individual decisions on each article, reconciled any differences, and established a list of articles to be reviewed at the next stage. Whenever a disagreement occurred, review authors shared their evaluation of the article in the context of the protocol and then discussed differences of opinion and came to a consensus on whether to include the article in the study.
Consistent with the PRISMA guidelines (Moher et al., 2009), Figure 1 depicts the flow of articles through the title and abstract review, full-text article review, and final sample. Data were extracted from the selected articles to complete the evidence and risk of bias tables, which were reviewed by AOTA staff and the EBP Project consultant and methodologist to ensure accuracy. Data extracted for the evidence table included location of the study, sample demographics, intervention components and comparators, and results (Supplemental Table 2, online). The risk of bias appraisal was guided by the Cochrane risk of bias guidelines for intervention studies (Higgins, Altman, & Sterne, 2011; Supplemental Table 3, online) and by the Assessment of Multiple Systematic Reviews (AMSTAR) system (Shea et al., 2007) for systematic reviews and meta-analyses (Supplemental Table 4, online).
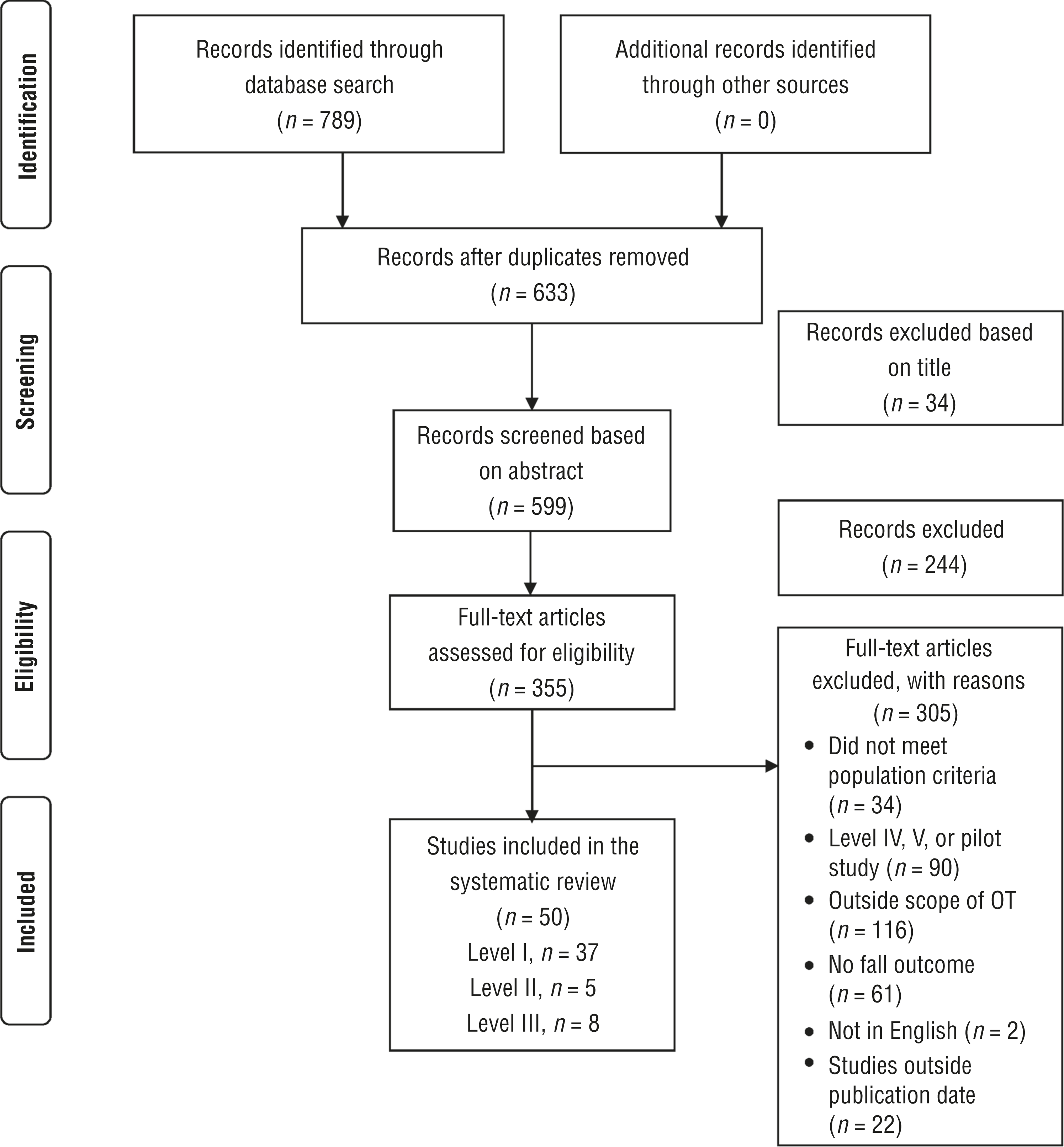
Flow diagram for studies included in the systematic review.
Using guidance from the AOTA methodologist and EBP Project staff, the authors individually grouped the results of the analysis into four major themes. The strength of the evidence for each theme was assigned on the basis of the U.S. Preventive Services Task Force (2012) ratings, as follows:
Strong evidence—consistent results from at least 2 well-conducted RCTs
Moderate evidence—at least 1 RCT or at least 2 studies providing lower levels of evidence, with inconsistencies in findings across well-designed individual studies
Limited evidence—too few research studies, often with flaws, to make specific recommendations
Mixed evidence—inconsistent or conflicting findings throughout studies.
A meta-analysis was not conducted for this review given the heterogeneity of the studies with respect to the diversity of outcomes assessed, the outcome instruments used, and the variation in interventions (e.g., type, duration, frequency; see Supplemental Table 2 for details).
Results
Fifty articles were included in this review, including 37 Level I studies, 5 Level II studies, and 8 Level III studies (see Supplemental Table 2). Research studies were grouped into four themes addressing single-component (14 studies), multicomponent (group-based; 7 studies), multifactorial (individually tailored; 19 studies), and population-based (10 studies) interventions.
Single-Component Fall Prevention Interventions
Single-component interventions address a single fall risk factor, such as balance (Panel on Prevention of Falls in Older Persons, 2011). Among the 14 studies, 11 were Level I studies (10 RCTs, 1 systematic review and meta-analysis), 2 were Level II studies, and 1 was a Level III study. These studies examined interventions including exercise (n = 11), guided imagery and relaxation (n = 1), occupational therapy home and functional assessment (n = 1), and fall prevention education (n = 1). Exercise interventions included functional, dual-task or multitask, virtual reality, water-based, and standard multidimensional approaches.
Overall, mixed evidence was found regarding the use of single-component fall prevention interventions. Two Level I functional exercise intervention studies indicated that Lifestyle Integrated Functional Exercise, which embeds exercise into a person’s everyday activities, was effective (Burton, Lewin, Clemson, & Boldy, 2013; Clemson et al., 2012). Three Level I studies support the effectiveness of dual-task or multitask exercises (combining motor and cognitive components) to reduce falls, improve falls self-efficacy, and lessen fall risk (Roaldsen, Halvarsson, Sahlström, & Ståhle, 2014; Silsupadol et al., 2009; Wang et al., 2015). Because of the paucity of studies, the evidence is insufficient regarding the following single-component interventions: water-based exercise (Oh et al., 2015), standard multidimensional exercise (Kim, Yoshida, & Suzuki, 2011), guided imagery and relaxation (Kim, Newton, Sachs, Glutting, & Glanz, 2012), occupational therapy functional and home safety assessment (Johnston, Barras, & Grimmer-Somers, 2010), and education alone (Koestner, Walters, Mattice, Manion, & Seguin, 2009).
Multicomponent Fall Prevention Interventions (Group Based)
Group-based multicomponent fall prevention interventions target a prescribed set of fall risk factors (Panel on Prevention of Falls in Older Persons, 2011). Of the 7 multicomponent intervention studies, 6 were Level I RCTs and 1 was a Level III study. Strong evidence indicates that multicomponent interventions significantly improve fall-related outcomes; 5 Level I studies found a positive effect (Almeida et al., 2013; Comans, Brauer, & Haines, 2010; Kloubec, Rozga, & Block, 2012; Smulders et al., 2010; Szanton et al., 2011), and 2 studies found little to no effect (Beauvais & Beauvais, 2014, Level III; Resnick, Galik, Gruber-Baldini, & Zimmerman, 2012, Level I).
Regarding specific fall-related outcomes, Kloubec and colleagues (2012) found a significant improvement in balance confidence, Smulders and collaborators (2010) a reduction in fall rate, and Almeida et al. (2013) enhanced gait speed. Szanton and colleagues (2011) found improved occupational performance through a reduction in ADL and IADL impairments, improved QOL, and increased falls self-efficacy.
Strategies used in the programs varied, but all included a form of both exercise and education. Exercise approaches included balance, strength, functional tasks, walking, dual-task or multitask activities, obstacle course training, and training in fall techniques. Education topics included feet or footwear risk, energy conservation strategies, safe assistive device use, home modification recommendations, fall recovery, medication management, nutrition and hydration, and relaxation and stress management. Education also focused on risk factors such as reduced cognitive function, postural hypotension, vision impairments, and continence. Three of the 7 studies augmented education and exercise with other components such as pain management (Szanton et al., 2011), focused goal development and monitoring (Resnick et al., 2012), mentoring and motivation (Resnick et al., 2012), or referrals and education about available community resources (Comans et al., 2010; Resnick et al., 2012).
Multifactorial Fall Prevention Interventions (Individually Tailored)
Multifactorial fall prevention interventions are individually tailored to target clients’ multiple fall risk factors (Panel on Prevention of Falls in Older Persons, 2011). Mixed evidence was found for these interventions because of inconsistent or conflicting findings. Of the 19 studies in this theme, 8 (7 RCTs and 1 Level III study) found positive effects on outcomes, such as reductions in fall risk, number or rate of falls, injurious falls, and fear of falling or improvements in balance confidence, balance and mobility skills, awareness of fall reduction strategies, and use of measures to reduce fall risk (Di Monaco et al., 2008; Fox et al., 2010; Kamei et al., 2015; Luck et al., 2013; Palvanen et al., 2014; Sze et al., 2008, Xia, Jiang, Niu, Tang, & Xia, 2009; Zidén, Frändin, & Kreuter, 2008). An additional 4 of the 19 studies, all RCTs, yielded conflicting results depending on the outcome being evaluated (Pérula et al., 2012; Salminen, Vahlberg, Salonoja, Aarnio, & Kivelä, 2009; Sheffield, Smith, & Becker, 2013; Vind, Andersen, Pedersen, Joergensen, & Schwarz, 2010).
The remaining 7 studies, all RCTs, found no effect of the intervention (Conroy et al., 2010; de Vries et al., 2010; Elley et al., 2008; Hendriks et al., 2008; Lee et al., 2013; Markle-Reid et al., 2010; Möller et al., 2014). At least 6 of these 7 studies had fewer than 400 total participants, and the largest had 616 participants. In the 8 studies that found positive effects, 4 had fewer than 400 total participants, and the largest study had approximately 2,300 participants.
Across the 19 multifactorial studies, common interventions included individualized fall risk assessment, environmental intervention, goal development, assessment and training, education, and group activities. Individualized fall risk assessment was included in 18 studies; methods included geriatric or medical assessment or consultation, vision or hearing screening and intervention, medication review, medication management or reduction, and referrals to other disciplines. Environmental interventions, such as home assessment or modification or hazard abatement, were included in 18 studies, including all 8 with positive results. Goal development and monitoring were integrated in 3 studies. Assessment and training on ADLs and IADLs (i.e., occupational performance), assistive devices, self-efficacy, or fear of falling were used in 9 studies. Educational modules focusing on fall prevention, general health, or adaptive or compensatory strategies were included in 12 studies. Group activities augmented individualized prevention strategies (e.g., exercise, psychosocial activities) in 14 studies.
Population-Based Fall Prevention Interventions
Population-based fall prevention interventions are strategies implemented across whole communities (Christoffel & Gallagher, 1999). Ten studies were analyzed, including 2 Level I RCTs, 3 Level II studies, and 5 Level III studies. Moderate evidence was found for the use of population-based fall prevention interventions; because of inconsistencies in findings in 3 studies, the evidence could not be qualified as strong. Six studies found improved fall-related outcomes (Alexander, Sartor-Glittenberg, Bordenave, & Bordenave, 2015, Level III; Chen, Edwards, & Janke, 2015, Level II; Cho et al., 2015, Level III; Smith, Jiang, & Ory, 2012, Level III; Teems, Hausman, Fischer, Lee, & Johnson, 2011, Level III; Zijlstra et al., 2009, Level I), whereas 1 study found no significant effect (Albert et al., 2014, Level II). Three additional studies yielded inconsistent or variable results depending on the outcome measured (Guse et al., 2015, Level I; Robitaille et al., 2012, Level II; Ziljstra et al., 2013, Level III).
Population-based interventions included in the appraisal were categorized as existing effective population-based fall prevention programs (e.g., Stepping On, A Matter of Balance) or as other population-based multicomponent interventions. Six studies evaluated either A Matter of Balance (Alexander et al., 2015, Level III; Chen et al., 2015, Level II; Cho et al., 2015, Level III; Smith et al., 2012, Level III; Zijlstra et al., 2013, Level III) or Stepping On (Guse et al., 2015, Level I) by scaling the interventions to a population level. A Matter of Balance, a peer-led program, includes eight 2-hr group sessions and helps decrease fear of falling and increase activity levels (Tennstedt et al., 1998). Stepping On, a seven-session group intervention, focuses on reducing falls and improving balance confidence (Clemson et al., 2004).
The remaining 4 studies evaluated population-based fall prevention programs across a regional area. These studies focused on multicomponent cognitive–behavioral fall prevention interventions (Zijlstra et al., 2009, Level I); an exercise and fall risk educational program (Albert et al., 2014, Level II; Teems et al., 2011, Level III); and a strength, balance, home safety, and safe behaviors program (Robitaille et al., 2012, Level II).
Discussion
Given the relationships among accidental falls, readmissions, and other adverse events, health care providers, regardless of clinical setting, are challenged to ensure that their clients are receiving high-quality, evidence-based fall prevention services (Leland et al., 2015; Mahoney et al., 2000; Petrella, Payne, Myers, Overend, & Chesworth, 2000; Zuckerman, Sheingold, Orav, Ruhter, & Epstein, 2016). Thus, to optimize client outcomes, the delivery of such interventions must be integrated throughout the care continuum (e.g., acute, postacute, community; Agency for Healthcare Research and Quality, 2011; CMS, 2016). Toward this end, this systematic review summarized the knowledge base for occupational therapy fall prevention intervention, in alignment with national health care quality initiatives and the need to equip clinicians with the current evidence on this area of practice.
As occupational therapy practitioners strive to meet national health care quality goals and optimize client outcomes, they need to become educated on effective evidence-based fall prevention interventions, especially because the incidence of major falls is a mandated postacute care quality measure (CMS, 2016). Because all multifactorial intervention studies with positive results included home assessment, modification, or hazard abatement, practitioners should consider these vital fall prevention components for community-dwelling older adults.
Occupational therapy practitioners have the skills to provide evidence-based fall prevention interventions, given their knowledge of function and the effects of the environment on occupational performance and participation. Despite the growth in fall prevention evidence, this review identified fall prevention intervention areas that need further evaluation and higher level research studies, including the effectiveness of single-component interventions including water-based exercises, standard multidimensional exercises, and guided imagery and relaxation and interventions that seek to prevent health care facility readmissions.
Limitations
Limitations noted during the analysis of the appraised studies included a lack of objective measures, randomization, blinding, a control group, or risk of bias. In addition, several studies had a small sample size or a limited geographic area or used a convenience sample, which may reduce the ability to generalize the results. High attrition during some studies or at follow-up limits the ability to identify whether the intervention results were maintained over time. Other limitations were reporting bias and the omission of other databases such as the European database EMBASE, although EMBASE does have some overlap in articles with Medline.
Implications for Occupational Therapy Practice
The following interventions are recommended for occupational therapy practice on the basis of the results of this review:
Multicomponent or population-based fall prevention strategies that include exercise and educational components
Individualized fall risk assessment, fall prevention education, and home safety assessment, modification, and hazard abatement as multifactorial components
Lifestyle Integrated Functional Exercise to reduce fall risk
Population-based fall prevention programs such as Stepping On and A Matter of Balance, which can be conducted in a variety of settings, including senior centers
Functional exercises plus fall prevention education on proper footwear, home modifications, and fall recovery (e.g., getting up from a fall).
Implications for Occupational Therapy Education
The following are recommendations for occupational therapy educators based on the results of this review:
Describe the differences between single-component, multicomponent, multifactorial, and population-based fall prevention interventions and the evidence behind them.
Inform students about population-based fall prevention programs that are evidence based, such as Stepping On and A Matter of Balance.
Discuss the relationship between the environment and fall prevention.
Implications for Occupational Therapy Research
The following are recommendations for occupational therapy researchers based on the results of this review:
Conduct further high-level fall outcome research on single-component, multicomponent, multifactorial, and population-based interventions to identify effective interventions.
Investigate the effectiveness of water-based exercises, standard multidimensional exercise, guided imagery and relaxation, and occupational therapy home and functional assessment as single-component fall prevention interventions.
Examine the effectiveness of fall prevention interventions in decreasing facility readmissions.
Conclusion
Addressing older adults’ fall risk during postacute care stays and in the community is essential for minimizing future risk and facilitating safe care transitions and aging in place. This systematic review adds to the growing body of literature on effective fall prevention interventions within the scope of occupational therapy practice. It also helps guide occupational therapy practitioners in choosing effective interventions, such as multicomponent group-based programs that include exercise and education on fall reduction techniques and population-based interventions such as A Matter of Balance and Stepping On. These findings can inform the delivery and integration of best practice from acute care to community discharge to minimize falls among community-dwelling older adults.
Supplemental Material
Supplementary material for Occupational Therapy Fall Prevention Interventions for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.030494.pdf for Occupational Therapy Fall Prevention Interventions for Community-Dwelling Older Adults: A Systematic Review by Sharon Elliott and Natalie E. Leland in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
During the time of this study, Dr. Leland was receiving funding from the Agency for Healthcare Research and Quality (HS022907). Preliminary results of this study were presented at the 2017 AOTA Annual Conference & Expo in Philadelphia. The authors thank Deborah Lieberman, Marian Arbesman, and Elizabeth Hunter for their input and expertise in conducting the systematic review or review of the article.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.