
Abstract
Community-dwelling older adults are one of the fastest growing age groups in the United States (He, Goodkind, & Kowal, 2016; Ortman, Velkoff, & Hogan, 2014). Occupational therapy practitioners across various settings are tasked with the responsibility of delivering evidence-based interventions to address the occupational performance needs of older clients as they age in place or prepare for discharge back into the community (American Occupational Therapy Association, 2014). As acknowledged by various scholars in the field, multiple interventions have been designed to enhance occupational engagement for older adults (Arbesman & Mosley, 2012; Orellano, Colón, & Arbesman, 2012; Stark, Keglovits, Arbesman, & Lieberman, 2017).
Although these interventions are promising, the actual implementation of evidence-based interventions into practice can present an array of challenges. Factors such as occupational therapy practitioners’ lack of time to read current evidence-based practice (EBP) updates, difficulties with interpreting research findings, and lack of access to research articles all contribute to the widespread research-to-practice gap (Clark, Park, & Burke, 2013; Samuelsson & Wressle, 2015; Upton, Stephens, Williams, & Scurlock-Evans, 2014).
The research-to-practice gap has been well documented in the health literature across age groups (Brekke, Ell, & Palinkas, 2007; Morris, Wooding, & Grant, 2011; Scott et al., 2012), but few occupational therapy researchers have attempted to empirically examine what strategies can be integrated to expedite the adoption of evidence-based interventions into practice (Marr, 2017). In attempts to narrow the research-to-practice gap, several multidisciplinary scholars have recognized how the emerging field of implementation science can inform research translation into the field (Clark et al., 2013; Eccles & Mittman, 2006; Marr, 2017). Although select occupational therapy researchers have proposed models and frameworks to guide best practice implementation (Cahill, Egan, Wallingford, Huber-Lee, & Dess-McGuire, 2015; Colquhoun, Letts, Law, MacDermid,& Missiuna, 2010; Lin, Murphy, & Robinson, 2010), occupational therapy research continues to lack studies designed to examine implementation research outcomes and the strategies used to adopt evidence-based interventions into practice (Marr, 2017).
Historically, social work, nursing, medical, and public health researchers have been at the forefront of implementation science (Clark et al., 2013). Implementation scientists have developed models and have conducted qualitative, quantitative, and mixed-methods studies designed to examine specific interventions and strategies for increasing the implementation of evidence-based interventions (Brewster et al., 2015; Herschell et al., 2015; Jones et al., 2015; Proctor et al., 2007). Target populations of implementation studies may include practitioners, payers, managers, organizations, stakeholders, and even policymakers. The intervention itself is not necessarily the focus of implementation research. Instead, implementation science addresses the processes of how to effectively promote the uptake of evidence-based practices across all levels of health care (Bauer, Damschroder, Hagedorn, Smith, & Kilbourne, 2015).
Although implementation science is an emerging field with little presence in occupational therapy research (Clark et al., 2013), its relevance to occupational therapy for community-dwelling older adults is evident. To narrow the research-to-practice gap, purposeful research is needed to identify and measure factors related to the actual implementation of interventions in occupational therapy practice. Because of the rapid growth of the older adult population, occupational therapy researchers and practitioners face an urgent need to implement effective interventions to meet the needs of older clients. A delay in integrating evidence-based interventions into practice can ultimately have a negative impact on older adult outcomes. Because of the pressing need to implement interventions into practice with older clients, we chose to assess the breadth of implementation research related to evidence-based occupational therapy practices targeting community-dwelling older adults.
Our scoping review was guided by the methodological framework presented by Arksey and O’Malley (2005) and further discussed by Levac, Colquhoun, and O’Brien (2010). The goals underlying our decision to select a scoping review methodology were twofold: (1) to synthesize and disseminate research findings related to the implementation of occupational therapy interventions for older adults and (2) to identify gaps in occupational therapy literature pertaining to implementation research.
Method
Because of the rigorous and iterative nature of scoping reviews (Levac et al., 2010), we established an initial study protocol and revised the search process as needed on the basis of authors’ discussions and feedback from an implementation science scholar. We structured our protocol according to the five framework stages suggested by Arksey and O’Malley (2005): (1) identifying the research question, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, and (5) summarizing and reporting the results. In addition, because guidelines for scoping reviews have yet to be established, the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses; Moher, Liberati, Tetzlaff, & Altman, 2009) guidelines informed our review process.
Stage 1: Identifying the Research Question
Our goal was to identify a wide breadth of literature, regardless of study design, pertinent to the implementation of evidence-based interventions for community-dwelling older adults. Thus, we aimed to answer three broad research questions:
What factors influence effective implementation of evidence-based interventions specifically designed for older occupational therapy clients?
What types of implementation strategies (e.g., practitioner trainings, workshops, manuals) have been used to enhance the implementation of interventions with the older adult population?
What implementation outcomes (e.g., fidelity, feasibility, sustainability) have been assessed in the occupational therapy literature related to adopting evidence-based interventions with older clients?
To assist us in answering the third research question, we referred to Proctor et al.’s (2011) taxonomy of implementation outcomes. Our decision to use Proctor et al.’s taxonomy was influenced by our collaboration with an established implementation science scholar. The implementation outcomes listed in the taxonomy included acceptability, adoption, appropriateness, costs, feasibility, fidelity, penetration, and sustainability (Table 1).
Summary of the Search Strategy to Identify Relevant Articles
Note. When hand-searching journals, we entered “key implementation terms” with “key older adult terms” using the AND search function.
Stage 2: Identifying Relevant Studies
Because of the widespread use, yet conflicting definitions, of the term implementation in the allied health field, our search process first involved electronic hand searching of journals with a specific occupational therapy audience. Five electronic databases (PubMed, CINAHL, MEDLINE, PsycINFO, and SocINDEX with Full Text) were then searched to locate occupational therapy research with an implementation science focus. A full list of journals, databases, and terminology used in our search strategy can be found in Table 1.
Stage 3: Selecting the Studies
Both authors agreed on a set of search parameters before selecting relevant studies. Inclusion parameters included the following types of studies:
Published between 2002 and 2017
Contained a sample population of community-dwelling older adults ages 55 yr and older.
We also included the following studies pertaining to older adults residing in or preparing to be discharged to the community:
Written in English
Conducted in developed countries
Used qualitative, quantitative, or mixed-methods approaches.
Exclusion criteria parameters included the following types of studies:
Highlighted disciplines other than occupational therapy (e.g., physical therapy, nursing)
Measured older client outcomes only (e.g., did not measure actual implementation)
Presented as a systematic review, scoping review, literature review, narrative review, or opinion paper
Not yet conducted (i.e., published study protocols)
Used an unspecified age group.
To increase consistent application of inclusion and exclusion criteria between reviewers, both reviewers completed a sample exercise of assessing 50 titles and abstracts of occupational therapy research related to implementation science. Reviewers met and discussed the results of their sample exercise and reached consensus on article inclusion and exclusion before proceeding to reviewing the titles and abstracts identified in Stage 2.
During study selection, the titles and abstracts that were clearly eligible for full-text review were flagged by each reviewer. Articles with an unclear fit with the given criteria were marked for later discussion between reviewers to achieve consensus. Of our original 1,036 references, 46 were selected for full-text review. After reading each article in full, 13 articles were included in the present review (Figure 1).
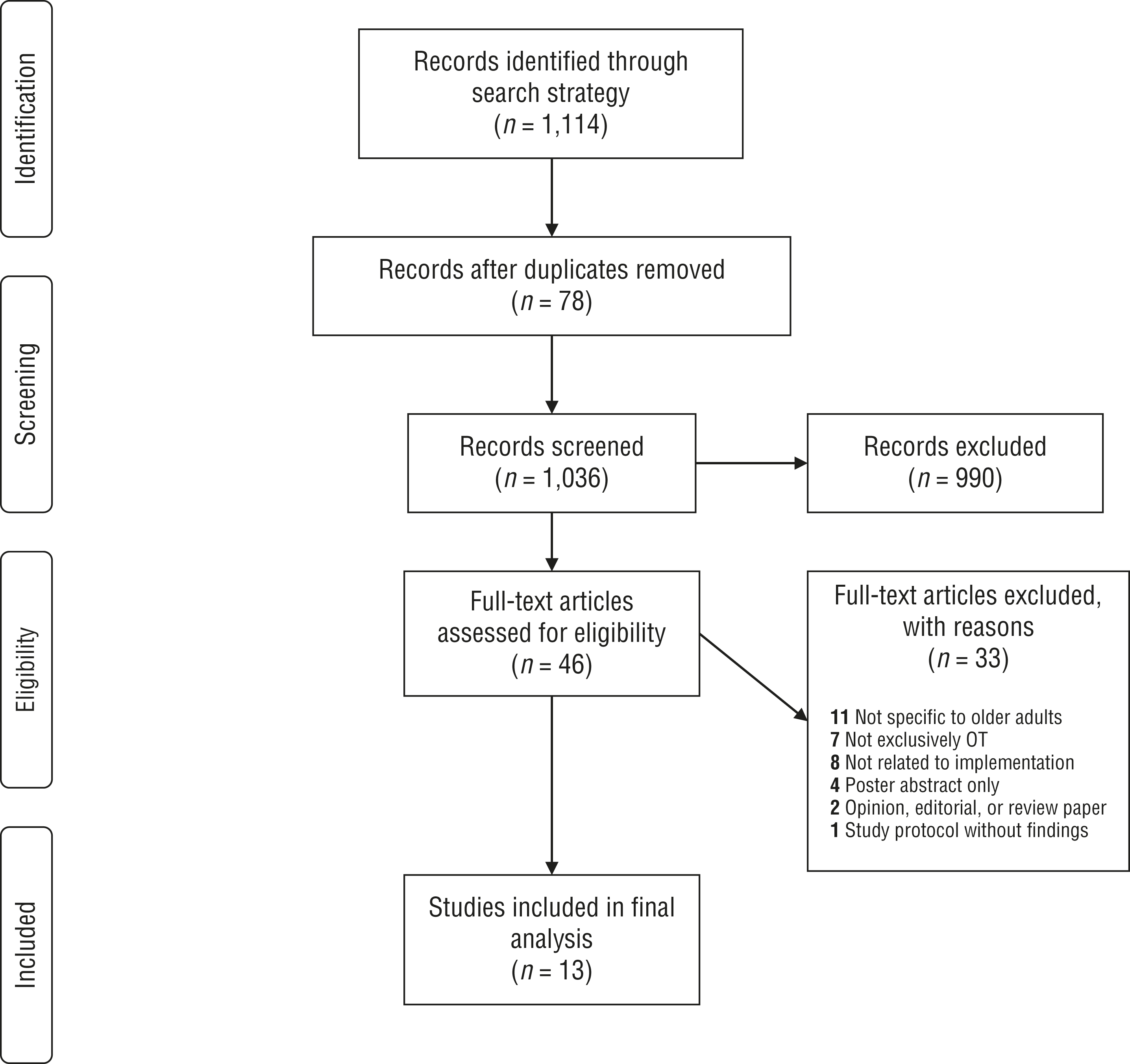
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study selection process.
Stage 4: Charting the Data
A descriptive-analytic method was used to extract information from each article. This method was adopted to provide readers with a broader understanding of each article, the processes of how implementation strategies were being used and measured (as applicable), the barriers and facilitators of implementing evidence-based interventions, and the actual intervention (e.g., a fall prevention program) being integrated into practice.
Stage 5: Summarizing and Reporting the Results
We established two processes when synthesizing the results from our review: (1) a descriptive numerical summary and (2) a thematic analysis (Arksey & O’Malley, 2005; Levac et al., 2010). In our descriptive numerical summary, we presented details about the number and type of studies included, where the studies were conducted, and characteristics about implementation barriers and facilitators as well as strategies and outcomes. We completed our thematic analysis using a content analysis approach to identify themes based on implementation barriers and facilitators as well as outcomes. We adopted these two processes to create a useful product for other researchers, clinicians, administrators, and policymakers who are interested in advancing the implementation of evidence-based interventions for community-dwelling older adult clients.
Results
Our review process yielded 13 articles included in the present review. Study types were as follows: exploratory (n = 6), descriptive (n = 4), quasi-experimental (n = 1), experimental (n = 1), and longitudinal (n = 1). Our search strategy, which was designed to locate articles specific to occupational therapy intervention implementation for older adults, yielded 8 articles addressing practitioners’ implementation of interventions, 3 articles addressing caregivers’ implementation of occupational therapy–based skills and activities with family members, 1 article examining both practitioners and caregivers, and 1 article addressing the perceptions of program recipients. Six studies deliberately measured one or more of the eight implementation outcomes identified by Proctor et al. (2011), whereas the remaining 7 studies examined barriers or facilitators to the implementation of evidence-based interventions for older adults. Thus, we chose to summarize the themes of our review into three categories: implementation barriers, implementation facilitators, and implementation outcomes. Interestingly, only 3 articles referenced purposeful use of a behavior change model to influence practitioners’ or caregivers’ implementation of new programs or interventions, and articles (n = 9) from the international literature dominated our search results.
Implementation Barriers
Key barriers, or obstacles, hindered the uptake of occupational therapy interventions for the community-dwelling older adult population. For practitioners, time restraints, organizational aspects, and costs all influenced implementation. Not having adequate time to attend trainings, learn how to use documentation tools, and actually implement complex interventions with older adult clients appeared to be major barriers to implementation (Clemson, Donaldson, Hill, & Day, 2014; Van’t Leven et al., 2012). Practitioners concerned about time restraints also expressed criticism of the costs of interventions compared with the effectiveness of the intervention itself (Clemson et al., 2014; Goodacre, McCreadie, Flanagan, & Lansley, 2008). For some practitioners, a lack of referrals from physicians and government agencies’ delayed acknowledgment of recommendations also posed barriers that affected intervention implementation (Bleijlevens, Hendriks, Van Haastregt, Crebolder, & Van Eijk, 2010; Döpp, Graff, Rikkert, Nijhuis-van der Sanden, & Vernooij-Dassen, 2013).
As with practitioners, caregivers’ perceived barriers to implementation were related to time. The usability of resources and hesitancy to change also posed notable challenges (Chee, Gitlin, Dennis, & Hauck, 2007; Hynes et al., 2016). Some caregivers also felt that programs were not quite applicable to their needs or the needs of their care recipients (Hynes et al., 2016).
Implementation Facilitators
Among practitioners, program training aspects, the usability of an intervention, and support from staff were factors that appeared to increase the uptake of occupational therapy interventions. Outreach visits, regional meetings, manualized protocols, follow-up visits, and interactive workshops were integrated into practitioner trainings to promote a positive outlook on implementation and to ensure that the new interventions were being implemented correctly (Cox, Mills, Fleming, & Nalder, 2014; Döpp et al., 2013). Support from peers and managers also facilitated practitioners’ implementation behaviors (Döpp et al., 2013).
Factors facilitating the implementation of interventions from caregivers’ perspectives included training aspects, and caregivers seemed more likely to adopt interventions if researchers or practitioners collaborated with the caregivers and clients during program or intervention development (Hynes et al., 2016). Training aspects for caregivers included interactive workshops, in-home trainings, phone calls, and manualized training modules (DiZazzo-Miller, Samuel, Barnas, & Welker, 2014; Hampson & Smith, 2015).
Implementation Outcomes
We assessed implementation outcomes on the basis of the definitions provided by Proctor et al.’s (2011) taxonomy. Main implementation outcomes included fidelity, feasibility, acceptability, sustainability, cost, appropriateness, and adoption. Because of the variability in how these outcomes were measured, we present a summary of the methods used to measure each implementation outcome. Additional details can be found in Supplemental Table 1 (available online at https://otjournal.net; navigate to this article, and click on “Supplemental”).
Fidelity was one of the most commonly measured outcomes in the 13 studies included in our review. Measurement of fidelity occurred through documentation review, vignettes, and questionnaires (Chee et al., 2007; DiZazzo-Miller et al., 2014; Döpp et al., 2015; Gitlin, Jacobs, & Earland, 2010). Feasibility was a term often encountered in our initial full-text review; however, it was seldom measured as an outcome of its own. Cassidy, Richards, and Eakman (2017) assessed program feasibility by examining recruitment rate, program attendance and completion rate, resource needs, participant satisfaction, and the intervention process, similar to how other authors have measured feasibility (Tickle-Degnen, 2013).
Acceptability has previously been termed complexity or satisfaction at the level of the practitioner or the client (Proctor et al., 2011; Rogers, 1995). Questionnaire-based data and participant satisfaction surveys were gathered to determine intervention acceptability (Cassidy et al., 2017; Chee et al., 2007; Hampson & Smith, 2015). Sustainability and costs of occupational therapy interventions for older adults were associated with funding and reimbursement. Training for caregivers was found to be reimbursable through Medicare Part B, indicating the potential for practitioners to maintain their ability to implement a reimbursable environmental skills-building program (ESP) with dementia caregivers (Gitlin et al., 2010).
Appropriateness of three different older adult interventions was measured solely through qualitative methods. Interviews and focus groups were used to assess caregivers’ and practitioners’ perspectives on interventions (Clemson et al., 2014; DiZazzo-Miller et al., 2014; Hynes et al., 2016). Adoption was an outcome of interest for one group of authors (Gitlin et al., 2010) who opted to measure practitioners’ intervention adoption through survey distribution.
Discussion
In our scoping review, we identified key barriers and facilitators to the implementation of occupational therapy interventions with community-dwelling older adults. Our search results yielded few strategies that informed how best to implement interventions with practitioners and caregivers who frequently interact with the older adult population.
Major barriers limiting practitioners’ implementation of occupational therapy interventions included time restraints, costs, and organizational hindrances. Perceived barriers to implementing interventions on behalf of caregivers also included time restraints and the complexity of new interventions. Because both practitioners and caregivers identified time restraints as key obstacles to implementation, issues such as the length of program training, the frequency of intervention delivery, and the time needed to learn documentation procedures should be considered during intervention development.
Factors that practitioners perceived to support implementation consisted of training methods, administrative support, peer support, and the intervention’s ease of use. Caregivers reported that multifaceted training methods supported implementation, which is consistent with findings in the implementation science literature (Kirchner, Waltz, Powell, Smith, & Proctor, 2018). Caregivers also identified the value of researchers and practitioners collaborating with clients and family when developing new interventions for older adults.
The identified barriers and facilitators are consistent with factors influencing the implementation of interventions with other populations in occupational therapy practice. In previous studies, researchers have found that elements limiting practitioners’ ability to implement new interventions into practice have included a lack of time, complexity of interventions, difficulty incorporating new practices into preestablished workplace routines, and difficulty locating intervention resources independently (Murphy & Robinson, 2009; Samuelsson & Wressle, 2015; Upton et al., 2014). Conversely, practitioners’ positive outlook on evidence-based research can support the implementation of interventions into practice with older adults (Eriksson, Erikson, Tham, & Guidetti, 2017).
Although our search strategy did yield 13 results that met our inclusion criteria, it is worth noting that only 6 articles explicitly addressed the methodology used to measure outcomes specific to the implementation of older adult interventions. The remaining 7 studies highlighted barriers and facilitators to evidence-based intervention implementation and would be considered “preimplementation” studies. To determine the most successful strategies for implementing occupational therapy interventions for older adults into practice, investigators are encouraged to conduct further implementation research that is purposely designed to examine an implementation strategy, such as a practitioner workshop or caregiver training, and measure implementation outcomes. Implementation research is by definition conducted to examine how to promote the effective adoption of interventions into practice (Bauer et al., 2015; Eccles & Mittman, 2006).
In our review, researchers who purposely sought to measure implementation outcomes (fidelity, feasibility, acceptability, sustainability, costs, appropriateness, and adoption) used a range of techniques to gather outcome data. Such strategies included evaluating practitioner and caregiver documentation, assessing program attendance and completion rates, using vignettes, conducting focus groups, and distributing standardized evaluation forms to practitioners and caregivers.
Despite following recommendations by Arksey and O’Malley (2005), we do acknowledge limitations in our search strategy. Because we chose to use Proctor et al.’s (2011) outcomes framework to guide our search, our results may have omitted articles that refrained from using terminology discussed in Proctor et al.’s outcomes taxonomy. Moreover, we may also have excluded articles, particularly on the basis of implementation of stroke-related interventions, that actually applied to people ages 55 yr and older. We decided to exclude implementation research articles from the stroke population because of the applicability to a wider range of ages; however, we recognize that performing a future scoping review regarding the implementation of stroke interventions into practice may be a valuable contribution to the community-dwelling older adult stroke survivor literature.
We also acknowledge that the variability among countries’ health care structures affected our ability to generalize barriers and facilitators related to costs and sustainability. We found that the majority of articles identified in our review were published in international journals, limiting the application of results to the health care reimbursement system in the United States.
Implications for Occupational Therapy Practice
The findings from our scoping review can help inform the translation of evidence-based interventions for community-dwelling older adults into practice at various stages of implementation and have the following implications for occupational therapy practice:
Occupational therapy managers and organizational leaders may consider surveying their staff to determine what perceived barriers and facilitators influence practitioners’ adoption of occupational therapy interventions for community-dwelling older adults.
Clinic or organizational team leaders seeking to integrate research into practice may consider using strategies such as workshops, follow-up consultations from experts, fidelity vignettes, peer mentoring, and standardized training modules to enhance the implementation process related to older adult interventions.
Practitioners who train caregivers in how to implement interventions with family members should collaborate with caregivers and families to ensure that the intervention can be integrated into daily routines with greater ease and acceptability. Caregivers may be more accepting of programs and care strategies after participating in interactive demonstrations with practitioners delivering the training.
Conclusion
On the basis of the results of our scoping review, we propose that an implementation research agenda specifically targeting interventions designed for community-dwelling older adults is needed. We challenge researchers, particularly those who have developed evidence-based interventions for older adults, to conduct studies designed to purposely examine how to effectively implement their interventions into practice. A first step may include descriptive studies that determine the key barriers to or facilitators of evidence-based intervention adoption by practitioners and organizations, followed by empirical studies (based on behavioral change theories) that assess the most effective strategies (i.e., live trainings, webinars, or e-modules) for promoting the uptake of interventions designed for older adults. Researchers are directed to Bauer et al.’s (2015) article in which the authors presented a clear definition of implementation research as it applies to health care.
Although we value interventions—such as COTiD (Community Occupational Therapy in Dementia; Hynes et al., 2016), ESP (Gitlin et al., 2010), and Aging Well by Design (Clark et al., 1997, 2012)—that have already been well-supported in the literature and viewed as effective interventions targeting older adults, we argue that the need for implementation research is equally as important as the development of these interventions themselves. Because the older adult population continues to grow, occupational therapy practitioners are faced with the immediate challenge of determining how to successfully integrate effective, evidence-based interventions and programs into practice. Occupational therapy researchers are encouraged to collaborate with implementation scientists to decrease the research-to-practice gap, thereby enhancing practitioners’ skills, which, in turn, can enhance the well-being and occupational engagement of community-dwelling older adults.
Supplemental Material
Supplementary material for Implementing Evidence-Based Interventions With Community-Dwelling Older Adults: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.031583.pdf for Implementing Evidence-Based Interventions With Community-Dwelling Older Adults: A Scoping Review by Lisa A. Juckett and Monica L. Robinson in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We extend our appreciation to our colleagues, Elizabeth Koss and Christopher Brown, for their supportive feedback and insight throughout the iterative scoping review process. We also thank Alicia C. Bunger for providing her implementation science perspective during the development of this article.
*
Indicates studies included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.