
Abstract
In 2015, an estimated 9.8 million American adults were labeled as having a serious mental illness (SMI), and approximately 65% of these individuals received mental health services within the year (Center for Behavioral Health Statistics and Quality, 2016). According to the Substance Abuse and Mental Health Services Administration (2017), the SMI population includes all people
having, at any time during the past year, a diagnosable mental, behavior, or emotional disorder that causes serious functional impairment that substantially interferes with or limits one or more major life activities. Serious mental illnesses include major depression, schizophrenia, and bipolar disorder, and other mental disorders that cause serious impairment. (para. 7)
Most adults with SMI desire to work or engage in education programs and perceive education and employment as valuable in the recovery process (Dunn et al., 2008; Fernando et al., 2017). The value of employment includes potential increases in financial stability, social interactions, self-esteem, and community integration (Koletsi et al., 2009). The majority seeking employment also report a need for more skills training and favorably view vocational services in both Clubhouse and clinical settings (McQuilken et al., 2003).
Despite the recognition of the benefits of work and the desire to engage in employment and educational programs in accordance with social roles, adults with SMI continue to struggle to gain competitive employment. The National Institutes of Health, reporting data from 2009 and 2010, showed that adults with SMI had substantially lower employment rates than the general population (Luciano & Meara, 2014). For adults aged 18–64, the full-time employment rate was 61.7% for those with no mental illness, yet only 38.1% for those with SMI. Adults with SMI also had much lower wages (38.5% earning under $10,000 per year) and an increased likelihood (40.7%) of missing or skipping a day of work weekly (Luciano & Meara, 2014).
For adults with SMI, barriers to obtaining and maintaining employment include personal factors such as psychiatric symptoms, minimal or no previous work experience, low confidence and motivation, and long periods of being out of work. External barriers include restricted job markets, complex job search procedures, nonsupportive working conditions, lack of meaningful work, and stigma associated with mental illness (Koletsi et al., 2009; Milfort et al., 2015). In the United States, concern over losing disability benefits in exchange for low pay is one of the most prevalent deterrents to seeking employment (McQuilken et al., 2003).
Research reveals common trends in the process of overcoming barriers to competitive employment. For example, evidence shows that both cognitive and social functioning should be addressed in supported employment programs (Saavedra et al., 2016). Lexén and Bejerholm (2016) demonstrated that higher quality communication and interaction skills (e.g., asking questions, sharing information, sustaining conversation in an appropriate manner) were significantly correlated with increased working hours and higher income for adults with SMI. Research has also shown that effective cognitive skills are critical to successful work performance. In fact, improvement in attention and vigilance in adults with SMI has been shown to improve vocational outcomes (Puig et al., 2016).
Barriers to education include previous negative educational experiences, sporadic attendance at school because of psychiatric symptoms, feelings of frustration and apathy, and withdrawal prior to graduation (Fernando et al., 2017). Currently, few formal supported education programs exist in the United States, and occupational therapy practitioners are seldom found in them (Gutman et al., 2009).
The objective of this systematic review was to answer the research question, What is the evidence for the effectiveness of interventions to improve and maintain participation and performance in employment and education for people with serious mental illness?
Method
The research question was reviewed by review authors, an advisory group of experts in the field, American Occupational Therapy Association (AOTA) staff, and the methodology consultant to the AOTA Evidence-Based Practice (EBP) Project. Search terms for the reviews were developed by the methodology consultant to the EBP Project and AOTA staff, the review authors, and an advisory group. Table 1 lists the search terms related to population (SMI), types of interventions, and study designs included in the systematic review.
Key Search Terms for the Systematic Review of Occupational Therapy Intervention With Employment and Education for Adults With Serious Mental Illness
A medical research librarian with experience in completing systematic review searches conducted the search and confirmed and improved the search strategies. Databases and sites searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and consolidated information sources such as the Cochrane Database of Systematic Reviews. Moreover, reference lists from articles included in the systematic review were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included. This review was limited to peer-reviewed scientific literature published in English, and the intervention approaches examined were within the scope of practice of occupational therapy for adults with SMI, as defined by the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014). The literature included in the review for this question was published between January 2008 and June 2016. The review included only Level I, II, and III evidence and excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses.
The systematic review was carried out as an academic partnership in which academic faculty worked with a student as a team. This team narrowed the initial search results by reviewing citations and abstracts provided from the search, retrieved the full-text versions of potential articles, and selected and reviewed those articles using the predetermined inclusion and exclusion criteria. Of the 952 abstracts initially reviewed, 57 articles were critically appraised according to their quality and level of evidence (Figure 1). Each article was abstracted using an evidence table that summarizes the methods and findings of the article. AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. All studies are summarized in full in the evidence table in Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”).
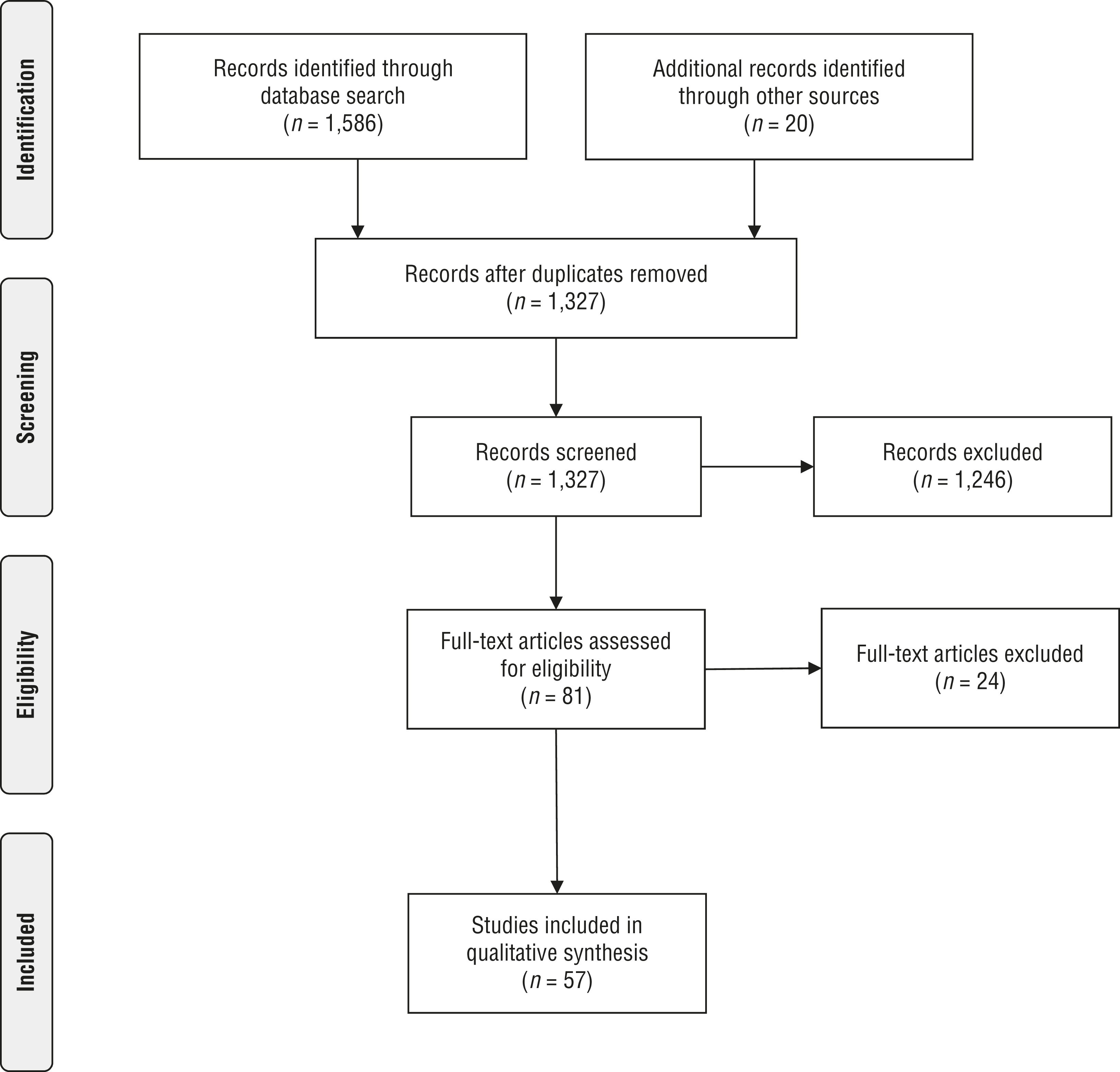
Flow diagram for studies included in the systematic review.
The risk of bias for individual studies (Higgins et al., 2011) and systematic reviews (Shea et al., 2007) included in this review was assessed using the methods appropriate for each (see Supplemental Tables 2 and 3, available online). Of the 49 individual studies, 35 used random assignment and had blinding of patient-reported outcomes, 24 included allocation concealment, 17 used blinding of participants and personnel, 36 had high or unclear risk of attrition bias, and 46 had low risk of reporting bias. Of the 8 systematic reviews or meta-analyses, 2 had good rigor, and the other 6 presented potential risk of bias in 2 to 4 of the 11 areas assessed.
The strength of the evidence was evaluated using the guidelines of the U.S. Preventive Services Task Force (2017). According to these guidelines, a designation of strong evidence indicates consistent results from well-conducted studies, usually at least two randomized controlled trials (RCTs). Moderate evidence consists of one RCT or two or more studies with lower levels of evidence. Limited evidence indicates that there are few studies, flaws in the available studies, and some inconsistency in the findings across individual studies. A designation of mixed evidence indicates that findings were inconsistent across studies in a given category, whereas insufficient evidence indicates that the number and quality of studies are too limited to make any clear classification.
Results
The strongest evidence for interventions to support employment and education for adults with SMI was found in studies using the Individual Placement and Support (IPS) model, various forms of cognitive intervention, and supported education programs.
Individual Placement and Support
The IPS model of supported employment has been rigorously researched since its inception, and strong evidence exists for its effectiveness (Mueser & Cook, 2016). This service provision model is based on eight key elements that hold competitive employment as the goal and privilege clients’ choices and preferences. Other key elements of IPS include a rapid job search, unlimited individualized support, and integration of the client’s vocational and mental health teams (Bond et al., 2012). Of the IPS studies appraised, 31 provided Level I and 5 generated Level II evidence. The majority of Level I studies compared IPS with traditional vocational rehabilitation (TVR), whereas others compared IPS with novel interventions including occupational therapy, mindfulness-based stress reduction (MBSR), and background music.
Five systematic reviews determined that IPS significantly increased competitive employment rates for adults with SMI (Arbesman & Logsdon, 2011; Bond & Campbell, 2008; Bond et al., 2008; Gibson et al., 2011) and supported participants to find jobs more quickly and keep them longer (Kinoshita et al., 2013). In two meta-analyses, Campbell et al. (2010, 2011) found that IPS resulted in better competitive employment rates for all participants except those who had more than a high school education or were separated or divorced. Another meta-analysis determined that initial benefits of IPS intervention for participants continued over a 2-yr period (Modini et al., 2016).
Eight of 11 RCTs found IPS to be superior to TVR in vocational outcomes, demonstrating double the rates of competitive employment and job tenure, more hours worked and higher total income, and improved quality of life for participants (Areberg & Bejerholm, 2013; Catty et al., 2008; Heslin et al., 2011; Kin Wong et al., 2008; Kukla & Bond, 2013; Michon et al., 2014; Twamley et al., 2008, 2012). Three RCTs showed less success for IPS; Burns et al. (2009), for instance, found that working at all—whether in IPS or TVR—resulted in improvement in symptoms and social function. Howard et al. (2010) believed that the context in which their study was conducted—a socioeconomically deprived area with a somewhat rigid welfare benefits system, with intervention provided by an external agency—negatively influenced the successful implementation of IPS. And Poremski et al. (2017) noted that although IPS intervention showed a trend toward increased rates of competitive employment, results did not reach statistical significance.
Several Level I RCTs compared IPS with other types of vocational intervention, including job clubs, the Clubhouse Model (Schonebaum & Boyd, 2012), occupational therapy–specific programs or interventions, and Integrated Supported Employment (ISE). Bond et al. (2015) compared IPS with a job club intervention and reported similar outcomes on all measures except competitive employment rates, which were 31% for IPS participants and 7% for job club participants. Four studies used supported employment methods derived from but not using the IPS model (Cook et al., 2008, 2016; Hoffmann et al., 2012, 2014) and found similarly high rates of competitive employment for participants in the supported employment programs compared with those who received variations of TVR. In a 2014 RCT, Mueser et al. compared IPS with a Psychosocial Clubhouse intervention and found that IPS demonstrated work outcomes that were statistically significant across all measures of competitive employment, including a rate of competitive employment 4 times higher (73%) than that for the Clubhouse (18%).
Hees et al. (2013) added occupational therapy to treatment as usual (TAU) and compared work participation, at-work and health-related functioning, and coping skills with TAU only. Although nearly all participants (91%) achieved at least partial return to work, no significant benefit was attributable to occupational therapy for work participation (defined in terms of absenteeism and length of time until partial or full return to work). However, results indicated that occupational therapy intervention improved the probability of long-term return to work (defined as full return to work while being remitted from symptoms of depression and with better work and role functioning), increased long-term depression recovery, and reduced need for other high-cost medical treatment during intervention.
Four studies investigated the use of ISE, which is IPS plus social skills training. H. W. H. Tsang et al. (2009, 2010) compared ISE with IPS only and with TVR only, and Waghorn et al. (2014) compared ISE with nonintegrated supported employment, with all studies showing significantly better competitive employment rates for participants in the ISE program. Au et al. (2015) added cognitive remediation training (CRT) to ISE and compared the combined intervention with ISE only. Both programs demonstrated improvement in vocational outcomes, with no evidence that CRT contributed to improvements beyond those already associated with ISE.
Two Level I studies addressed unique vocational interventions. Davis et al. (2015) studied a version of MBSR that had been modified for people with schizophrenia: MIRRORS (Mindfulness Intervention for Rehabilitation and Recovery in Schizophrenia). Participants in the MIRRORS program sustained work longer and performed better at a work placement than those in the control condition. Shih et al. (2015) studied the use of background music with adults with schizophrenia and found significant improvement in scores on an assessment of attention.
Several Level II studies supported the effectiveness of IPS. For instance, van Veggel et al. (2015) demonstrated that IPS resulted in a statistically significant improvement in obtaining competitive employment compared with conventional vocational rehabilitation (CVR). Competitive employment rates during the 12 months of the study were nearly twice as high for IPS (24.9%) as for CVR (14.3%). The Psychosocial Clubhouse Model was investigated in 2 Level II studies. Schonebaum and Boyd (2012) found that the work-ordered day that provides daily structure in Clubhouses had a significant positive impact on total employment duration before employment but a significant negative relationship to total employment duration during employment. In A. W. Tsang et al.’s (2010) study, employment rates were significantly higher for Clubhouse participants compared with control participants. Using standard vocational rehabilitation for intervention, Watzke et al. (2009) showed a statistically significant improvement in employment status and more competitive employment at 9-mo follow-up compared with TAU. Rouleau et al. (2009) tested an occupational therapy–led prevocational program (OT–PVP) based on Anthony and Liberman’s (1986) model of skills training, combined with cognitive–behavioral and skills training and psychosocial approaches. Participants in OT–PVP achieved volunteer or paid work at more than 4 times the rate (71%) of the TAU group (16%) and showed statistically but not clinically significant reduction in negative symptoms on the Positive and Negative Symptom Scales and in general symptom scores at discharge.
One retrospective cohort study (Chuang et al., 2015) found four variables that reached statistical significance in discerning employment outcomes for people who participated in a prevocational program during psychiatric inpatient admission. Participants were more likely to be employed (sheltered, supported, or competitive employment) if they had an associate or college degree; good, fair, or mildly impaired hand function; excellent, good, or average core strength; and vocational counseling services posttraining.
Cognitive Interventions
Fifteen Level I studies used cognitive remediation methods that improved outcomes for both cognitive skills and employment. Such methods included the Neuropsychological Educational Approach to Remediation (NEAR) technique (Hodge et al., 2010), neurocognitive enhancement therapy plus a vocational program (Bell et al., 2008a, 2008b), cognitive enhancement therapy (Eack et al., 2011), Thinking Skills for Work (McGurk et al., 2015), and cognitive remediation (Bio & Gattaz, 2011; Lee, 2013; McGurk et al., 2009; Tan & King, 2013; Tao et al., 2015). Positive results included broad cognitive improvement, significantly higher rates of competitive employment, increased length of employment and hours worked, significantly higher earnings per week, and higher satisfaction with employment status. Cognitive–behavioral therapy intervention also contributed to better vocational outcomes (Kukla et al., 2014; Lysaker et al., 2009).
In 2 studies using virtual reality interventions, participants received more job offers (Smith et al., 2015) and experienced improved cognition (M. M. Y. Tsang & Man, 2013). Additionally, Chan et al.’s (2015) meta-analysis found that computer-assisted cognitive remediation enhanced productivity outcomes for participants with SMI.
Two Level II studies addressed cognitive remediation interventions. Quee et al. (2014) found that cognitive adaptation training plus TAU resulted in significantly more hours spent in work-related activities than TAU. Sato et al. (2014) compared cognitive remediation plus supported employment with supported employment only and found no significant change in employment status in either condition.
A Level III study by McGurk et al. (2010) reported that participants in the Thinking Skills for Work program at a Psychosocial Clubhouse worked significantly more competitive hours per month. Significant improvements were also noted in participants’ overall cognitive composite scores.
Supported Education
Only 2 studies on supported education met the criteria for this review, and although both were Level I studies, they provide only moderate strength of evidence because of inconsistency of results within and across the studies. In a quasi-experimental study of the Bridge Program, a supported education program using occupational therapy intervention (Gutman et al., 2009), participants increased their skill level in basic academic areas, improved professional behaviors and social skills needed for school and work settings, and gained the confidence to test their skills in the larger community. Factors that correlated most with success in the program included adherence to a medication routine, stable residence, and motivation to attend the program regularly.
Kidd et al.’s (2014) RCT added cognitive remediation to supported education interventions and showed that although both treatment and control groups demonstrated improvements in cognitive functioning, there was no evidence that cognitive remediation facilitated improvement in cognition above and beyond gains associated with supported education. However, improvements in academic functioning were associated with cognitive remediation, and treatment participants showed a greater rate of completion of the first semester.
Discussion
The typical age of onset for SMI, during emerging adulthood, coincides directly with the developmental tasks of completing education and beginning to work. Further, the cognitive impairments that co-occur with SMI can cause more interruption in occupational performance than the symptoms of the illness itself (Bell et al., 2008a; Kidd et al., 2014), negatively affecting school and work performance. Yet adults with SMI desire to engage in age-appropriate life roles of student or worker, despite the barriers to education and employment presented by those illnesses (Gutman et al., 2009; McGurk et al., 2015). The results of this systematic review provide recent evidence for the effectiveness of supported employment and education interventions for adults with SMI. Three prominent program strategies emerged in the review: (1) IPS and (2) cognitive remediation as interventions for employment are supported by strong evidence, and (3) supported education programs are supported by moderate evidence.
Very few of the studies reviewed were conducted by occupational therapy researchers or addressed a role for occupational therapy practitioners in the interventions; however, this review intentionally included only interventions that fall within the scope of occupational therapy practice. Therefore, these evidence-based interventions can be used by occupational therapy practitioners working with adults with SMI who wish to engage in education or employment. For instance, occupational therapy philosophy and theory align seamlessly with the core principles of the IPS model (Bond et al., 2012), which has been studied persistently and rigorously and determined to be a successful evidence-based practice for supported employment. Numerous models of cognitive intervention also were shown to positively affect employment outcomes for adults with SMI, and cognition is clearly a factor in successful supported education experiences as well. Occupational therapy practitioners possess the expertise for intervention in the area of cognition as it relates to both employment and education for adults with SMI (AOTA, 2013).
Implications for Occupational Therapy Practice
Occupational therapy practitioners working with adults with SMI in their employment and educational pursuits can use this updated evidence to choose effective interventions. In addition, more high-level research on this topic is required from the field of occupational therapy. Further investigation of the contributions of occupational therapy in supported education and employment programs would serve both to increase the evidence base and to more clearly delineate the crucial role of occupational therapy in providing these services to adults with SMI.
Limitations
The variation in design, method, and quality of the individual studies used presents limitations in a systematic review. Many of the studies in this review were limited by risk of bias (see Supplemental Tables 2 and 3, online), and although this review includes only studies using interventions within the scope of occupational therapy practice, few of the studies were conducted by occupational therapy practitioners. In addition, only occupational therapy practitioners were involved as reviewers in this systematic review, contributing to potential bias.
Conclusion
Adults with SMI consistently express the desire to engage in student and worker roles. This review presents strong to moderate evidence for specific interventions that fall within the scope of occupational therapy practice and that promote positive education and employment outcomes for adults with SMI.
Supplemental Material
Supplementary material for Evidence for Occupational Therapy Intervention With Employment and Education for Adults With Serious Mental Illness: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.033068.pdf for Evidence for Occupational Therapy Intervention With Employment and Education for Adults With Serious Mental Illness: A Systematic Review by Susan Noyes, Helena Sokolow and Marian Arbesman in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman, Marian Arbesman, and Beth Hunter for their guidance and support and Jill Blackstock for technical assistance during the systematic review process. This systematic review was presented preliminarily at the 2017 AOTA Annual Conference & Expo in Philadelphia.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.