
Abstract
This systematic review examines the evidence for the effectiveness of interventions within the scope of occupational therapy that address leisure engagement and social participation among community-dwelling older adults. Eleven Level I, 1 Level II, 1 Level III, and 1 Level IV studies met inclusion criteria. Included articles addressed two themes: interventions supporting social participation and interventions supporting leisure engagement. Strong evidence supports leisure education interventions to enhance leisure engagement, and moderate evidence supports chronic disease self-management programs to support leisure engagement. Mixed evidence exists for community-based group interventions and electronic gaming to support social participation. Routine use of leisure education and chronic disease self-management programs to enhance leisure engagement and selective use of community-based groups and electronic gaming to support social participation are recommended.
Within 30 yr, the population of older adults residing in the United States is expected to reach nearly 84 million (Ortman, Velkoff, & Hogan, 2014). Researchers estimate that 35% of U.S. adults over age 45 are lonely (Wilson & Moulton, 2010). As a population, older adults may experience greater social isolation because they are more likely to live alone, have a chronic illness, lose a significant other, experience transportation or mobility difficulties, have low income, and experience declines in muscle strength (Kharicha et al., 2007; Nicholson, 2009; Wilson & Moulton, 2010).
Older adults who experience loneliness or social isolation have an increased risk of other physical and mental health issues, such as disease, falls, depression, poor nutrition, rehospitalization, cognitive decline, heavy alcohol consumption, high systolic blood pressure, infection, and mortality (Coyle & Dugan, 2012; Lillyman & Land, 2007; Nicholson, 2009; Wilson & Moulton, 2010). Loneliness and social isolation can undermine well-being by leading to feelings of stress and can influence physical, emotional, and psychological health (Coyle & Dugan, 2012; Shankar, McMunn, Banks, & Steptoe, 2011; Wilson & Moulton, 2010). Because health and wellness risks are associated with social isolation and loneliness in older adults, mitigating these health risks may improve not only mental health but also physical health and quality of life (QOL) in this population.
Maintaining social participation and leisure engagement throughout the lifespan is important for enhanced well-being and health (Chang, Wray, & Lin, 2014; Doble & Santha, 2008). Because leisure pursuits often stem from engagement in meaningful occupations identified earlier in life, ensuring that clients maintain this participation while considering new interests is important (Agahi, Ahacic, & Parker, 2006). Social and leisure interests are often interrelated, leading to improvements in both areas even when addressing only one. Leisure participation has been shown to decrease stress, improve psychosocial well-being, and provide meaning in daily occupations (Carruthers & Hood, 2004). Similarly, enhanced social participation and a strong social network have positive implications for engagement in leisure and enrichment in life (Carruthers & Hood, 2004). Embracing the use of occupation-based interventions aimed at health promotion through socialization can decrease health disparities, improve overall health, and enhance QOL (American Occupational Therapy Association [AOTA], 2013, 2014).
Participation in social and leisure activities is critical to health and well-being (Chang et al., 2014; Doble & Santha, 2008). Older adults, who naturally experience many losses during older adulthood, may benefit from interventions designed to promote engagement in social and leisure activities. Encouraging active participation in social and leisure activities that require cognitive, physical, intellectual, or social skills has been shown to decrease cognitive decline and promote physical health (Karp et al., 2006; Wang, Karp, Winblad, & Fratiglioni, 2002). The purpose of this systematic review was to identify and examine the evidence supporting the role of occupational therapy in promoting social participation and leisure engagement for community-dwelling older adults.
Method
This systematic review was one of six reviews on productive aging supported by the AOTA Evidence-Based Practice (EBP) Project. The method for the reviews was specified in advance and documented in a protocol for review authors.
Search Strategy
Search terms for the review were developed by the methodology consultant to the EBP Project and AOTA staff, in consultation with the review authors for each question, and by an advisory group consisting of expert occupational therapy practitioners and researchers in the area of aging. The search terms were developed not only to capture pertinent records but also to ensure that the terms relevant to the specific thesaurus of each database were included. Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) lists the search terms related to the population (community-dwelling older adults), interventions, and study designs included in this systematic review.
A medical research librarian with experience in completing systematic review searches conducted the search and confirmed and improved the search strategies in the following databases: Cochrane Database of Systematic Reviews, CINAHL, Medline, OTseeker, and PsycINFO. The methodology consultant for the EBP Project did the first review of the search results (citations), eliminating all records not relevant to the review scope. The review authors examined reference lists in the articles for potential studies and hand searched selected journals to ensure all appropriate articles were included.
Eligibility Criteria
Several inclusion and exclusion criteria provided the structure for the quality, type, and years of publication of the literature incorporated into the review. This review included peer-reviewed scientific literature published in English between 1995 and 2015. The intervention approaches examined were within the scope of practice of occupational therapy for older adults with an average age ≥65 living in the community, a retirement home, or an assisted living facility or in a rehabilitation, subacute, or hospital setting if they were being discharged to home. Studies were also included if participants were older adults with diabetes, arthritis, cardiac disease, or other chronic conditions, including mild cognitive impairment and mild Alzheimer’s disease.
The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Studies were excluded if the average age of participants was <65 or if participants were living in a skilled nursing facility or were in the hospital but not being discharged to home. Additionally, studies were excluded if they were in an AOTA Practice Guideline and included participants with acute or chronic conditions, such as stroke or moderate or severe Alzheimer’s disease. Studies without outcomes related to social participation or leisure engagement were also excluded from this review.
AOTA uses standards of evidence modeled on those developed in evidence-based medicine (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Records included in the review were rated as follows:
Level I—meta-analyses, systematic reviews, and randomized controlled trials (RCTs)
Level II—two-group nonrandomized studies (e.g., cohort, case-control)
Level III—one-group nonrandomized studies (e.g., before and after, pretest–posttest)
Level IV—descriptive studies (single-subject design, case series)
Level V—case reports and expert opinions that include narrative literature reviews and consensus statements.
Studies included in this review provide Level I, II, or III evidence. Level IV evidence was included only when higher levels of evidence in a given theme were not available. No Level V evidence was included in the review.
Data Extraction
The review authors worked collaboratively to evaluate all articles throughout the entire review process. The authors conducted the initial review individually. Collaborative discussion was used to reach a consensus on all articles and to resolve any disagreement. Each article included in the review was summarized in an evidence table (Supplemental Table 2, online). The studies were categorized into themes and subthemes. The AOTA EBP Project methodology consultant reviewed the evidence table for quality control.
Risk of Bias
Each article was individually assessed for risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias on a scale of low, high, or unclear, as described in the Cochrane risk of bias guideless (Higgins, Altman, & Sterne, 2011). During the rating process, both authors worked collaboratively to reach consensus in each category of bias. Supplemental Table 3 (online) displays the risk of bias for all studies included in this review.
Analysis
Each theme was analyzed for strength of evidence to assist in determining final recommendations for occupational therapy education, research, and practice. Analysis of study design, findings, and risk of bias determined strength of evidence designations. Number of studies and the strength of evidence they provided were determined in accordance with the U.S. Preventive Services Task Force (2014) recommendations, as follows:
Strong evidence indicates consistent results from well-conducted studies, usually at least two RCTs.
Moderate evidence indicates one RCT or two or more studies with lower levels of evidence. Some inconsistency of findings across individual well-conducted studies could preclude a classification of strong evidence and result in a designation of moderate evidence.
Limited evidence indicates few studies, flaws in the available studies, and some inconsistency in findings across individual studies.
Mixed evidence indicates that the findings were inconsistent across studies in a given category.
Insufficient evidence indicates that the number and quality of studies are too limited to make any clear recommendation.
Results
Figure 1 is a flow diagram of record selection. The review team identified 14 articles for inclusion in the final qualitative synthesis. The articles addressed two themes: (1) interventions supporting social participation (7 studies) and (2) interventions supporting leisure engagement (7 studies). For the theme of social participation, 5 Level I studies, 1 Level II study, and 1 Level III study were identified. For the theme of leisure engagement, 5 Level I studies reported in 6 articles and 1 Level IV study were identified.
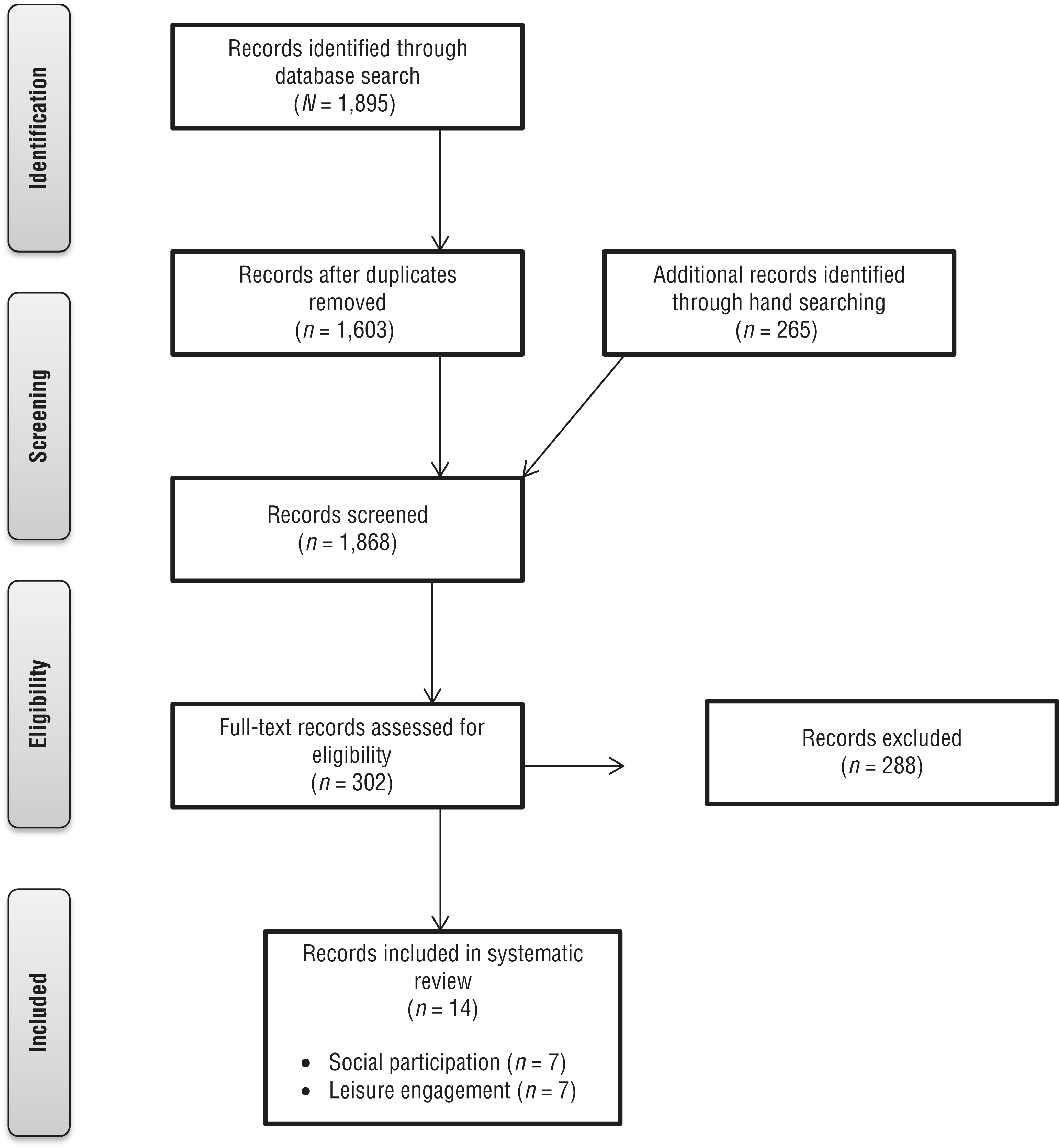
Flow diagram for studies included in the systematic review.
Outcome Measures
Outcome measures used in the studies were varied. For the theme of social participation, measurement tools included primarily self-report measures of social and activity participation, health (e.g., SF–12 and SF–36; RAND, 1994–2018), loneliness (UCLA Loneliness Scale; Russell, 1996), and depression (Geriatric Depression Scale; Yesavage et al., 1982–1983). For the theme of leisure engagement, outcome measures included self-reports of frequency of activity participation, performance of occupations including leisure activities, leisure competence and engagement, and life satisfaction.
Interventions Addressing Social Participation
Seven articles included in this review addressed the effectiveness of interventions within the scope of occupational therapy to promote social participation in community-dwelling older adults. Five articles provided Level I evidence (Creswell et al., 2012; Dickens et al., 2011; Kahlbaugh, Sperandio, Carlson, & Hauselt, 2011; Ollonqvist et al., 2008; Routasalo, Tilvis, Kautiainen, & Pitkala, 2009), 1 article provided Level II evidence (Bell et al., 2011), and 1 article provided Level III evidence (Matuska, Giles-Heinz, Flinn, Neighbor, & Bass-Haugen, 2003). Three main intervention approaches—community-based group interventions, community mentoring, and electronic gaming—were identified.
Community-Based Group Interventions.
Four studies used a community-based group model of intervention either as part of a multicomponent intervention or as a single-component intervention (Creswell et al., 2012; Matuska et al., 2003; Ollonqvist et al., 2008; Routasalo et al., 2009). Group sessions were usually held weekly, and programs lasted from 8 wk to 6 mo. In a Level III study, Matuska et al. (2003) found that group sessions run by occupational therapists resulted in increased social and community participation and significant differences in posttest scores on social functioning. However, in a Level I study, Routasalo et al. (2009) studied the effect of 3-mo psychosocial groups on the outcomes of loneliness and social networking. Participants were assigned on the basis of interest to one of three weekly groups: art or other creative activities, group exercise and discussions, or therapeutic writing and group therapy. Intervention participants reported significant increases in number of new friends but nonsignificant differences in loneliness or social networking compared with control participants.
Creswell et al. (2012, Level I) studied an 8-wk stress reduction program and found a significant decline in loneliness. Finally, Ollonqvist et al. (2008, Level I) examined the effectiveness of intensive multidisciplinary group rehabilitation for frail older adults but found no significant difference between groups on the outcome of loneliness. In combination, the 3 Level I studies and 1 Level III study provide mixed evidence for the use of community-based group interventions to improve social participation among community-dwelling older adults.
Community Mentoring.
One study used a community mentoring model of intervention (Dickens et al., 2011, Level I). Older adults received up to 12 wk of mentoring in self-confidence and engagement in personally meaningful social activities. However, no improvements in the outcomes of social activity or social support resulted from the mentoring relationships. Thus, this study provides moderate evidence against the use of a community mentorship approach to promote social activity and support.
Electronic Gaming.
Two studies used an electronic gaming intervention to address social participation (Bell et al., 2011; Kahlbaugh et al., 2011). In a small Level I study, Kahlbaugh et al. (2011) examined the use of a Nintendo Wii game with another person once per week for 10 wk. This intervention decreased social isolation and loneliness for the intervention group compared with the control group, who watched television with another person. In a Level II study, Bell et al. (2011) investigated the effect of Nintendo Wii games with and without fall prevention education over an 8-wk period on the outcomes of social relationships and social support. They found no significant differences between the intervention and control groups. Therefore, these studies provide mixed evidence for the use of electronic gaming to promote social participation.
Interventions for Leisure Engagement
Five Level I studies reported in six articles (Chang, 2014; Garvey, Connolly, Boland, & Smith, 2015; Janssen, 2004; Searle, Mahon, Iso-Ahola, Sdrolias, & Van Dyck, 1995, 1998; Zingmark, Fisher, Rocklöv, & Nilsson, 2014) and 1 Level IV study (Schweitzer, Mann, Nochajski, & Tomita, 1999) provide evidence for the role of occupational therapy in supporting leisure engagement of community-dwelling older adults. Three intervention types—leisure education, self-management of chronic disease, and assistive devices—were identified.
Leisure Education.
Four Level I studies reported in five articles used leisure education as the intervention (Chang, 2014; Janssen, 2004; Searle et al., 1995, 1998; Zingmark et al., 2014). Janssen (2004) examined a 6-wk group educational program that focused on leisure appreciation, awareness, self-determination, and decision making related to leisure choices and found significant increases on leisure domains of QOL compared with control participants. In a small RCT, Searle et al. (1995, 1998) examined a modified form of a community reintegration program that included 12 individualized sessions consisting of discussion, paper-and-pencil tasks, role-playing, and recreational activities over approximately 17 wk. This leisure education program led to significant increases in perceived leisure control, leisure competence, and leisure boredom compared with a control group (Searle et al., 1995) that were maintained at follow-up (Searle et al., 1998). However, immediate between-group differences in life satisfaction were not maintained at follow-up.
Building on the work of Searle et al. (1995, 1998), Chang (2014) investigated the effect of a similar 12-wk leisure education program addressing leisure competence (e.g., perceptions, capacity, behaviors) delivered 2×/wk for 3 mo on the outcomes of leisure competence and capacity and found improved competence among the intervention group compared with the control group. Finally, Zingmark et al. (2014) used a four-arm RCT to compare one-to-one, client-centered intervention focused on occupational engagement with a group activity intervention, a discussion group intervention, and no intervention. All groups declined in participation over time; however, leisure participation declined slightly less among intervention group participants, with the one-to-one intervention group showing the highest rate of continued leisure engagement. In general, although the dosage and content of the programs varied, strong evidence supports use of leisure education programs in occupational therapy interventions targeting engagement in leisure activities for community-dwelling older adults.
Self-Management of Chronic Disease.
Garvey et al. (2015, Level I) reported on the use of a 6-wk chronic disease self-management program to enhance leisure participation among older adults with multiple chronic conditions. Goal setting, self-management of chronic conditions, and peer support were introduced in weekly meetings that had an occupational therapy emphasis. This intervention led to an increase in activity frequency compared with a control group and improved self-perception of activity performance and satisfaction. This study provides moderate evidence supporting the use of chronic disease self-management programs to address the outcome of leisure activity engagement.
Assistive Devices.
One Level IV study examined assistive device use in relation to leisure participation among community-dwelling older adults with physical disabilities that limited home-based leisure activities (Schweitzer et al., 1999). Participants’ home setup, assistive device use, and barriers to leisure participation were reviewed in structured interviews. Then, an appropriate assistive device was provided to each participant to encourage participation in a personally meaningful leisure activity. Provision of assistive devices led to an increased likelihood of attempting leisure pursuits. Because only one low-level study addressed this subtheme, insufficient evidence supports the use of assistive devices to increase home-based leisure engagement for community-dwelling older adults.
Discussion
This systematic review examined the effectiveness of interventions within the scope of occupational therapy to promote leisure engagement and social participation among community-dwelling older adults. Results provide strong evidence for the use of leisure education programs and moderate evidence for the use of chronic disease self-management programs to enhance leisure engagement of community-dwelling older adults with chronic health conditions. These interventions should be offered routinely to clients in this population who present with decreased participation in leisure activities. Additionally, mixed evidence was found for community-based group interventions and electronic gaming interventions to improve social participation outcomes; therefore, occupational therapy practitioners should consider these interventions on a case-by-case basis.
Implications for Occupational Therapy Education
The role of occupational therapy in community-based practice is expected to rise to meet the challenge of caring for the growing number of older adults in an ever-changing health care environment (Lamb & Metzler, 2014). Preparing future occupational therapy practitioners to meet the needs of older adults living in the community, including social participation and leisure engagement, should be a focus of occupational therapy educational programs. Curricula should include the following:
Education regarding the relationship between leisure and social participation and physical, cognitive, and emotional health and well-being
Education about health conditions and contextual factors that influence participation in social and leisure activities
Training in the use of formal and informal assessments of leisure and social participation
Knowledge and skill training in the delivery of effective interventions for social and leisure participation, including leisure education and electronic gaming.
Implications for Occupational Therapy Research
Occupational therapy has the potential to play a significant role in supporting social participation and leisure engagement among community-dwelling older adults. Occupational therapy researchers need to continue to develop and examine interventions for enhancing these occupations. Further research regarding interventions that improve social and leisure participation will be critical to supporting occupational therapy practitioners in this area of practice. Recommendations for strengthening research in this area include the following:
Use of occupational therapy practitioners as study interventionists
Improvement in the consistency of interventions included in multicomponent interventions
Evaluation of intervention dosages (frequency and duration of intervention) needed for efficacy
Increased consistency in outcome measures used to demonstrate intervention effectiveness
Review of differences in leisure engagement and social participation among older adults residing in assisted living facilities versus those living at home.
Increased quantity and quality of evidence-based interventions that promote social participation and leisure engagement will guide practitioners in providing best practice to community-dwelling older adults.
Implications for Occupational Therapy Practice
On the basis of the results of this review, the following interventions are recommended as part of routine occupational therapy services to community-dwelling older adults at risk of a decline in social participation and leisure engagement:
Leisure education programs to enhance leisure participation
Chronic disease self-management programs to improve leisure participation among those with chronic conditions.
The following interventions should be offered selectively on the basis of individual client characteristics and intervention context:
Community-based group interventions to support social participation
Electronic gaming to enhance social participation.
The following intervention requires further research:
Assistive devices to promote home-based leisure participation for clients with physical disabilities.
Limitations
Although a growing body of literature supports interventions within the scope of occupational therapy practice to promote social participation and leisure engagement in community-dwelling older adults, the available research has several limitations. First, the majority of outcome measures used to collect information on social participation and leisure engagement were self-report measures, which introduce recall bias. Second, interventions, intervention dosages, and outcome tools varied across studies, limiting the extent to which the data could be synthesized. Third, several included RCTs had small sample sizes. Last, several subthemes did not have enough studies to provide sufficient evidence. Finally, although the interventions described were within the scope of occupational therapy practice, in the majority of studies, the interventionists were not occupational therapy practitioners. Future research addressing these gaps will strengthen the evidence supporting interventions in this area of practice.
Conclusion
Older adults may experience increased social isolation because of the natural losses that occur in this phase of life. Those who experience loneliness and social isolation have an increased risk of other physical and mental health issues. Interventions that support social participation and leisure engagement may mitigate social isolation and loneliness and improve well-being. Strong evidence supports leisure education programs and moderate evidence supports chronic disease self-management programs to enhance leisure engagement. Mixed evidence exists for community-based group programs and electronic gaming interventions to promote social participation.
Occupational therapy practitioners know the value of engaging in meaningful activity in all stages of life and understand the effect of social participation and leisure engagement on older adults’ health and well-being. Practitioners working with community-dwelling older adults are strongly encouraged to integrate effective interventions for social and leisure occupations into routine care for this population.
Supplemental Material
Supplementary material for Occupational Therapy Interventions Supporting Social Participation and Leisure Engagement for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.030627.pdf for Occupational Therapy Interventions Supporting Social Participation and Leisure Engagement for Community-Dwelling Older Adults: A Systematic Review by Stacy Smallfield and Whitney Lucas Molitor in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman, Marian Arbesman, and Beth Hunter for their guidance and support on this project. We also acknowledge Kaitlin LaPlant, who assisted with minor editing. An earlier version of this article was presented at the 2017 AOTA Conference & Expo in Philadelphia.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.