
Abstract
Approximately 87% of American older adults want to stay in their current home as they age (AARP Livable Communities, 2014). This desire is known as aging in place—the ability to live in one’s own home and community safely, independently, and comfortably (Centers for Disease Control and Prevention, 2013). Aging in place is at risk when older adults experience declines in independence and safety (Freedman & Spillman, 2014). When age-related impairments and chronic health conditions put older adults at risk for these declines, they frequently seek assistance through community-based long-term services and supports (LTSS).
LTSS address needs related to activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Commission on Long-Term Care, 2013). Common examples of these supports include personal care, meal delivery, and transportation. Older adults may access LTSS through many sources, including informal networks, individual community resources, or well-integrated LTSS coordination programs. Regardless of the source, the predominant approach in LTSS is to provide external support to address care needs rather than to provide training or strategies to help older adults actively preserve independence and participation (Wysocki et al., 2012).
As the population ages and the demand for LTSS increases, the supply of LTSS resources to facilitate aging in place is insufficient. Waiting lists, limited availability of caregivers, inaccessible Medicaid programs, and unaffordable out-of-pocket fees are major problems within the LTSS system (Commission on Long-Term Care, 2013). Because of the reality of resource barriers, 60% of older adults who receive formal LTSS experience adverse consequences, such as falls, hospitalization, and mortality related to unmet needs in their care (Freedman & Spillman, 2014).
Occupational therapy may be one solution for lessening the gap between need and availability of LTSS. In research on aging in place, occupational therapy that centers on environmental modifications, education, and skills training to activate older adults to “do for themselves” has been identified as an effective, critical intervention for promoting independence, safety, and quality of life (Gitlin, Szanton, & Hodgson, 2013; Szanton, Leff, Wolff, Roberts, & Gitlin, 2016). Adding occupational therapy to the current menu of LTSS offered may not only facilitate aging in place but also allow for better distribution of limited resources.
Despite the promising role of occupational therapy, there remains limited knowledge on how to translate this evidence and implement occupational therapy practice into existing community-based LTSS (Sheffield, Smith, & Becker, 2013). Challenges include the culture of the community and system, geographic location (e.g., rural), reimbursement, and clients’ readiness to engage in training to do for themselves (American Occupational Therapy Association, 2013).
To advance understanding of how to implement occupational therapy as a strategy for aging in place through community-based LTSS, we describe the incorporation of occupational therapy into an LTSS coordination service: the University of Pittsburgh Medical Center (UPMC) Living-at-Home Program (LAHP). The primary aim of this study was to examine the feasibility of integrating occupational therapy within LAHP.
Method
Design
Three theoretical frameworks that promote functional change in health behavior with older adults served as the foundation of this program: (1) the Person–Environment–Occupation–Performance (PEOP) model (Baum & Christiansen, 2005), (2) the Transtheoretical Model of Change (TTM; Prochaska & Velicer, 1997), and (3) Goal-Setting Theory (Locke & Latham, 1990). PEOP is a framework for identifying clients’ strengths, values, challenges, and barriers that influence aging in place. TTM is a behavioral framework for understanding readiness for change through five change stages: (1) precontemplation, (2) contemplation, (3) preparation, (4) action, and (5) maintenance (Prochaska & Velicer, 1997).
Clients in precontemplation and contemplation require additional time, information, exploration, and reflection before changing, whereas clients in preparation require guidance in active behavior change (Zimmerman, Olsen, & Bosworth, 2000). Goal-Setting Theory emphasizes the importance of setting motivating goals that are clear and challenging to improve performance and to inspire commitment. Combined, these frameworks informed the occupational therapy service model’s holistic, behavioral, and motivational approach. Following the University of Pittsburgh Institutional Review Board guidelines, this study was approved as a Quality Improvement project by the UPMC Health System.
Setting
LAHP is a geriatric care coordination program offered through the UPMC Health System as a free community benefit to promote aging in place. LAHP uses a team-based approach that includes social work, nursing, and physician support. Clients are referred through the UPMC Health System. LAHP develops a client-centered care plan on the basis of self-report to provide care coordination, service referral, and in-home care for older adults who are at least 70 yr old, meet income guidelines, and live in urban neighborhoods of Pittsburgh (PA).
Participants
Recruitment occurred for 16 wk from January through April 2017 and was through referral from LAHP care providers. Occupational therapists collaborated with social workers and nurses to generate a referral list of clients who appeared to have unmet needs in their care and would likely be willing to engage in the occupational therapy program. Clients on the referral list were contacted and offered the opportunity to receive an occupational therapy evaluation.
Measures
The occupational therapy evaluation battery involved three components: (1) an occupational profile (American Occupational Therapy Association, 2014), (2) the In-Home Occupational Performance Evaluation (I–HOPE; Stark, Somerville, & Morris, 2010), and (3) the Readiness for Change screen (Prochaska & Velicer, 1997). The occupational profile produces a summary of a client’s history and experiences, patterns of daily living, interests, and needs. The I–HOPE is a valid and reliable measure of ADL–IADL performance for community-dwelling older adults that includes an ADL–IADL self-report assessment followed by a targeted ADL–IADL performance assessment.
We measured clients’ readiness to pursue strategies to reduce ADL–IADL difficulties using the Readiness for Change screen that determined each client’s current stage of behavior change (Prochaska & Velicer, 1997). The screen indicates that clients in the stage of preparation are ready for action-oriented programs (Wallbridge, Furer, & Lionberg, 2008). Goal attainment scaling (GAS) was used to measure the effect of occupational therapy services. GAS is a valid and reliable tool for setting quantifiable client-centered goals and measuring incremental improvement toward these goals (Kiresuk, Smith, & Cardillo, 1994).
Procedures
Occupational therapy evaluations and visits were conducted in the client’s home by a single occupational therapist who was a novice clinician but who had advanced training in geriatric occupational therapy. Clients received an occupational therapy evaluation and education on strategies for aging in place specific to their results. Clients who scored in the preparation stage on the Readiness for Change screen were assisted in establishing three goals with GAS and received four additional occupational therapy visits over 4 wk focused on skills training, problem solving, and encouragement to assist clients in achieving their goals. At the end of 4 wk, clients evaluated their current performance of the goals in relation to the indicators for goal attainment initially established.
Analysis
We analyzed data using IBM SPSS Statistics (Version 24; IBM Corp., Armonk, NY). To determine feasibility, we set benchmarks a priori as dichotomous outcomes (Table 1) on the basis of previous research that examined goal setting with older adults and recommendations for at-risk populations related to readiness for change (Prochaska & Velicer, 1997; Toto, Skidmore, Terhorst, Rosen, & Weiner, 2015). Frequencies were calculated to determine the extent to which these benchmarks were achieved. In addition, we analyzed each goal to determine level of attainment using the GAS scoring criteria. Percentage of total goals being met or exceeded was used to describe the effect of occupational therapy services for those ready for change.
Feasibility Benchmarks for the Occupational Therapy Program
Note. GAS = goal attainment scaling; LAHP = Living-at-Home Program.
Results
The flow of clients through the occupational therapy program is illustrated in Figure 1. During the 16-wk trial, LAHP providers referred 23 clients to occupational therapy, and 16 LAHP clients participated in an occupational therapy evaluation. No referred clients refused occupational therapy; reasons for not receiving an occupational therapy evaluation included hospitalization, difficulties with scheduling, and timing of the referral (e.g., at the end of the 16-wk trial). Clients were predominantly older women who lived alone (Table 2). The occupational profile revealed that although these clients received many environmental modifications through LAHP, they continued to have difficulty with ADL and IADL performance because of personal factors such as pain, fatigue, fear, and depression. Six of the LAHP clients who participated in an occupational therapy evaluation (37%) were interested in setting goals and receiving additional occupational therapy support to assist them in achieving their goals.
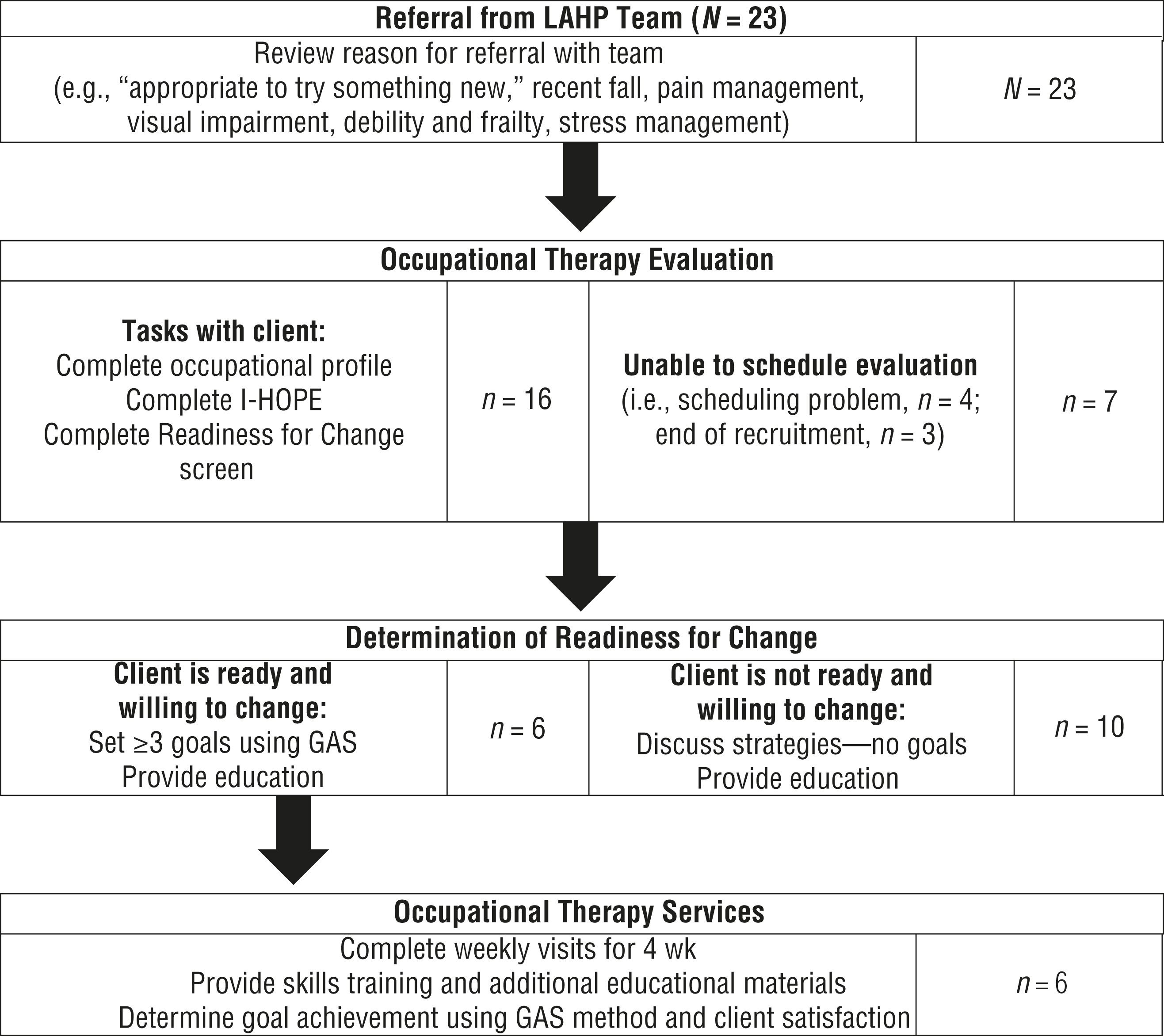
Approach to and flow of clients in the occupational therapy program.
Demographic Information of Clients Who Completed Occupational Therapy Evaluation (n = 16)
Note. ADL = activity of daily living; IADL = instrumental activity of daily living; LTSS = long-term services and supports.
Primary Aim: Feasibility
Integration of occupational therapy into LAHP was feasible, as indicated by 87% of feasibility benchmarks being met (see Table 1). Goals related to sample size were not achieved because of scheduling difficulties and a short recruitment period (see Figure 1).
Exploratory Aim: Goal Attainment
Clients who indicated a readiness for change (n = 6) established a total of 18 goals; 50% of the goals related to ADLs (n = 9), and 28% focused on IADLs (n = 5). The remaining goals (n = 4) focused on leisure and social participation. Goals were broad and reflected clients’ individual needs, ranging from establishment of pain management techniques to increasing confidence in bed mobility. Gains were reported for 100% of the goals, and all goals were met or exceeded on the basis of GAS scoring criteria.
Discussion
This project explored the feasibility of integrating occupational therapy into an existing LTSS coordination program to help older adults age in place. Although this was only a 16-wk pilot, the integration of occupational therapy into LAHP appeared to be feasible, with nearly all benchmarks being met. Clients who received support through LAHP were willing to engage in an occupational therapy program that provided strategies to better enable them to do for themselves.
The occupational therapy evaluation revealed critical information relevant to each client’s goal of aging in place. The occupational profile captured information about roles, habits, and routines that reflected clients’ occupational needs beyond basic ADLs and IADLs, thereby providing novel information for the LAHP care plan. Inclusion of performance-based assessment allowed for comparison of each client’s perceptions (i.e., self-report) and capabilities. The combination of performance-based assessment and self-report has been shown to be more accurate than self-report alone for predicting need and cost of home care services in community-dwelling older adults (Brown & Finlayson, 2013). The evaluation also confirmed the influence of pain, fatigue, fear, and depression on ADL–IADL performance. Without the inclusion of performance-based elements in the occupational therapy evaluation, the influence of personal factors may not have been revealed, given the clients’ high utilization of environmental supports through assistive devices and caregivers.
The occupational therapy program was designed on the basis of evidence suggesting that readiness for change allows for the provision of the correct support at the right time. Results of research examining an aging-in-place intervention that included occupational therapy, nursing, and a handyman reported goal attainment to be 62% more likely when a participant’s readiness for change increased by one stage (Waldersen et al., 2017). For clients not ready to do for themselves, education to promote health awareness and to stimulate interest in strategies for independence was provided. For clients who were ready, goal setting and additional occupational therapy services helped to initiate behavior change and to promote goal attainment (Wallbridge et al., 2008). Occupational therapy visits included training of compensatory and adaptive strategies and incorporated methods to increase self-efficacy.
Not everyone who was evaluated was interested in receiving additional occupational therapy support. The TTM “rule-of-thumb for at-risk populations” may explain why clients were not ready to do for themselves (Prochaska & Velicer, 1997). The rule states that in at-risk populations, only 20% are ready for change. With our sample indicating 37.5% (n = 6) readiness for change, the occupational therapy clients had a higher percentage of readiness than the TTM rule suggests. In studies investigating interventions for aging in place, older adults have demonstrated greater readiness for change when personal factors, such as depression and pain, are addressed (Waldersen et al., 2017).
Successful integration of occupational therapy into an LTSS care coordination program is dependent on several factors at both the person and the system levels. The occupational therapist who delivered our program had advanced training with frail older adults in a primary care model. Occupational therapy clinicians working in this setting must be able to demonstrate their distinct value, addressing occupations that expand beyond ADLs with consideration of performance patterns, the health care context, and the client’s personal context through a preventive approach (Siebert, 2003).
Readiness for change is not limited to the person; successful innovation in health care is often dependent on clusters of influence, including perception of innovation and contextual factors (Berwick, 2003). We had strong top-down support from the UPMC Health System. This support not only facilitated referrals from LAHP staff but allowed us to generate a part-time position in occupational therapy for the 16-wk trial. Systems that do not offer top-down support or demonstrate readiness for change may be less inclined to add occupational therapy to their menu of service options despite the potential benefits.
Our findings support the use of occupational therapy in LTSS coordination to promote aging in place. However, our study had several limitations that suggest the need for caution in interpretation of our results. We piloted a brief trial under ideal circumstances. A 16-wk window of time for recruitment and implementation resulted in a small sample. Clients referred to occupational therapy were identified as having unmet care needs and a willingness to participate. Thus, a preset bias toward readiness for change may account for our percentage of participants receiving occupational therapy visits being higher than the TTM rule. This bias may also have influenced the success that occupational therapy clients experienced in goal attainment.
Time also precluded us from revisiting clients whose screen indicated that they were not ready for change to see whether the occupational therapy evaluation and education precipitated a change in their level of readiness. In our trial, we chose to offer occupational therapy as an additional service within LAHP rather than as a billable adjunct service (e.g., outpatient therapy), thereby adding cost for the program but eliminating potential cost for the client. This decision influenced how an occupational therapist’s time was used in referral, evaluation, and intervention and may not be practical or ideal in other LTSS programs.
Future trials with larger samples, longer implementation time frames, and alternate delivery models will allow further exploration of the effect of occupational therapy service on aging in place, readiness for change, and the use of LTSS by LAHP clients.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
The deficit in the number of LTSS available for older adults who want to age in place is growing. This study demonstrates a potential role for occupational therapy in care coordination programs as an alternative to LTSS for older adults who are experiencing disability yet want to age in place.
Care coordination programs frequently rely on self-report assessment to determine an older adult’s LTSS needs. This study reinforces evidence attesting to the value of combining performance-based and self-report assessment over self-report alone to best determine an older adult’s ability and capacity for aging in place.
Environmental modifications are often considered a simple solution for reducing disability and risk for adverse events. This research reveals that addressing personal factors such as pain, fear, and fatigue is equally as important as the environment in maximizing independence to promote aging in place.
Readiness for change may be an important consideration in determining older adults who can best benefit from occupational therapy services to reduce the need for LTSS. In our research, those indicating readiness for change were able to meet 100% of goals addressing ADLs, IADLs, and leisure needs.
Conclusion
Occupational therapy offers a distinct approach for helping older adults to age in place. Making occupational therapy accessible in traditional LTSS systems may be feasible and potentially beneficial for older adults who are ready for change.
Footnotes
Acknowledgments
We thank Missy Sovak, director of the UPMC Living at Home program, and Juleen Rodakowski, assistant professor, Department of Occupational Therapy, University of Pittsburgh, for their support on this project.