
Abstract
As communication and information technologies become more sophisticated and embedded within everyday activities, people across the globe are adapting to more complex technologies (Emiliani, 2006). Increasing the use of these technologies among older adults may increase quality of life (Czaja, 2015; Gell, Rosenberg, Demiris, LaCroix, & Patel, 2015), but these technologies impose new demands on older adults, who must learn new skills to use everyday technology and engage in activities (Malinowsky, Kottorp, Patomella, Rosenberg, & Nygård, 2015). Everyday technologies—for example, stoves, phones, and health monitors—are objects that people use to engage in meaningful activities across environments and contexts (Nygård, Rosenberg, & Kottorp, 2015).
Recent studies have reported the development of assessments that systematically evaluate the use of everyday technology among older adults with and without cognitive impairments (Nygård et al., 2015; Rosenberg, Nygård, & Kottorp, 2009). In the United States, technology use and availability among older adults varies according to health and sociodemographic categories: People reporting less education and more impairments have less access to technology (Gell et al., 2015). Moreover, clients’ socioeconomic status may also create barriers or facilitators to technology access and use (Kottorp et al., 2016). Many other factors also affect the use of everyday technology to engage in activities; thus, investigating the use of everyday technology among all older adults rather than only those with cognitive impairments is critical.
The main purpose of this study was to investigate associations among activity engagement (AE), number of available and relevant everyday technologies, ability to use everyday technologies, and cognitive status among older adults in an urban area. We used the Frenchay Activities Index (FAI; Holbrook & Skilbeck, 1983) to measure AE, the Everyday Technology Use Questionnaire (ETUQ; Nygård et al., 2015) to measure the number of available and relevant everyday technologies and the ability to use those technologies, and the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) to assess cognitive status. Three main hypotheses were tested:
Higher AE will be associated with a greater number of available and relevant everyday technologies.
Higher AE will be associated with a higher ability to use everyday technologies.
Higher AE will be associated with a higher cognitive status.
Method
Participants
One hundred thirty-three participants from an urban community center for older adults indicated interest in the study, and 114 participated. The inclusion criteria were (1) age 65 yr or older and (2) able to give informed consent to participate in the study. The majority of participants reported one or more functional limitations. Four participants did not complete the FAI, reducing the number of participants to 110. In addition, 4 participants in the reduced dataset did not complete the MoCA, so analyses involving the MoCA included 106 participants. Table 1 provides an overview of participant characteristics.
Participant Characteristics by AE Group (N = 110)
Note. AE = activity engagement; ETUQ = Everyday Technology Use Questionnaire; FAI = Frenchay Activities Index; M = mean; MoCA = Montreal Cognitive Assessment; SD = standard deviation.
One participant did not report gender.
Participants reported hours of compensated work per week on the FAI.
Number of functional limitations is the number of self-reported dementia-related, neurological, developmental, mental health, medical, or orthopedic disorders.
1 = client needs maximum assistance to live in the community; 2 = client needs moderate assistance to live in the community; 3 = client needs minimal assistance to live in the community; 4 = client can live independently in the community (Nygård et al., 2015).
Four participants did not complete the MoCA.
One participant scored 30 and also reported ≤high school diploma and was thus assigned an extra point according to administration instructions (Nasreddine et al., 2005).
Instruments
Everyday Technology Use Questionnaire.
The ETUQ was developed on the basis of the interaction and match between the person’s competence and the environmental characteristics (Lawton & Nahemow, 1973; Taylor, 2017) and identifies changes in the number of available and relevant everyday technologies and in the ability to use them. The ETUQ version used includes 88 items that represent commonly used technological objects and services (e.g., stoves, the Internet, vending machines) and is administered in a 30- to 45-min semistructured interview (Nygård et al., 2015).
The ETUQ has been validated for use among many client groups, including older adults with and without specific disabilities (Hällgren, Nygård, & Kottorp, 2011; Larsson Lund, Nygård, & Kottorp, 2014; Nygård & Kottorp, 2014; Nygård et al., 2015). In addition, Kaptain, Kottorp, Patomella, and Helle (2017) reported that the ETUQ has excellent interrater reliability. The ETUQ generates two measures of everyday technology use: (1) number of available and relevant everyday technologies and (2) perceived ability to use everyday technologies. Available and relevant everyday technologies are defined as those available and previously used by the person, currently used by the person, or intended to be used by the person. The interviewer rates the person’s ability to use available and relevant everyday technologies on a six-step scale of perceived ability ranging from A (the technology is not used anymore or has not come into use even if it is relevant) to F (used without difficulties; Nygård et al., 2015).
Frenchay Activities Index.
The FAI is a 15-item self-report of engagement in instrumental activities of daily living as well as in social and community activities. It was initially validated in a poststroke population (Holbrook & Skilbeck, 1983). We used the FAI, a broad measure of AE, to separate participants into AE groups. Participants rated their frequency of engagement in activities (e.g., meal preparation, shopping, gainful work) on 13 items and identified their level of effort in AE on the remaining 2 items. The majority of items were scored 0 (never/none), 1 (rarely/light), 2 (occasionally/moderate), or 3 (often/heavy) to yield a score of as many as 45 points.
Montreal Cognitive Assessment.
The MoCA is a cognitive screen with a maximum score of 30. It was validated among older adults with cognitive impairments and assesses short-term memory recall, visuospatial abilities, executive functions, attention, concentration, working memory, language, and temporospatial orientation (Nasreddine et al., 2005). Tu et al. (2013) reported that the MoCA has good interrater reliability. We used the MoCA to measure participants’ cognitive status.
Data Collection
The University of Illinois at Chicago’s institutional review board approved the study. From November 2016 to May 2017, five interviewers—three occupational therapy students and two occupational therapy faculty members—collected data from participants. Interviewers participated in modules to learn how to administer the ETUQ from the instrument’s developers. The occupational therapy faculty members trained student interviewers in FAI and MoCA administration.
Interviewers recruited participants through referrals, face-to-face recruitment, and paper advertisements. Data collection occurred at an urban community center for older adults. Participants provided verbal and written informed consent to the interviewers and could withdraw consent before, during, or after data collection. All data were deidentified, and each participant was compensated $40.
Data Analysis
Preparatory Data Analysis.
First, we transformed the ETUQ data into interval measures by applying a Rasch rating scale model (Hällgren et al., 2011; Larsson Lund et al., 2014). Because the ETUQ has not been validated in the United States in a sample of older adults with and without specific diagnoses, a preliminary validity control was performed. Winsteps® (Version 3.93.0; Linacre, 2017) was used with an infit mean square statistic of <1.4 associated with a standardized z value of <2.0 to indicate acceptable person goodness-of-fit to the Rasch model (Patomella, Tham, & Kottorp, 2006). Only 1 participant in the sample demonstrated unacceptable goodness of fit to the model, so we used all participants’ Rasch-generated interval measures as valid estimations of ability to use everyday technologies. We reported number of available and relevant everyday technologies from the ETUQ as sums and cognitive status from the MoCA as total scores.
Primary Data Analysis.
To explore the influence of independent variables on AE, we applied a multivariate linear regression model. Independent variables included number of available and relevant everyday technologies, ability to use everyday technologies, gender, age, number of functional limitations, and cognitive status. We applied a tolerance statistic to control for multicollinearity among independent variables. A cutoff value ≤.20 indicated collinearity among the independent variables.
Participants were divided into three AE groups according to composite FAI scores to support the outcomes’ clinical relevance. The low AE group scored between 15 and 25, the medium AE group scored between 26 and 30, and the high AE group scored between 31 and 40. To compare the main independent variables of interest (i.e., number of available and relevant everyday technologies, ability to use everyday technologies, cognitive status) among the three AE groups, we performed a one-way analysis of variance (ANOVA) on each group using IBM SPSS Statistics (Version 24; IBM Corp., Armonk, NY). Post hoc Bonferroni tests were applied to further analyze differences among the three AE groups.
Results
Distributions for the FAI, ETUQ, and MoCA are provided in Table 1. The multiple linear regression model revealed that only the variables number of available and relevant everyday technologies (p < .001), age (p < .01), and number of functional limitations (p < .05) significantly predicted AE. The multiple linear regression model explained 34% of the total variance in AE. Tolerance statistics ranged from .68 to .99. Number of available and relevant everyday technologies had the lowest tolerance statistic (.68). None of the tolerance statistics indicated multicollinearity among the independent variables when predicting AE. See Table 2 for a summary.
Summary of Multiple Linear Regression Model for Variables Predicting AE Total Scores (N = 105)
Note. We excluded 5 participants with unreported gender or MoCA scores. F(6, 98) = 8.29, p < .0001. β = standardized beta coefficient; R 2 = .34. AE = activity engagement; ETUQ = Everyday Technology Use Questionnaire; FAI = Frenchay Activities Index; MoCA = Montreal Cognitive Assessment.
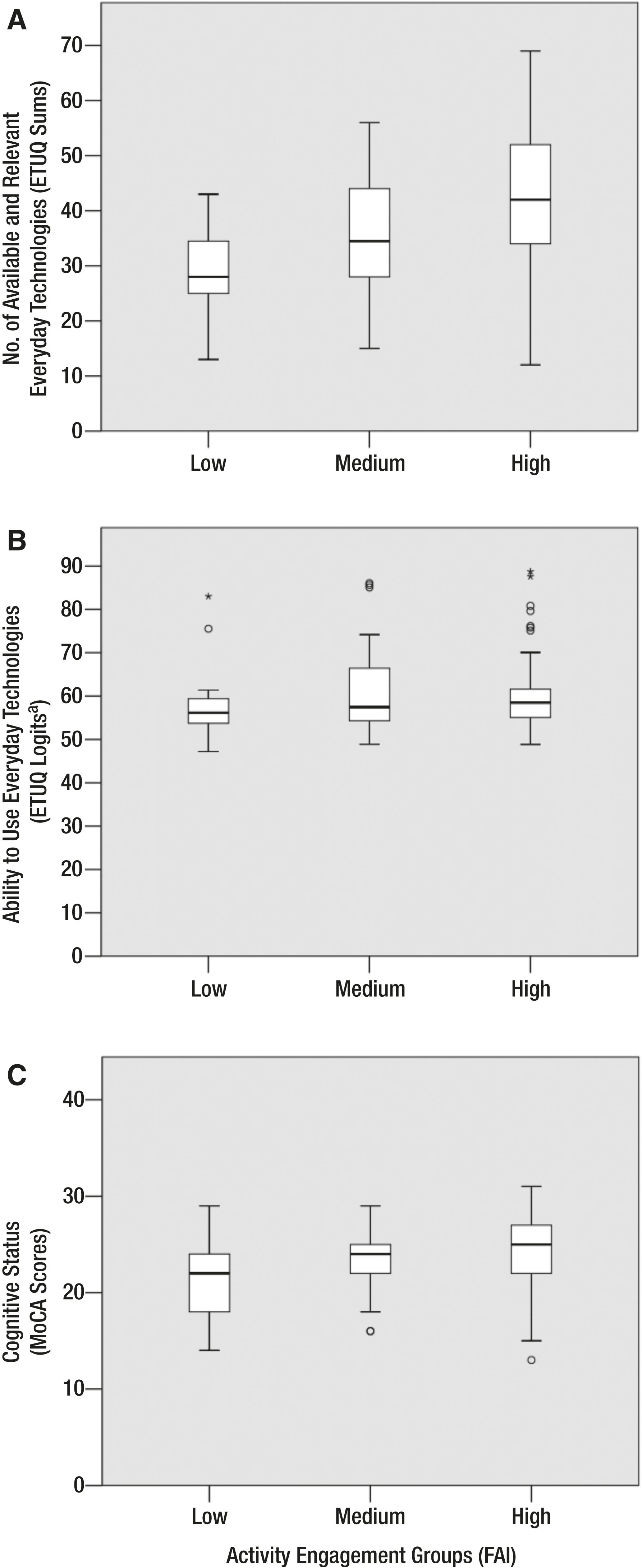
The one-way ANOVA demonstrated that participants who belonged to the medium and high AE groups also reported a greater number of available and relevant everyday technologies (p < .001). Post hoc Bonferroni tests revealed significant differences between the low AE and high AE groups (p < .001) and the medium AE and high AE groups (p < .05). The one-way ANOVA also demonstrated significant differences in cognitive status among the AE groups (p < .05). However, post hoc Bonferroni tests demonstrated significant differences in cognitive status between only the low AE and high AE groups (p < .01). We found no significant differences between the AE groups in the ability to use everyday technologies. See Table 3 for a summary of the one-way ANOVA and Figure 1 for box-and-whisker plots of AE group scores.
One-Way Analysis of Variance of Number of Available and Relevant Everyday Technologies, Ability to Use Everyday Technologies, and Cognitive Status by AE Group
Note. AE = activity engagement; df = degrees of freedom; ETUQ = Everyday Technology Use Questionnaire; MoCA = Montreal Cognitive Assessment.
Four participants did not complete the MoCA.
Discussion
The findings of this exploratory study are threefold. First, consistent with the initial hypothesis, older adults in an urban area who reported higher levels of AE also reported a greater number of available and relevant everyday technologies. Second, in contrast to the second hypothesis that groups with higher levels of AE would report greater ability to use everyday technologies, the findings indicated no significant differences among the three groups. Third, although groups that reported higher levels of AE also demonstrated higher cognitive status, post hoc testing revealed that differences were only significant between the low AE and high AE groups. Cognitive status was also not significant in the multiple linear regression model.
Hedman, Nygård, and Kottorp (2017) highlighted the importance of maintaining availability of relevant everyday technologies to sustain engagement in valued activities in a longitudinal study of older adults with mild cognitive impairment. In addition, self-efficacy in the use of everyday technology among older adults may predict the likelihood of using, learning, struggling with, or abandoning the use of challenging everyday technologies (Yagil, Cohen, & Beer, 2016). Although studies of everyday technology use among older adults have focused on specific diagnostic groups, socioeconomic or sociodemographic aspects such as income, available social support, and health status may also influence approaches to facilitating everyday technology use and AE (Gell et al., 2015; Kottorp et al., 2016). Although this study provides added insight into everyday technology use among older adults, studying even more heterogeneous samples may elevate the generalizability of findings and inform approaches to increasing self-efficacy in everyday technology use among diverse older adults.
Ability to use everyday technologies was not strongly associated with AE; we found neither significant differences among AE groups nor identifiable levels of significance in the multiple linear regression models. The findings suggest that older adults who have more available and relevant everyday technologies demonstrate higher levels of AE, despite varying ability to use everyday technologies. To further analyze both perceived and observed ability to use everyday technology among clients who may overestimate or underestimate their ability to use everyday technologies, measures such as the ETUQ should be paired with observation-based measures of everyday technology use such as the Management of Everyday Technology Assessment (Malinowsky, Nygård, & Kottorp, 2011).
In addition, the multiple linear regression model indicated that cognitive screening may not detect limitations in AE when considering the number of everyday technologies used. Moreover, the analyzed variables predicted only 34% of the sample’s variation in AE. This study’s findings suggest that screening for use of everyday technology may better predict AE than cognitive screening. However, including socioeconomic aspects of a client profile may enhance predictions (Kottorp et al., 2016).
Limitations and Future Research
This study used self-report measures, except for the MoCA, so future studies should also include measures of observed performance in everyday technology use. Future research should also compare measurements on the ETUQ and FAI with additional measurements of AE, participation, and quality of life to understand the impact of everyday technology use. Although the FAI broadly measures AE, it does not include activities specific to everyday technology use (Appelros, 2007). Thus, to address more updated profiles of AE, future studies should include measures that specifically assess activities on the FAI requiring everyday technology use. Last, the varying group sample sizes may have an impact on data analyses, and the sample may not have been sufficiently diverse to generalize findings to other populations.
Implications for Occupational Therapy Practice
As everyday technology use becomes a prerequisite for AE, practitioners can facilitate clients’ abilities to meet the demands of everyday technology use in valued activities. Practitioners are skilled in analyzing activity demands and facilitating engagement in activities requiring the use of objects such as everyday technologies (American Occupational Therapy Association, 2014). Because clients, regardless of functional status or diagnosis, engage in everyday technology use, practitioners play a role in addressing barriers to and enablers of participation in valued activities requiring use of everyday technologies (Nygård & Rosenberg, 2016). The findings of this study have the following implications for occupational therapy practice:
Using rigorously validated client-centered everyday technology use assessments such as the ETUQ may complement approaches to facilitating participation and engagement in valued activities.
Increasing the availability and relevance of everyday technologies to clients may increase frequency of engagement in activities and occupations.
Evidence of the ETUQ’s validity when used with older adults in an urban area supports its use among occupational therapists as an additional systematic approach to evaluating use of everyday technologies.
Conclusion
In summary, this cross-sectional study of older adults in an urban area suggests that differences only in number of available and relevant everyday technologies, not in the ability to use everyday technologies, exist among AE groups, despite diagnostic labels. This finding among groups of older adults divided into AE groups differs from previous studies’ findings that suggest clients’ ability to use everyday technologies varies according to diagnostic groups (Hällgren et al., 2011; Larsson Lund et al., 2014; Nygård & Kottorp, 2014). Because the relationship between everyday technology use and AE is complex, a single measurement approach may be insufficient for a heterogeneous sample of older adults.
Footnotes
Acknowledgments
We thank all participants and community partners who took part in this study. In addition, we thank the University of Illinois at Chicago’s Department of Occupational Therapy for its continuing support of this project. Last, we thank Neal Singleton for assistance with formatting the article’s figure.