
Abstract
Because of age-related changes in sleep patterns, older adults may get less sleep than the recommended amount and experience decreased performance in daytime activities as a result. This article examines the evidence for the effectiveness of interventions within the scope of occupational therapy addressing sleep. Thirteen Level I studies met inclusion criteria and were categorized into three themes: (1) one-to-one single-component interventions, (2) one-to-one multicomponent interventions, and (3) group multicomponent interventions. Strong evidence supports cognitive–behavioral intervention strategies for older adults that include relaxation, sleep hygiene education, problem solving, and physical exercise, among others, delivered one to one or in a group. Routine use of these interventions is recommended.
Sleep is one of the most important occupations humans engage in because it assists in maintaining all aspects of health (National Institutes of Health, 2017). However, roughly a third of the U.S. population reports getting less than the recommended 7–9 hr of sleep each night (American Sleep Foundation, 2017). In fact, the Centers for Disease Control and Prevention (2015) has recognized sleep deprivation as a public health problem with wide-reaching effects. Without adequate sleep, the performance of daytime occupations such as driving, work, leisure, and social participation may be impaired.
The valuable health benefits of sleep remain important to people throughout the lifespan. Although older adults require roughly the same amount of sleep per night as young adults, many have difficulty falling asleep, sleep less deeply, and wake more frequently (Loiselle, Means, & Edinger, 2005; National Institute on Aging [NIA], 2012; Vaz Fragoso & Gill, 2007). Although sleep patterns tend to change as a person ages, aging is often not the sole cause of disrupted sleep (Loiselle et al., 2005; Vaz Fragoso & Gill, 2007). Factors such as chronic health conditions, overall health status, and daytime activity level contribute to sleep quality among older adults. Variations in sleep among older adults may include getting sleepy earlier in the evening and waking earlier than young adults. Older adults with chronic health conditions requiring medication may experience additional sleep disruptions (NIA, 2012). For these reasons, older adults may get less than the recommended amount of sleep at night and may engage in daytime napping.
Poor sleep quality may present in a variety of ways, including inactivity, fatigue, depressed mood, anxiety, and memory difficulties, among others (Chen et al., 2009; Foley, Ancoli-Israel, Britz, & Walsh, 2004). Older adults with poor sleep quality may be at higher risk for nighttime falls and increased use of over-the-counter or prescription sleep medication (NIA, 2012). They report lower quality of life than those without reported sleep difficulties (NIA, 2012).
Sleep medications are used frequently to promote sleep among older adults (Ford et al., 2014). The 1999–2010 National Ambulatory Medical Care Survey findings indicate that older adults are more likely than young adults to have a formal sleep diagnosis and a prescription for sleep medication (Ford et al., 2014). Moreover, use of sleep medications by older adults increases their risk of daytime fatigue, sleepiness, and falls and decreases cognitive function (Diem et al., 2014; Endeshaw, 2015). Additionally, Choi, DiNitto, Marti, and Choi (2017) found that use of sleep medications by older adults as little as one or two occasions per week is related to shorter sleep duration, trouble falling asleep, trouble staying asleep, and increased emergency room visits compared with those who do not use sleep medication. Sleep medication may also contribute to variations in sleep duration among older adults (Choi et al., 2017).
Nonpharmacological interventions to promote sleep among community-dwelling older adults may be a viable alternative. Specifically, interventions within the scope of occupational therapy aimed at health-promoting sleep behaviors may be beneficial. Relaxation techniques, stress management, daily physical activity, education on positive sleep habits, sleep diaries, and cognitive therapy, among other strategies, have been studied as alternatives to sleep medication (Freburger, Callahan, Shreffler, & Mielenz, 2010; Lichstein, Riedel, Wilson, Lester, & Aguillard, 2001; Rybarczyk, DeMarco, DeLaCruz, Lapidos, & Fortner, 2001; Sun, Kang, Wang, & Zeng, 2013). However, there is a dearth of literature describing occupational therapy’s role in addressing sleep (Leland, Marcione, Schepens Niemiec, Kelkar, & Fogelberg, 2014). The purpose of this systematic review was to examine the evidence for the effectiveness of interventions within the scope of occupational therapy for the outcome of improved sleep.
Method
This systematic review is one of six reviews of the literature on productive aging supported by the American Occupational Therapy Association’s (AOTA’s) Evidence-Based Practice (EBP) Project. The findings of the reviews are being incorporated into AOTA’s forthcoming practice guideline on occupational therapy interventions for productive aging. The method for the reviews was specified in advance and documented in a protocol for the review authors.
Search Strategy
Search terms for this systematic review were developed by the methodology consultant to the EBP Project and AOTA staff, in consultation with the review authors, and by an advisory group. The search terms were developed not only to capture pertinent records but also to ensure that the terms relevant to the specific thesaurus of each database were included. Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) lists the search terms related to the population (community-dwelling older adults), interventions, and study designs included in this review. A medical research librarian with experience in completing systematic review searches conducted the search and confirmed and improved the search strategies in the following databases: Cochrane Database of Systematic Reviews, Medline, PsycINFO, CINAHL, and OTseeker.
The methodology consultant for the EBP Project did the first review of the search results, eliminating all records not relevant to the review scope. The review authors examined reference lists in the studies for potential citations and hand searched selected journals to ensure all appropriate records were included.
Eligibility Criteria
Several inclusion and exclusion criteria provided the structure for the quality, type, and years of publication of the literature incorporated into the review. This review included peer-reviewed scientific literature published in English between 1995 and 2015. The intervention approaches examined were within the scope of practice of occupational therapy for older adults with an average age ≥65. Participants were older adults living in the community, a retirement home, or an assisted living facility as well as those in a rehabilitation, subacute, or hospital setting being discharged to home. Studies were also included if participants were older adults with diabetes, arthritis, cardiac disease, or other chronic condition, including mild cognitive impairment and mild Alzheimer’s disease. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Studies were excluded if participants had acute or chronic conditions covered in a previous AOTA Practice Guideline, such as stroke or Alzheimer’s disease. Studies without outcomes related to sleep were also excluded.
AOTA uses standards of evidence modeled on those developed in evidence-based medicine (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). Articles included in the review were rated as follows:
Level I—meta-analyses, systematic reviews, randomized controlled trials (RCTs)
Level II—two-group, nonrandomized studies (e.g., cohort, case-control)
Level III—one-group, nonrandomized studies (e.g., before and after, pretest–posttest)
Level IV—descriptive studies (single-subject design, case series)
Level V—case reports and expert opinions that include narrative literature reviews and consensus statements.
Articles containing Level I, II, and III evidence were considered for inclusion in this review; Level IV evidence was considered only when articles with higher levels of evidence in a given theme were not available. No Level V evidence was considered for inclusion in the review.
Data Extraction
The authors worked collaboratively to evaluate all records throughout the entire review process. Initial review of records was conducted individually. Collaborative discussion between the authors was used to reach a consensus on all articles and to resolve any disagreement. Each article was summarized in an evidence table (see Supplemental Table 2, online) and synthesized by theme. The EBP Project methodology consultant reviewed the evidence table to ensure quality control.
Analysis
Each theme was analyzed for strength of evidence to assist in determining final recommendations for occupational therapy education, practice, and research. Analysis of study design, findings, and risk of bias determined the strength of evidence designation. Number of studies and the strength of evidence they provided were determined in accordance with the U.S. Preventive Services Task Force (2014) recommendations:
Strong evidence indicates consistent results from well-conducted studies, usually at least two RCTs.
Moderate evidence indicates one well-conducted RCT or two or more studies with lower levels of evidence. Some inconsistency of findings across individual well-conducted studies could preclude a classification of strong evidence and result in a designation of moderate evidence.
Limited evidence indicates few studies, flaws in the available studies, and some inconsistency in findings across individual studies.
Mixed evidence indicates that the findings were inconsistent across studies in a given category.
Insufficient evidence indicates that the number and quality of studies are too limited to make any clear recommendation.
Results
Figure 1 displays a flow diagram of record selection. The authors identified 13 articles, all providing Level I evidence, for inclusion in the final qualitative synthesis and synthesized the results. One article had findings applicable to two themes and therefore was included in the evidence table and synthesis under both.
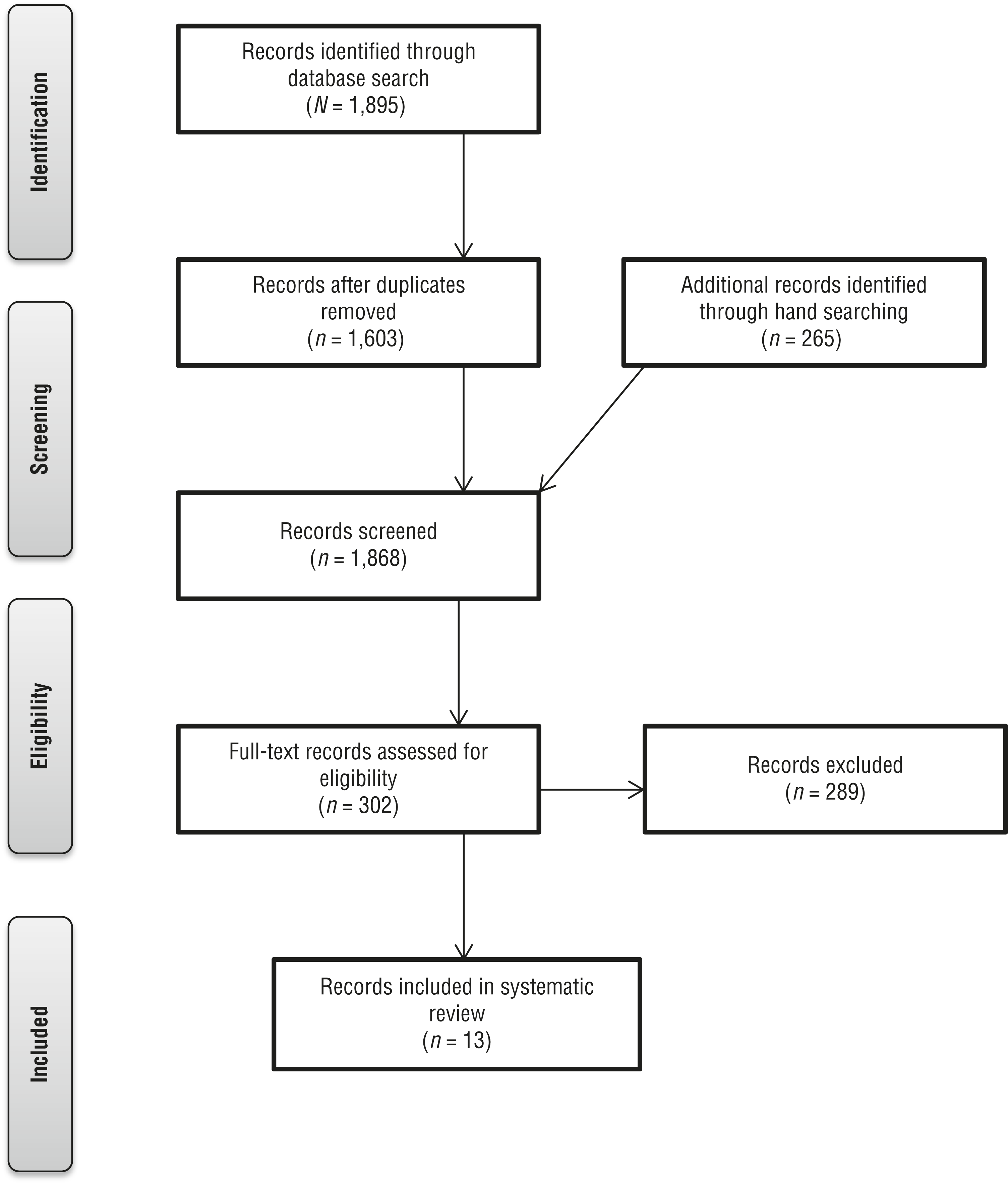
Flow diagram for studies included in the systematic review.
Risk of Bias
Each study was individually assessed for risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias on a scale of low, high, or unclear as described in the Cochrane risk of bias guidelines (Higgins, Altman, & Sterne, 2011). During the rating process, the authors worked collaboratively to reach consensus in each category of bias assessed. Supplemental Table 3 (online) displays the results of the risk-of-bias evaluation of all articles included this review.
Outcome Measures
Outcome measures used in the studies incorporated subjective measures of quantity and quality of sleep (e.g., sleep diaries or logs, questionnaires, standardized sleep assessments such as the Pittsburgh Sleep Quality Index; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). Few studies included in this review used objective measures of sleep, such as actigraphy or polysomnography, in addition to subjective outcome measures.
Interventions to Enhance Sleep
The 13 studies included in the review used cognitive–behavioral intervention strategies. Cognitive–behavioral interventions assist people to become aware of distorted thinking or maladaptive behaviors and to learn alternative strategies and develop adaptive skills (Ikiugu, 2007). The cognitive–behavioral interventions discussed in this review should not be confused with cognitive–behavioral therapy, which is one type of cognitive–behavioral intervention. Specific cognitive–behavioral strategies described in the studies in this review include relaxation techniques (e.g., progressive muscle relaxation, meditation, guided imagery), health education, sleep hygiene education, sleep diaries, group problem solving, computerized training, and didactic class sessions. These strategies were used either individually or as part of multicomponent interventions and were delivered either one to one or in a group format. The articles were categorized into three themes according to intervention design: (1) one-to-one single-component interventions, (2) one-to-one multicomponent interventions, and (3) group multicomponent interventions. No studies examined a single-component intervention offered in a group format.
One-to-One Single-Component Interventions.
Three Level I articles described improved sleep outcomes with use of a single-component cognitive–behavioral intervention provided in a one-to-one format (Brenes et al., 2012; Buysse et al., 2011; Haimov & Shatil, 2013). Brenes et al. (2012) compared a cognitive–behavioral intervention delivered by telephone guided by an eight-chapter workbook with an information-only control condition for older adults with anxiety disorder. The intervention group experienced a significant reduction in self-rated insomnia (a general term used to describe the inability to sleep) at postintervention; however, this reduction was not maintained at 6-mo follow-up.
Buysse et al. (2011) studied the use of a brief behavioral treatment delivered in two intervention sessions and two telephone calls for older adults with insomnia compared with an information-only control condition. At the 4-wk posttest, the intervention group showed significant differences on specific sleep outcomes of later bedtimes, improved sleep quality, improved sleep latency, delayed waking after sleep onset, and increased sleep efficiency. Sleep quality is a self-reported measure of sleep, whereas sleep latency is the time it takes to fall asleep. Sleep efficiency is the total sleep time compared with the total time spent in bed.
Haimov and Shatil (2013) also studied older adults with insomnia. They found positive results for sleep latency, efficiency, waking after sleep, and number of wakings after an 8-wk, individualized, cognitive computerized training program compared with low-cognitive-demand computerized tasks.
Three well-conducted Level I studies provided consistent and significant findings for single-component cognitive–behavioral interventions delivered individually to community-dwelling older adults with insomnia. Thus, the evidence is strong for the effectiveness of these interventions in enhancing sleep outcomes.
One-to-One Multicomponent Interventions.
Three Level I studies found improved sleep outcomes with use of multicomponent cognitive–behavioral interventions provided in a one-to-one format (Lichstein et al., 2001; McCrae, McGovern, Lukefahr, & Stripling, 2007; McCurry, Logsdon, Vitiello, & Teri, 1998). Lichstein et al. (2001) conducted a three-arm RCT with older adults with insomnia. They found that two 6-wk interventions, one of individual sleep hygiene education combined with progressive relaxation and the other of sleep hygiene education, identification of sleep goals, and conforming to a sleep schedule, were effective in reducing self-reported insomnia compared with a placebo control consisting of a quasi-desensitization bedtime routine. Similarly, McCrae et al. (2007) found that 9 of 11 participants with self-reported sleep difficulty receiving sleep hygiene education, progressive relaxation, and sleep restriction in two individual sessions and two follow-up telephone calls no longer met insomnia criteria; only 3 of 9 control group participants, who received sleep and aging education, no longer met insomnia criteria.
McCurry et al. (1998) completed a three-arm RCT of an intervention for caregivers of people with dementia consisting of sleep hygiene, stimulus control, sleep compression, relaxation, use of a sleep diary, and education about dementia and caregiving. They compared delivery of the intervention in a one-to-one format over 4 wk, delivery in a group format over 6 wk, and a no-intervention control condition. They found significant improvements in sleep quality for both intervention groups compared with the control group. No difference was found between the one-to-one and group delivery format for the outcome of sleep quality. However, a small sample size limits the generalizability of these results.
These 3 well-conducted, Level I studies demonstrated consistent findings in support of multicomponent cognitive–behavioral interventions delivered individually to community-dwelling older adults with insomnia to improve sleep outcomes. Therefore, strong evidence supports this intervention strategy to decrease insomnia.
Group Multicomponent Interventions.
Eight Level I articles reporting on 7 studies described improved sleep outcomes with the use of multicomponent cognitive–behavioral interventions provided in a group format (Chen et al., 2009; Freburger et al., 2010; McCurry et al., 1998; Morin, Colecchi, Stone, Sood, & Brink, 1999; Rybarczyk et al., 2001, 2005; Sun et al., 2013; Vitiello, Rybarczyk, Von Korff, & Stepanski, 2009). Morin et al. (1999) compared eight weekly sessions of small-group cognitive therapy plus sleep hygiene education with interventions based on drug therapy or drug therapy plus cognitive therapy. They found that the cognitive therapy, either with or without drug therapy, was more effective than drug therapy alone at reducing insomnia. Participants were more satisfied with therapy when it included the group cognitive therapy sessions.
McCurry et al. (1998), as described previously, compared a 4-wk multicomponent intervention delivered in a one-to-one format with the same intervention delivered in a 6-wk group format and a no-intervention control condition. They found significant improvements in sleep quality for both intervention groups compared with the control group, with no difference between the one-to-one and group delivery format.
Rybarczyk et al. (2005) and Vitiello et al. (2009) compared eight sessions of cognitive–behavioral interventions consisting of didactic presentations, question-and-answer sessions, sleep log review, and group problem solving delivered in a classroom setting to participants with osteoarthritis with a control condition of eight sessions of stress management and wellness training. They found significant differences on 8 of 10 sleep measures, including improved sleep latency, waking after sleep onset, and sleep efficiency favoring the intervention group.
Sun et al. (2013) examined the effectiveness of self-relaxation training that included progressive muscle relaxation, meditation, and sleep hygiene education compared with a control condition of sleep hygiene education. Significant group differences favored the self-relaxation and meditation training and lasted throughout the 1-yr duration of the study.
Three of the articles describing a group-based multicomponent approach to enhance sleep performance included relaxation as one component of the intervention (Chen et al., 2009; Freburger et al., 2010; Rybarczyk et al., 2001). All 3 studies found significant differences in sleep quality compared with a control group.
Freburger et al. (2010) conducted a large RCT for community-dwelling older adults with arthritis using an 8-wk arthritis exercise program. The program consisted of land-based exercise, education on arthritis self-management, activities to promote social interaction, and relaxation techniques delivered twice weekly. They found short-term positive effects on improved sleep quality related to waking up tired and waking up at night for the intervention group compared with a wait-list control group. Effects were not maintained at 3- or 6-mo follow-up, but it is unclear whether the participants continued to exercise after the 8-wk study period.
Chen et al. (2009) conducted a large RCT in Taiwan with community-dwelling older adults. They found that a 6-mo program including yoga, gentle stretching, meditation, and relaxation interventions delivered 3×/wk produced significantly improved subjective sleep quality, faster sleep latency, and less daytime dysfunction at the 3- and 6-mo posttests compared with a wait-list control group. The difference in sleep quality was maintained over the 1-yr study period.
Finally, Rybarczyk et al. (2001) conducted a large RCT with community-dwelling older adults who had at least one chronic illness. They found that eight sessions of a mind–body wellness intervention that included classroom training sessions on mind–body relationships, relaxation training, cognitive restructuring, problem solving, communication, behavioral treatment of insomnia, nutrition, and exercise resulted in decreased sleep difficulties compared with the wait-list control condition. These benefits were maintained at 1-yr follow-up.
Eight high-quality Level I studies with low risk of bias provide strong evidence for the effectiveness of multicomponent cognitive–behavioral interventions delivered in a group format to community-dwelling older adults with insomnia. Although the specific intervention strategies varied across studies, multicomponent interventions that included self-relaxation, meditation, physical exercise, sleep hygiene education, sleep diaries, and cognitive therapy were found to be effective in improving sleep quality, sleep latency, subjective satisfaction regarding sleep, and sleep efficiency.
Discussion
This systematic review examined the effectiveness of interventions within the scope of occupational therapy to improve sleep in community-dwelling older adults. Strong evidence was found for one-to-one single-component interventions, one-to-one multicomponent interventions, and group multicomponent interventions. These interventions should be routinely offered to community-dwelling older adults who have difficulties with sleep. Single-component interventions included cognitive–behavioral strategies delivered in person, over the telephone, or on the computer (Brenes et al., 2012; Buysse et al., 2011; Haimov & Shatil, 2013). Multicomponent interventions incorporated specific strategies including relaxation training, physical exercise, meditation, sleep-related goal setting, sleep hygiene education, use of a sleep journal, cognitive therapy, and group problem-solving sessions (Chen et al., 2009; Freburger et al., 2010; McCurry et al., 1998; Morin et al., 1999; Rybarczyk et al., 2001, 2005; Sun et al., 2013; Vitiello et al., 2009).
Implications for Occupational Therapy Education
Sleep is an important occupation that should be included in occupational therapy professional education programs. The role of occupational therapy with older adults in community-based settings is expected to increase, necessitating skills related to this method of service delivery (Lamb & Metzler, 2014). Preparing future practitioners to address the needs of older adults living in the community, including sleep, should be a focus of educational programs. On the basis of the results of this review, occupational therapy curricula should include knowledge and skill training related to sleep assessment and intervention, including the following:
The importance of sleep as an area of occupation that should be addressed in occupational therapy practice
Knowledge of the sleep cycle, sleep disorders, and health conditions related to impaired sleep that limit performance in daytime occupations
Assessment of sleep using formal and informal measurement tools
Cognitive–behavioral interventions, including cognitive restructuring, stress management, relaxation strategies, problem solving, integration of physical activity and exercise into daily routines, and sleep hygiene education
Training in leading group intervention and delivering multicomponent interventions to maximize outcomes.
Implications for Occupational Therapy Research
Occupational therapy has the potential to play a significant role in enhancing sleep for community-dwelling older adults. Occupational therapy researchers need to continue to develop the evidence base for interventions aimed at improving sleep outcomes. Further research regarding these interventions and the link between improvement of sleep and daytime activity is critical to support occupational therapy’s role in this area of practice. To strengthen current research in this area, occupational therapy practitioners should be used as study interventionists, and consensus across research studies should be established regarding
Intervention strategies used in multicomponent intervention,
Intervention dosages (frequency and duration of intervention), and
Outcome measures used to determine the result of the intervention on sleep.
Increased consistency across research will enable more robust data synthesis and meta-analysis of research outcomes and more effectively guide practitioners in delivering evidence-based interventions enhancing sleep to community-dwelling older adults.
Implications for Occupational Therapy Practice
On the basis of the results of this review, interventions recommended as part of routine occupational therapy services to community-dwelling older adults who identify issues with sleep include
One-to-one single-component cognitive–behavioral interventions including cognitive computer training or educational sessions;
One-to-one multicomponent cognitive–behavioral interventions including sleep hygiene education, progressive relaxation, goal setting, development of a sleep schedule, and use of a sleep diary; and
Group multicomponent interventions including self-relaxation, meditation, physical exercise, sleep-related goal setting, sleep hygiene education, use of a sleep journal, group problem-solving sessions, and cognitive therapy.
Limitations
Although the body of literature supporting interventions within the scope of occupational therapy practice to enhance sleep is growing, limitations exist that should be addressed in future research. A large amount of heterogeneity characterizes the studies included in this review. The combinations used in multicomponent interventions varied greatly, as did the intervention dosages and outcome tools used to measure effectiveness. This heterogeneity limits the extent to which the data can be synthesized. Moreover, although the participants studied were community-dwelling older adults, there was some heterogeneity in participants across studies, so it is not clear whether these approaches can be generalized to other, nonstudied populations.
Additionally, the majority of the outcome measures were subjective rather than objective measures of sleep, which limits the rigor and precision of the data. The use of objective measures may strengthen study outcomes. Finally, although the interventions described in these studies are within the scope of occupational therapy practice, the interventionists were not occupational therapy practitioners. Future research addressing these gaps will strengthen the evidence that supports interventions in this area of practice.
Conclusion
Because of age-related changes in sleep patterns, older adults may get less than the recommended 7–9 hr of sleep per night and may experience decreased performance in daytime activities as a result. Strong evidence supports the use of a variety of cognitive–behavioral strategies delivered in a one-to-one or group format. Occupational therapy practitioners working with community-dwelling older adults are strongly encouraged to address this important occupation by integrating these interventions into routine care when clients’ participation in daytime activities is impaired as the result of sleep disturbances.
Supplemental Material
Supplementary material for Occupational Therapy Interventions Addressing Sleep for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.031211.pdf for Occupational Therapy Interventions Addressing Sleep for Community-Dwelling Older Adults: A Systematic Review by Stacy Smallfield and Whitney Lucas Molitor in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman, Marian Arbesman, and Beth Hunter for their guidance and support on this project, as well as Kaitlin LaPlant, who assisted with minor editing. An earlier version of this work was presented at the 2017 AOTA Conference & Expo in Philadelphia.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.