
Abstract
More than 95% of the older adult population live in the community (Administration on Aging, 2016). Preserving the ability to perform activities of daily living (ADLs) is fundamental for older adults to live an independent life. Becoming dependent on others to complete daily activities is associated with more doctor visits and longer hospitalization (Millán-Calenti et al., 2010). In particular, such dependence is a significant contributing factor in long-term nursing home placements (Gaugler, Duval, Anderson, & Kane, 2007) and escalating health care costs (Guralnik, Alecxih, Branch, & Wiener, 2002). Identifying and implementing effective interventions to help community-dwelling older adults maintain ADL independence is imperative to ease the potential care burden on families and the nation and, more important, to support older adults to live life to the fullest.
Older adults experience ADL disability through two pathways: (1) a catastrophic event, such as a hip fracture, or (2) progressive decline (Ferrucci et al., 1996). Along the two pathways, occupational therapy practitioners in health care and community settings have opportunities to disrupt the disablement process and maximize older adults’ ADL independence. This systematic review was conducted to assist practitioners in making evidence-based decisions on selecting effective interventions to improve ADL outcomes for community-dwelling older adults. The research question was, What is the evidence for the effect of interventions within the scope of occupational therapy to improve the performance of ADLs in community-dwelling older adults?
Method
This systematic review is one of six reviews on productive aging supported by the American Occupational Therapy Association’s (AOTA’s) Evidence-Based Practice (EBP) Project. The methods for the review were specified in advance and documented in a protocol for review authors.
Literature Search
Search terms were developed by a methodology consultant to the EBP Project and AOTA staff in consultation with the review authors and an advisory group (for key search terms, see Supplemental Table 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). An experienced medical research librarian conducted the literature search in the following electronic databases: CINAHL, Cochrane Database of Systematic Reviews, MEDLINE, OTseeker, and PsycINFO. The search duration of published articles was set from 1995 to 2015. The publication language was limited to English. The methodology consultant perused the initial search results and removed irrelevant citations before passing the results on to the review authors. The consultant also provided additional records from related EBP Project reviews on productive aging that might be relevant to this review.
Screening and Selection
Each citation and abstract was independently reviewed by two review authors. Discord was resolved by consultation with the third review author. A study was included if all of the following criteria were met:
The average age of study participants was ≥65 yr.
The level of evidence was Level I (randomized controlled trial), Level II (nonrandomized study with two or more groups), or Level III (one-group nonrandomized study).
Performance of basic ADLs was reported as an outcome.
A study was excluded if it had any of the following characteristics:
It was a dissertation, thesis, or conference presentation or proceedings.
The intervention content was outside the scope of occupational therapy practice.
Participants lived in a skilled nursing facility.
The study population, including people with stroke, Parkinson’s disease, multiple sclerosis, traumatic brain injury, or moderate or severe Alzheimer’s disease, was included in another AOTA EBP Project systematic review.
Participants were recruited in a health care setting but no outcomes were measured after they were discharged to home.
The outcomes were a mix of ADLs and instrumental ADLs (IADLs).
The study was a systematic review or meta-analysis. However, studies included in identified systematic reviews and meta-analyses were individually reviewed for eligibility.
The full text of studies that passed the initial title and abstract screening was then obtained for further review using the same criteria.
Risk-of-Bias Assessment and Data Extraction
The methodology of each eligible study was independently reviewed by two review authors using the methods described by Higgins, Altman, and Sterne (2011). The risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias was evaluated and rated as high, low, or unclear. Discord on classification of a study was resolved by consultation with the third review author. Data were extracted using an evidence table summarizing the methods and findings of the studies. One author extracted the data, and another author checked the extracted data. Multiple publications from the same trial were entered as 1 study in the evidence table.
Results
We screened 1,383 records and identified 43 eligible studies in 50 publications (see Figure 1 for a chart of the flow through the selection process). Of these, 34 studies provide Level I evidence, 4 provide Level II evidence, and 5 provide Level III evidence. The evidence is summarized in Supplemental Table 2 (online).
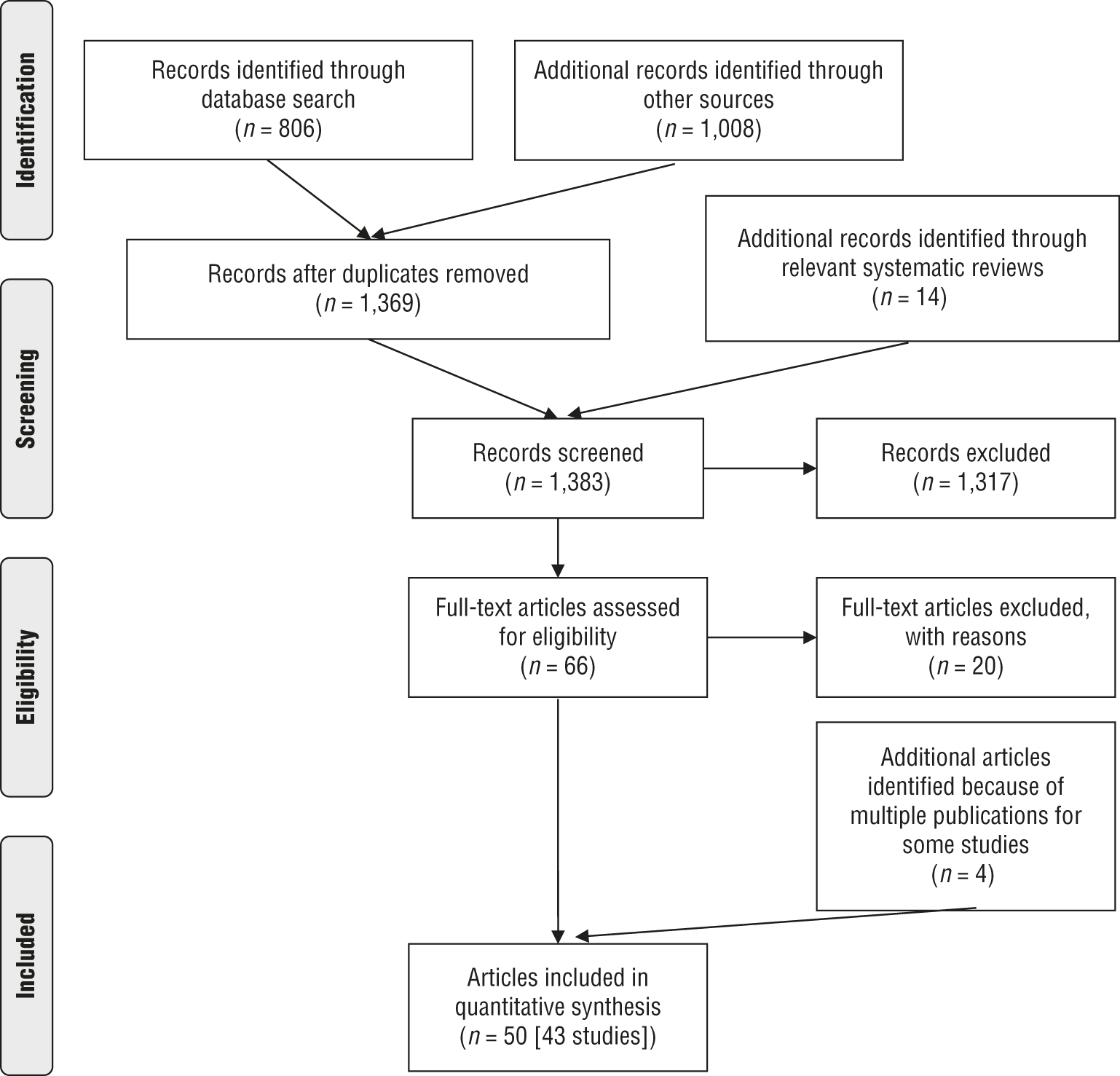
Flow diagram for studies included in the systematic review.
Risk of Bias
Results of the risk-of-bias rating are presented in Supplemental Table 3 (online). A moderate selection bias existed among the selected studies; 19 of the 34 Level I studies lacked clarification on allocation concealment. Performance and detection bias were high. Regarding performance bias, 36 studies (84%) were rated as high risk because study participants and personnel were not blinded to the study. Regarding detection bias, 22 studies (51%) were rated as high risk because the outcome assessors were not blinded. Attrition bias was low to moderate, and reporting bias was low.
Summary of Study Characteristics
Study characteristics were summarized by study population, mean age, and intervention (Table 1). On the basis of their participant recruitment inclusion and exclusion criteria, the 43 reviewed studies were categorized by population, as follows:
Older adults without noticeable ADL difficulty (n = 1,341; 7 studies)
Older adults with ADL difficulty (n = 2,403; 16 studies)
Older adults who were receiving restorative home care services (n = 1,487; 2 studies)
Frail older adults (n = 1,019; 7 studies)
Older adults discharged to home from a hospital setting (n = 1,055; 7 studies)
Older adults with a history of hip fracture (n = 290; 4 studies).
The mean age of study participants was in the 70s or 80s, except 1 study, in which the mean age was in the 60s.
Study Characteristics, by Population and Intervention Approach
Note. ADL = activities of daily living.
Six major intervention approaches were identified: physical exercise (19 studies), home visits or home-based intervention (7 studies), multicomponent programs (7 studies), additional occupational therapy services (2 studies), inpatient therapy (4 studies), and multidisciplinary team (4 studies). Physical exercise approaches included unimodal exercise programs, such as task-specific resistance exercise (Alexander et al., 2001), and multimodal exercise programs, such as a combination of stretching, muscle strengthening, and balance exercises (Ohtake, Morikagi, Suzuki, Kanoya, & Sato, 2013).
Examples of home visits or home-based intervention include in-home assessments and recommendations (Kono, Kai, Sakato, Harker, & Rubenstein, 2004); single-component programs, such as home modification (Fänge & Iwarsson, 2005); or multicomponent programs, such as a combination of education in problem-solving and energy-conserving techniques, home modification, and exercise (Gitlin et al., 2006). The multicomponent programs identified in this review were not home-based interventions, for example, a comprehensive geriatric assessment followed by individualized recommendations or resources referral (Li, Chen, Li, Wang, & Wu, 2010) and standard programs such as Lifestyle Redesign® (Clark et al., 1997).
Examples of approaches using additional occupational therapy services include programs offering extra occupational therapy consultation in addition to usual community occupational therapy services (Borrows & Holland, 2013) and having a nurse follow through and carry out recommendations made by occupational therapists (Liddle et al., 1996). Inpatient therapy approaches were used in an acute care setting (Wressle et al., 2006), a rehabilitation department (Di Monaco et al., 2008), and an emergency department (Hendriksen & Harrison, 2001); these studies followed up ADL outcomes after participants were discharged to home. The multidisciplinary team approach included intervention content that was within the practice scope of occupational therapy, such as a multidisciplinary fall prevention program (Vind, Andersen, Pedersen, Joergensen, & Schwarz, 2010).
A great of variety of ADL outcome measures were used in the studies. The most frequently reported measure was the Barthel Index or Modified Barthel Index (Mahoney & Barthel, 1965; Shah, Vanclay, & Cooper, 1989), used in 12 studies. The remaining studies rarely used the same outcome measure. Examples of other ADL measures include the FIM® (Keith, Granger, Hamilton, & Sherwin, 1987), the Katz Index of ADL (Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963), and the Klein–Bell ADL Scale (Klein & Bell, 1982). Some authors used study-specific ADL items or ADL questionnaires (Luukinen et al., 2006; Wressle et al., 2006).
Summary of Key Findings
Findings of the reviewed studies are summarized in Supplemental Table 2. In this section, we summarize the results of 2 or more studies that examined a similar intervention approach by study population. The net benefit (strength of evidence) was graded as high, moderate, or low on the basis of the grade definitions of the U.S. Preventive Services Task Force (2014); net benefit is defined as benefit minus harm of an intervention approach. High indicates that the available evidence includes consistent results from well-designed, well-conducted studies and is unlikely to be strongly affected by the results of future studies. Moderate indicates that the available evidence is sufficient to determine the effects; however, confidence in the estimate is constrained by factors such as the number, size, or quality of individual studies; lack of coherence in the chain of evidence; or limited generalizability. The magnitude or direction of the observed effect could change when more information becomes available. Low indicates that available evidence is insufficient to assess effects because of the limited number of studies, significant flaws in study design or methods, or inconsistency of findings across studies. More information is needed to estimate the effects.
Older Adults Without Noticeable ADL Difficulty
Four studies examined the effect of physical exercise. One Level I study (Ohtake et al., 2013) and 1 Level III study (Yokoya, Demura, & Sato, 2009) examined multimodal exercise. One Level II study (Kolbe-Alexander, Lambert, & Charlton, 2006) and 1 Level III study (Wallmann, Schuerman, Kruskall, & Alpert, 2009) examined upper and lower extremity exercise. None of these studies showed a significant difference between the intervention and control groups or from baseline to posttest. Overall, these studies did not show additional benefits of exercise for ADL performance in older adults who did not have noticeable ADL difficulty.
Three Level I studies examined the effect of multicomponent programs. One study showed that the Lifestyle Redesign program did not improve short-term or long-term ADL performance compared with a social control group and a no-intervention control group (Clark et al., 1997, 2001). Another study compared a comprehensive geriatric assessment followed by an individualized intervention with a screening-only control group and did not find an improvement in ADLs (Li et al., 2010). The third study compared a specialized health enhancement program (evidence-based exercise class and chronic disease self-management class) with an attention control condition. Among participants who did not have ADL disability at baseline, the results showed that the attention control participants were more likely to develop ADL disability (Phelan, Williams, Penninx, LoGerfo, & Leveille, 2004). Because of heterogeneity in multicomponent program content and inconsistent findings across studies, the benefit of using multicomponent programs to improve ADL outcomes in older adults without noticeable ADL difficulty was low.
Older Adults With ADL Difficulty
Three Level I studies examined the effect of multimodal exercise compared with home flexibility exercise, mobility activity, or exercise education, and all showed nonsignificant findings (Binder et al., 2002; Foley, Hillier, & Barnard, 2011; Timonen et al., 2006). These studies suggest no additional benefits of multimodal exercise for improving ADL performance in older adults with ADL difficulty compared with other types of exercise or exercise education.
In addition, 1 Level I study examined the effect of chair or bed rising resistance exercise (Alexander et al., 2001), and 1 Level III study examined the effect of a walking club (Taylor et al., 2003). Both showed a positive effect on ADL outcomes. The benefit of using task-specific exercise to improve ADL outcomes in older adults with ADL difficulty was moderate.
Six studies examined the effectiveness of home visits or home-based intervention, and 5 of them demonstrated a significant improvement in ADL performance: 3 Level I studies (Gitlin et al., 2006; Kono et al., 2004; Szanton et al., 2011), 1 Level II study (Zingmark & Bernspång, 2011), and 1 Level III study (Gitlin, Miller, & Boyce, 1999). The interventions in these studies included home visits and an offer of recommendations by public health nurses (Kono et al., 2004); home visits and multicomponent intervention by occupational therapists and physical therapists (Gitlin et al., 2006); home visits and multiprofessional support from an occupational therapist, a nurse, and a repair person (Szanton et al., 2011); and home visits by occupational therapists to address bathing-related performance or to conduct a bathroom modification program (Gitlin et al., 1999; Zingmark & Bernspång, 2011). An additional Level III study did not show a significant change in ADL scores but found that fewer clients were dependent in bathing after housing adaptions (Fänge & Iwarsson, 2005). Overall, the benefit of using home visits or home-based intervention to improve ADL outcomes in older adults with ADL difficulty was high.
Two studies examined the effect of a multicomponent program to promote active engagement through daily activities (Lewin et al., 2013, Level I; Lewin & Vandermeulen, 2010, Level II). However, these 2 studies reported conflicting findings. Intervention contamination might have occurred in the Level I study (Lewin et al., 2013). Because of the contamination concern, the benefit of using this multicomponent program to improve ADL outcomes in older adults with ADL difficulty was low.
One Level I study examined the effect of 1.5 hr of occupational therapy evaluation and consultation in addition to usual community occupational therapy services (Borrows & Holland, 2013). Another Level I study examined the effect of implementing home assessment recommendations suggested by occupational therapists versus no follow through on the recommendations (Liddle et al., 1996). Both studies showed nonsignificant findings regarding provision of opportunities for additional occupational therapy consultation and implementation. Because the intervention content was different in the 2 studies, the benefit of adding occupational therapy related services to improve the ADL outcome was low.
Older Adults Receiving Restorative Home Care Services
Two Level I studies examined the multidisciplinary approach of restorative home care for older adults who were at risk of institutionalization or functional decline (Senior et al., 2014; Tinetti et al., 2002). Although 1 study showed a marginally significant intervention effect on self-care scores (Tinetti et al., 2002), neither study suggests that such home care services significantly improve ADLs compared with usual care. The benefit of using restorative home care services to improve ADL outcomes was low because the number of related studies included in this review was limited and service content and duration were different in the 2 studies.
Frail Older Adults
Six Level I studies examined the effects of physical exercise compared with no intervention, social groups, or usual care (Chin A Paw, de Jong, Schouten, Hiddink, & Kok, 2001; Giné-Garriga et al., 2010; Luukinen et al., 2006; Rydwik, Frändin, & Akner, 2010; Rydwik, Lammes, Frändin, & Akner, 2008; Sato, Kaneda, Wakabayashi, & Nomura, 2007, 2009; Westhoff, Stemmerik, & Boshuizen, 2000). Of these studies, 3 found significant ADL improvements at exercise completion, but the results from long-term follow-ups were inconsistent (Giné-Garriga et al., 2010; Sato et al., 2009; Westhoff et al., 2000). Overall, the benefit of using exercise to improve ADL outcomes in frail older adults was moderate.
Older Adults Discharged to Home From a Hospital Setting
Two Level I studies compared the effects of multimodal exercise with placebo motor activity or usual hospital care (Hauer, Pfisterer, Schuler, Bärtsch, & Oster, 2003; Hauer et al., 2001; Siebens, Aronow, Edwards, & Ghasemi, 2000). Both studies showed nonsignificant findings. The benefit of using physical exercise to improve ADL outcomes in older adults discharged to home from a hospital setting was low because of the limited number of related studies included in this review.
Three studies examined the effects of inpatient rehabilitation programs. Two Level I studies examined the effect of inpatient occupational therapy intervention compared with no occupational therapy (Hendriksen & Harrison, 2001; Wressle et al., 2006) but showed conflicting results. One Level II study compared an inpatient multicomponent program that included one home visit by an occupational therapist with usual care (Di Monaco et al., 2008) and found no group differences after the intervention. The benefit of using an inpatient rehabilitation program to improve ADL outcomes was low because of heterogeneity in the intervention programs.
Older Adults With a History of Hip Fracture
One Level I study compared lower limb progressive resistance exercise with no intervention and found that exercise improved function in transferring from and to bed (Edgren et al., 2012). Another Level I study compared the ProMo program (multimodal exercise) plus standard care with a written home exercise program and found no group differences (Edgren et al., 2015). The benefit of using exercise to improve ADL outcomes in older adults with a history of hip fracture was low because of the limited number of available studies and the difference in the selection of comparison group between the studies.
Discussion
This systematic review examined interventions within the scope of occupational therapy to maintain or improve ADL performance in community-dwelling older adults. High benefit was found of using home visits or home-based intervention to improve basic ADL performance in older adults who experienced ADL difficulty. Physical exercise, a common intervention approach identified in this review, showed moderate benefit in improving ADLs for frail older adults, particularly task-specific exercise. However, the benefit of exercise to improve ADL performance for older adults discharged to home from a health care setting or with a history of hip fracture was low. In addition, the benefit of using multicomponent programs, restorative home care services, additional occupational therapy services, or inpatient rehabilitation programs to improve ADL performance was low. The low benefit is attributable to the limited number of studies for each intervention approach and the heterogeneity in intervention content.
The ability to perform ADLs gradually declines after age 50 (Hayase et al., 2004), with difficulty in IADLs preceding difficulty in ADLs (Kingston et al., 2012). Our review indicates that studies that recruited older adults with ADL difficulty generally had a higher mean age than studies that included older adults without noticeable ADL difficulty. More than one-third of the studies included in this review are in the category of older adults with ADL difficulty, reflecting great research interest in this population.
Being physically active is a protective factor for late-life ADL disability (Tak, Kuiper, Chorus, & Hopman-Rock, 2013). Physical exercise is the most common of the six intervention approaches identified in this review. This review identified a moderate benefit of exercise to improve ADL performance for frail older adults and older adults with ADL difficulty. Among the variety of physical exercise programs reviewed, task-specific or task-oriented exercise that linked muscle groups with ADL tasks was more beneficial than structured, repetitive raw exercise movements (Alexander et al., 2001). Prior studies have shown similar findings (Liu, Shiroy, Jones, & Clark, 2014; Liu, Xu, Keith, & Clark, 2017). Therefore, occupational therapy practitioners may use physical exercise, particularly task-specific or task-oriented exercise, for the purpose of improving ADL performance in older adults who are at risk of losing independence at home.
For older adults with no noticeable ADL difficulty, several reasons may account for some of the nonsignificant findings observed in the reviewed studies. The intervention duration in studies of older adults without noticeable ADL difficulty often lasted less than 6 mo, which might be too short to show the maintenance effect of physical exercise. Also, the primary interest in many exercise studies was physical benefits, such as muscle strength or balance, so these studies might not be adequately powered to identify an effect on ADL outcomes. Another reason is the lack of sensitive measures of ADL performance for older adults with high function; therefore, these studies tend to encounter the ceiling effect as a limitation.
A high benefit was identified for the home visits or home-based intervention for older adults with ADL difficulty. Home is where older adults participate in ADLs to age in place. ADL difficulty may arise when there is a mismatch between personal abilities and the home environment (Iwarsson, 2005). Conducting a home visit or a home assessment helps practitioners pinpoint the mismatch. Recommendations and interventions after the visit and evaluation are individualized, which increases their effectiveness. The intervention may include a restorative approach to increase personal abilities and assistive device provision or environment modification to lower the activity demand. This positive finding highlights the importance of addressing older adults’ living environment during evaluation and intervention if the goal is to promote independence in ADLs.
Results of the 2 studies on restorative home care services (Senior et al., 2014; Tinetti et al., 2002) somewhat contradict the positive finding of home-based intervention. Both studies used a multidisciplinary team that included an occupational therapist. Because of the limited number of studies included in this review, no conclusion can be drawn on the effect of restorative home care services on ADL outcomes. With the same inquiry, 2 systematic reviews of home care services found limited evidence for reducing ADL dependency among service users (Pettersson & Iwarsson, 2017; Whitehead, Worthington, Parry, Walker, & Drummond, 2015). The effect of home-based intervention seems to attenuate when adopted as a home care service model. Identifying factors related to this attenuation is critical to research evidence in practice and health policy.
This systematic review has several limitations. First, the search terms did not include specific health conditions, such as mild cognitive impairment or arthritis. Although the review criteria did not exclude studies of older adults with these conditions as long as they resided in the community, articles that focused on these specific groups might have been missed. Second, the six study participant categories were not mutually exclusive, nor were the six intervention strategies. For example, the multidisciplinary intervention might adopt a multicomponent program, and older adults who received restorative home care services were likely to be frail. Last, conducting a meta-analysis was not feasible because of the great variety of outcome measures and intervention content.
Implications for Occupational Therapy Practice, Education, and Research
The results of this systematic review have the following implications for occupational therapy practice, education, and research:
Conducting home visits or home-based intervention is strongly recommended to improve ADL performance in community-dwelling older adults who already experience ADL difficulty. Identifying the mismatch between clients’ personal abilities and living environment is central to maximizing occupational performance in ADLs for older adults.
Models that delineate the dynamic relationship among people, occupations, and environments, such as the Person–Environment–Occupation Model (Law et al., 1996), should be emphasized in the productive aging curriculum. Students and practitioners must familiarize themselves with the application of these models in evaluation and intervention.
Future intervention research in community-dwelling older adults is needed that includes ADLs as a primary outcome measure. Additionally, identifying or developing an outcome measure that is sensitive to changes in ADL performance is essential to advance intervention research in productive aging for community-dwelling older adults.
Conclusion
This systematic review identified six intervention approaches within the scope of occupational therapy to maintain or improve ADL performance in community-dwelling older adults. The review found a moderate benefit of using an exercise approach, particularly for frail older adults. The review also found a high benefit of using home visits or home-based intervention, particularly for older adults with ADL difficulty; such high-benefit interventions often include home modifications, highlighting the importance of including older adults’ living environment in the treatment plan to promote ADL independence.
Supplemental Material
Supplementary material for Occupational Therapy Interventions to Improve Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.031252.pdf for Occupational Therapy Interventions to Improve Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review by Chiung-ju Liu, Wen-Pin Chang and Megan C. Chang in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
Wen-Pin Chang and Megan C. Chang contributed equally to the work. We thank Marian Arbesman, Methodology Consultant to the AOTA EBP Project, for her assistance.
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.