
Abstract
As the population continues to age, health and productive aging are important for occupational therapy research and clinical practice. The purpose of this systematic review was to examine the effectiveness of interventions within the scope of occupational therapy to improve the performance of instrumental activities of daily living (IADLs) for community-dwelling older adults (age 65 and older). This review updates a review conducted in 2012 (Orellano, Colón, & Arbesman, 2012) and highlights the research that has taken place since that review.
The number of older people with disabilities is expected to increase worldwide during the coming decades (Stuck, Beck, & Egger, 2004). Prevalence for older adults with disabilities ranges from 30% of people aged 75–79 to 40% of people aged 85 and older (Winblad, Jääskeläinen, Kivelä, Hiltunen, & Laippala, 2001). Because old age is a period of life associated with increased risk of becoming dependent, the maintenance of independence and the fostering of autonomy have become a high-priority public health issue.
IADL function is important to older adults, and IADL autonomy plays an important role in “successful” aging (Depp & Jeste, 2009). Day-to-day function is often defined clinically as performance of activities of daily living (ADLs) and IADLs. IADLs include activities such as shopping for groceries, making telephone calls, taking medication, and managing money. IADLs are closely related to executive functions such as planning, working memory, attention, problem solving, verbal reasoning, inhibition, mental flexibility, multitasking, and initiation and monitoring of actions (Chan, Shum, Toulopoulou, & Chen, 2008). Additionally, IADLs are significant health indicators that predict mild cognitive impairment, dementia, and mortality (Albert et al., 2011; Sikkes et al., 2011; Xavier, d’Orsi, Sigulem, & Ramos, 2010).
Disability is commonly defined as difficulty carrying out activities that are essential to independent living (Tas, Verhagen, Bierma-Zeinstra, Odding, & Koes, 2007). Disability in the older population is associated with increased health care utilization and related costs (Fried, Ferrucci, Darer, Williamson, & Anderson, 2004), premature death, and impaired quality of life (Freedman et al., 2004; Walter et al., 2001). Impairment in IADLs has been associated with adverse outcomes such as dementia, reduced psychological well-being, greater health care utilization, increased rates of institutionalization, and higher mortality (Naeim, Keeler, & Reuben, 2007; Pérès et al., 2008; Wolinsky et al., 2007). Previous studies have suggested that complex IADLs, such as using the telephone, managing transportation, self-managing medication intake, and handling finances, are strong predictors of dementia (Barberger-Gateau, Dartigues, & Letenneur, 1993).
Although IADLs are known to decline in the course of various neurodegenerative diseases, apparently healthy older adults who live independently in the community also exhibit considerable variability in IADL performance (Burton, Strauss, Hultsch, & Hunter, 2006). IADL functioning in daily life has many components, including physical, emotional, and cognitive, that interact to affect the person over time (Verbrugge & Jette, 1994). Long-term difficulty with IADL performance can lead to more severe impairment, thus lessening the chance of recovery (Willis et al., 2006; Xavier et al., 2010). Lifestyle interventions, medical care, rehabilitation, and social support can contribute to recovery from IADL impairment or, in some cases, reduce its severity (Hardy & Gill, 2004).
Objective
The objective of this review was to systematically search for, assess, and synthesize interventions within the scope of occupational therapy to improve community-dwelling older adults’ IADL performance. The focused question was, What is the evidence for the effect of interventions within the scope of occupational therapy on the performance of selected IADLs for community-dwelling older adults?
Method
This systematic review was supported by the American Occupational Therapy Association (AOTA) as part of the Evidence-Based Practice (EBP) Project (Lieberman & Scheer, 2002). The research question and search terms for the review were developed by the methodology consultant, AOTA staff, and an advisory group in consultation with the review authors. The search terms related to IADLs and study and trial designs are listed in Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). Databases searched included MEDLINE, PsycINFO, CINAHL, and OTseeker. In addition, consolidated information sources, such as the Cochrane Database of Systematic Reviews, were included in the search. Reference lists from articles included in the systematic review were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
Inclusion and Exclusion Criteria
Articles were included if they were peer-reviewed scientific articles, involved participants aged 65 and older who lived in the community, were published in English from January 2008 to December 2016, and examined IADL interventions within the scope of practice of occupational therapy. Studies with participants who had mild cognitive impairment were included, but those examining participants with dementia were not.
Articles were excluded if they were presentations, conference proceedings, non–peer-reviewed research, dissertations, or theses; included participants who were younger than age 65; included older adults residing in long-term care settings; or addressed hospital-based interventions unless they related to transitioning to home. In addition, studies focusing on specific diagnoses that are covered in a previous AOTA Practice Guideline (e.g., stroke, Parkinson’s disease, multiple sclerosis, traumatic brain injury, Alzheimer’s disease) were excluded. Because driving and low vision were well covered in several recent systematic reviews, those findings were not included in this review (Arbesman & Pellerito, 2008; Kua, Korner-Bitensky, Desrosiers, Man-Son-Hing, & Marshall, 2007; Strong, Jutai, Russell-Minda, & Evans, 2008).
AOTA uses levels of evidence modeled on those developed in evidence-based medicine (Lieberman & Scheer, 2002; Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996):
Level I—systematic reviews, meta-analyses, randomized controlled trials (RCTs)
Level II—two groups, nonrandomized studies (e.g., cohort, case control)
Level III—one group, nonrandomized studies (e.g., pretest–posttest)
Level IV—descriptive studies that include analysis of outcomes (e.g., single-subject design, case series)
Level V—case reports and expert opinion that include narrative literature reviews and consensus statements.
Studies included in this review provide Level I, II, and III evidence. Level IV and V evidence was excluded from this review.
Screening and Data Extraction
After literature search results were collected and exact duplicates were removed, the remaining articles were exported in EndNote format (Clarivate Analytics, Philadelphia, PA) by the medical librarian working on the project. The methodologist for the EBP Project did the first review of the search results (citations), eliminating all articles not relevant to the project. The results of this step were conveyed to a team of two reviewers (the authors), who worked together to evaluate all articles at all subsequent stages of the review. Eligibility assessment was performed independently in an unblended standardized manner by the two reviewers, who then compared their choices for articles to include in the review. Disagreements between reviewers were resolved by consensus. Figure 1 depicts the flow of abstracts and articles through the process.
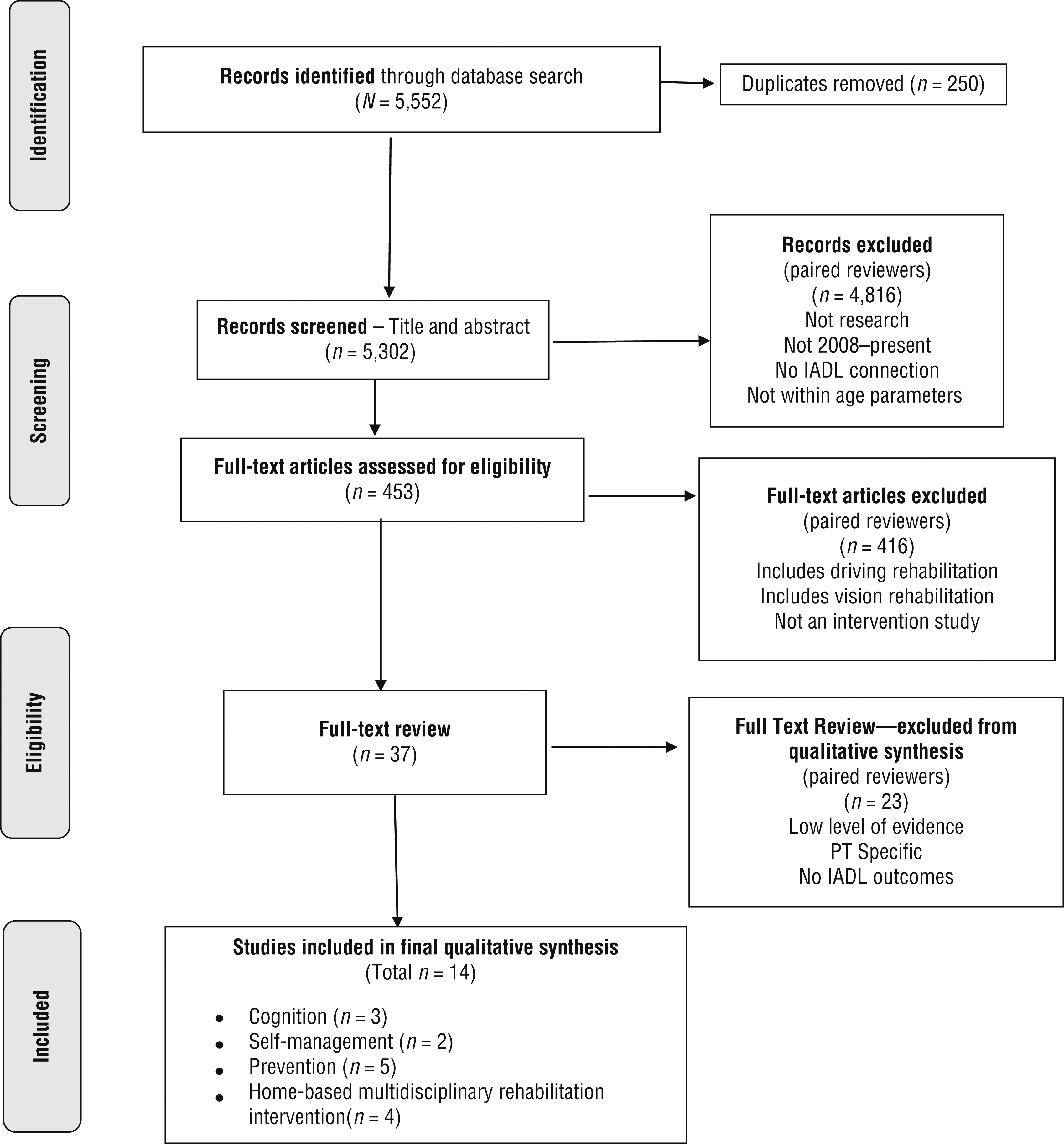
Flow diagram for studies included in the systematic review.
The synthesis entailed a detailed reading of the articles and completion of an evidence table summarizing each study (Supplemental Table 2, online). AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. The risk of bias of individual studies was assessed using the Cochrane risk of bias guidelines (Higgins, Altman, & Sterne, 2011; Supplemental Table 3, online). The articles selected for the final qualitative review were grouped into themes and analyzed and reported in that way.
Strength of Evidence Grading
Analysis of study design, outcomes, and risk of bias determined which studies were assessed as strong or moderate evidence. Strong evidence typically includes two or more well-designed RCTs. Moderate evidence includes at least one RCT or multiple studies of lower level evidence (Level II or III). Moderate evidence also includes inconsistent findings from well-designed projects with a high level of evidence (Level I or II; U.S. Preventive Services Task Force, 2016).
Results
We identified 14 articles for inclusion in the final qualitative synthesis. The articles provide Level I evidence, with the exception of 1 Level III article. Articles were organized into four intervention areas: cognitive, self-management, prevention, and home-based multidisciplinary rehabilitation interventions.
Cognitive Interventions
Three Level I RCTs, providing strong evidence, evaluated cognitive interventions aimed at enhancing IADL performance. The evidence indicates that functional task exercises with a focus on cognitive components (e.g., memory, attention, problem solving) can improve IADL performance. Law, Barnett, Yau, and Gray (2014) evaluated the impact of a 10-wk functional task exercise group facilitated by an occupational therapist compared with a computer-based cognitive training group facilitated by an occupational therapist or occupational therapy assistant. The functional task exercise group included IADL activities with a focus on cognitive components. Participants in the functional task exercise group had significant improvements compared with the cognitive training group in general cognitive functions, memory, executive function, functional status, and everyday problem solving. These improvements were sustained over a 6-mo follow-up period.
Evidence also indicates that interventions focused on memory, reasoning, and speed of processing can have a lasting impact on IADL performance for up to 10 yr. Rebok et al. (2014) conducted a 10-yr follow-up of a Level I study to determine the impact of a cognitive training program for community-dwelling older adults. This intervention included 10 sessions for memory, reasoning, and speed of processing plus an additional four booster sessions at 11 and 35 mo. After 10 yr, participants in the cognitive training program reported significantly fewer difficulties with IADL activities. However, none of the findings indicated that cognitive interventions focused on attention control, prospective memory, and recollection had a significant impact on IADL performance evaluated in a simulated context.
In a Level I study of healthy older adults, McDaniel et al. (2014) evaluated the impact of cognitive training, exercise, or cognitive training combined with exercise on a simulated cooking task. There was no significant change in performance of this task for any of the groups.
Self-Management Interventions
Two studies, 1 Level I and 1 Level III, provide moderate evidence for programs based on Stanford University’s Chronic Disease Self-Management Program (CDSMP; Lorig et al., 2001) to improve levels of activity participation, self-efficacy, and quality of life for adults with multimorbidity (i.e., multiple comorbidities). Garvey, Connolly, Boland, and Smith (2015) conducted an RCT to determine the effectiveness of a 6-wk community-based, occupational therapist–led program based on the CDSMP addressing self-management for older adults with multimorbidity. Sessions addressed a variety of topics such as goal setting, effective communication, staying active, stress management, medication management, and healthy eating. Significant differences were found in IADL performance as measured by the Frenchay Activities Index (Holbrook & Skilbeck, 1983), the Nottingham Extended Activities of Daily Living Scale (Nouri & Lincoln, 1987), and the Satisfaction and Performance domains of the Canadian Occupational Performance Measure (COPM; Law, Baptiste, Opzoomer, Polatajko, & Pollock, 1990).
Dugow and Connolly (2012) conducted a Level III single-group pretest–posttest study with 10 older adults with chronic conditions. The 8-wk multidisciplinary program, also based on the CDSMP, combined individual and group sessions. Significant gains were found in everyday activity participation, motivation, and motor skills as measured by the Model of Human Occupation Screening Tool (Kielhofner et al., 2010) and improvements in self-reported performance and satisfaction on the COPM.
Prevention Interventions
Five Level I RCTs provide strong evidence for interventions to prevent deterioration in IADL performance. Gitlin, Szanton, Huang, and Roth (2014) measured the impact of a 10-wk intervention, Get Busy Get Better: Helping Older Adults Beat the Blues, on several factors including functional disability for older African-Americans with depression. Functional disability involved mobility and IADL and ADL tasks. The intervention was tailored to meet the specific needs, goals, and level of understanding of each participant. Key elements of the intervention were education regarding depression and symptom recognition and strategies for symptom management. Program participants experienced a significant reduction in functional disability.
Gitlin, Winter, Dennis, and Hauck (2008) examined the impact of gender, age, race, and education level on the efficacy of a 6-mo, multicomponent, tailored intervention to address functional impairment, fear of falling, and self-efficacy. The control group received usual care, meaning no care beyond typical medical care. For the intervention group, the primary focus was occupational therapy services for education, problem solving, home modification, and energy conservation training. Overall, this intervention reduced functional difficulties in participants compared with the control group. Analysis of demographic factors revealed that the intervention was most beneficial for women, participants age ≥80 yr, and those with less education. In terms of IADL performance, no significant differences in outcomes were found among demographic groups at 6 mo. At 12 mo, however, differences were identified in level of difficulty with IADLs; White participants reported fewer difficulties than non-White participants. The researchers identified the need for further research to better understand these differences so that more effective interventions can be developed.
Courtney et al. (2012) tested a 24-wk multifaceted transitional care program for older adults transitioning from hospital to home. The program included a tailored exercise program, education regarding health promotion behaviors, a home visit from a registered nurse, and regular telephone follow-up calls for 5 mo. IADL performance was measured using the Lawton IADL Scale (Lawton & Brody, 1969). The intervention resulted in significantly higher levels of IADL performance over the course of the intervention, with the greatest gains occurring in the first month.
Limited findings support the use of a biannual preventive home visit program conducted by nurses or case managers to improve function or psychosocial status. Kono et al. (2012; Level I) examined the impact of an intervention for frail Japanese older adults who were living at home and not receiving formal long-term care services. The intervention included a structured interview assessment of locomotion, daily activities, social contacts, health conditions, and signs of abuse provided in four preventive home visits over 2 yr by community health nurses, care managers, or social workers, who identified concerns and provided recommendations to participants. Although the researchers found no significant differences between the intervention and control groups in terms of function or psychosocial status at the conclusion of the intervention, they did find that control participants who had lower levels of dependency in ADL performance at the start of the intervention experienced less decline in IADL performance and depression than control participants with higher levels of dependency.
Day et al. (2012; Level I) examined a 24-wk Tai Chi program to improve physical function and disability for older adults living in the community and identified as being preclinically disabled. Preclinically disabled was defined as having changed the way in which one walks, climbs stairs, or both but still being able to perform without difficulty. Functional status, including IADL performance, was measured using the Late-Life Function and Disability Instrument (Haley et al., 2002). The intervention group experienced no significant impact on functional performance, level of impairment, or disability status compared with a control group participating in a flexibility and stretching program.
Home-Based Multidisciplinary Rehabilitation Interventions
Four Level I RCTs related to home-based multidisciplinary rehabilitation interventions met the criteria for this review, providing strong evidence for this type of intervention. Tuntland, Aaslund, Espehaug, Forland, and Kjeken (2015) compared a restorative care program led by occupational and physical therapy practitioners with usual care. The theoretical framework of this program was based on the Canadian Model of Occupational Performance and Engagement (Polatajko, Townsend, & Craig, 2007); the COPM was the primary outcome measure used. Intervention was tailored to meet participants’ self-identified needs, and home care personnel were trained in strategies to support engagement in daily activities. Compared with the control group, Performance scores on the COPM were significantly higher at both 3 and 9 mo for the intervention group, and Satisfaction scores were significantly higher at 9 mo.
Lewin et al. (2013; Level I) examined the impact of a multidisciplinary restorative care program incorporating a variety of strategies including task modification, assistive technology, falls prevention, and chronic disease self-management. The restorative care program participants showed less decline in IADL performance at 3 and 12 mo compared with a group receiving usual services.
Zidén, Frändin, and Kreuter (2008; Level I) compared a home rehabilitation program that included supported transition care in addition to standard inpatient rehabilitation with conventional inpatient rehabilitation care for older adults after hip fracture surgery. In the home rehabilitation program, participants and their health care team collaborated to develop an individualized intervention plan and a supported discharge plan. Intervention participants were discharged home with occupational and physical therapists initiating the home rehabilitation program immediately. The home program was typically delivered by the same therapy team seen in the hospital and included other team members as needed. At 1 mo postdischarge, the intervention group had higher levels of engagement and performance in domestic and outdoor activities than the control group, as measured by the Frenchay Activities Index (Holbrook & Skilbeck, 1983).
Fairhall et al. (2012; Level I) studied the impact of a multifactorial interdisciplinary intervention to address mobility, activity, and participation limitations in frail elders. All participants received a 10-session program addressing a client-centered mobility goal delivered by the physical therapist; other disciplines, including occupational therapy, were involved in the intervention as indicated. The intervention group demonstrated improved mobility at 3- and 12-mo follow-up; however, IADL status change did not reach statistical significance.
Discussion
This systematic review updates a previous systematic review related to occupation and activity-based interventions and their impact on IADL performance for older adults living in the community (Orellano et al., 2012) and provides the most current evidence to address this area of interest. This systematic review identified four areas of intervention that have been shown to have a positive impact on either improving IADL performance or slowing decline in performance: cognitive, self-management, prevention, and home-based multidisciplinary rehabilitation interventions.
The 14 studies varied in intervention protocols, involvement of occupational therapy practitioners in the intervention, and inclusion of IADL-specific training as a component of the intervention. Eight of the studies clearly described occupational therapy involvement in the intervention (Dugow & Connolly, 2012; Fairhall et al., 2012; Garvey et al., 2015; Gitlin et al., 2008; Law et al., 2014; Lewin et al., 2013; Tuntland et al., 2015; Zidén et al., 2008), 2 of them on an as-needed basis (Fairhall et al., 2012; Zidén et al., 2008). No interventions explicitly targeted an IADL-focused intervention, although IADLs may have been addressed as part of the occupational therapy interventions in the 8 studies incorporating occupational therapists.
Evidence indicates that interventions tailored to meet the individual needs of older adults can be effective in improving IADL performance or slowing decline in performance (Courtney et al., 2012; Gitlin et al., 2008, 2014; Tuntland et al., 2015; Zidén et al., 2008). These findings support the value of client centeredness in both intervention and research. The studies can provide a model for the development of RCTs that follow established protocols but also allow for client-centered intervention.
The results of this systematic review support the incorporation of cognitive-based interventions for IADL performance (Law et al., 2014; Rebok et al., 2014). However, the impact when IADL performance is assessed using simulated activities is unclear (McDaniel et al., 2014).
Support was found for the use of existing evidence-based programs that fit within the scope of occupational therapy practice to address IADL performance in older adults. The self-management studies included in this systematic review (Dugow & Connolly, 2012; Garvey et al., 2015) both used the Chronic Disease Self-Management Program (Lorig et al., 2001), which resulted in improved activity participation and perceptions of performance and satisfaction with daily activities, including IADLs.
Limitations
Limitations of this systematic review result from limitations in the individual studies’ designs and methods, including small sample sizes, short intervention periods, limited use of standardized assessments, and short follow-up periods. Several studies, particularly related to home-based self-management and restorative programs, were conducted in European countries or Australia; differences in health care funding may limit feasibility in the United States. Many of the studies included multicomponent interventions, so pinpointing the effects of any single intervention may not be possible. Finally, the specific role of occupational therapy was seldom discussed in the included articles on multidisciplinary interventions. None of the studies explicitly looked at helping people maintain or return to IADL function. Instead, the studies looked at IADL performance as one outcome among a number of others.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for occupational therapy practice:
IADL performance is a key indicator of overall performance in older adults. IADL assessment should be incorporated into evaluation of older adults on a routine basis.
Interventions that follow best practices yet are tailored to the specific goals and needs of the client produce better outcomes than standard care.
Standardized programs such as Stanford University’s CDSMP can serve as a foundation for the development of interventions that achieve positive results.
The ability to complete specific IADLs may not reflect older adults’ overall participation in IADLs. Occupational therapy practitioners working with older adults are encouraged in incorporate participation measures into the evaluation process.
This review highlights the importance of client centeredness when developing interventions to improve clients’ perception of their performance and satisfaction with IADL performance and with overall participation in IADLs.
Implications for Occupational Therapy Education
The results of this systematic review have the following implications for occupational therapy education:
Academic programs need to prepare future occupational therapy practitioners not only to collaborate effectively as members of a multidisciplinary team but also to be prepared to advocate for the role of occupational therapy on these teams and to take on leadership roles when able.
Students should be educated both to understand that different health care systems support different practice models and to appreciate the value of international research in providing evidence to support occupational therapy practice, including in the area of older adults’ IADL performance.
Implications for Occupational Therapy Research
The results of this systematic review have the following implications for occupational therapy research:
An ongoing need exists for more research studies that are well designed and occupational therapy driven and that address IADL performance and participation.
Researchers are encouraged to develop and test interventions that focus on the use of IADL performance as an intervention rather than exclusively an outcome.
There is a need for development of more standardized assessment tools that are sensitive to change in IADL performance and levels of participation to further support both practice and research.
Supplemental Material
Supplementary material for Occupational Therapy Interventions to Improve Performance of Instrumental Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.031062.pdf for Occupational Therapy Interventions to Improve Performance of Instrumental Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review by Elizabeth G. Hunter and Pamalyn J. Kearney in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman, program director, AOTA EBP Project, for her guidance and support during the process of this review and Marian Arbesman, methodology consultant for the AOTA EBP Project. The systematic review was supported by AOTA. The authors report no conflicts of interest.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.