
Abstract
The transition from adolescence to young adulthood (12–35 yr old) is a period of increased risk for onset of serious mental illness (SMI; McGorry, 2011). Early detection and rapid intervention may reduce the impact of mental illness and may even delay or prevent transition to SMI. Early intervention may also reduce the risk of death by suicide or a lifetime of disability characterized by unemployment, incomplete education, social isolation, and significant symptoms that interfere with daily living (Gonzalez et al., 2015; McGorry, 2011).
SMI, such as schizophrenia, bipolar disorder, and major depression, costs the U.S. government substantial amounts of money for Medicaid subsidies and other benefits (Gonzalez et al., 2015). Early intervention services (EIS), especially for people experiencing the early signs or first episode of psychosis, have been shown to be effective in reducing the impact of SMI through early detection, targeted interventions, and easy access to care (Bird et al., 2010; Gonzalez et al., 2015).
We were unable to find a systematic review that specifically focused on the role of occupational therapy in EIS for people with SMI or specifically on interventions to improve occupational performance in this population. This review aimed to identify the evidence related to specific interventions within the scope of occupational therapy practice for people in the early stages of onset of SMI. This review focuses on the question, What is the evidence for the effectiveness of early intervention to improve and maintain performance in occupations for people with serious mental illness? This research question was developed collaboratively by the review authors, an advisory group of experts in the field, staff of the American Occupational Therapy Association (AOTA), and the methodology consultant to the AOTA Evidence-Based Practice (EBP) Project.
Method
We used the PRISMA methodology (Moher et al., 2009) in conducting this review. The search terms were developed not only to capture pertinent articles but also to make sure that the terms relevant to the specific thesaurus of each database were included. Table 1 lists the search terms included in this systematic review.
Key Search Terms for the Systematic Review of Early Intervention in Mental Health for Adolescents and Young Adults
A medical research librarian with experience in completing systematic review searches conducted the search and confirmed and improved the search strategies. Databases and sites searched included MEDLINE, PsycINFO, CINAHL, and OTseeker. In addition, consolidated information sources, such as the Cochrane Database of Systematic Reviews, were included in the search; these databases are peer-reviewed summaries of journal articles and provide a system for clinicians and scientists to conduct systematic reviews of selected clinical questions and topics. Moreover, reference lists from articles included in related systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
Two of the authors (Roush and Downing) conducted the remainder of the review, beginning by independently reviewing citations and abstracts of the articles identified by the medical research librarian to determine whether to obtain the full-text article for further consideration. The two authors discussed discrepancies until they reached agreement. The same process was used to evaluate the full text of potential articles. They then recorded a summary of each article in an evidence table, rated each article for risk of bias, and determined themes presented by the articles. AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) is the evidence table for the systematic review.
Inclusion criteria specific to this review were as follows: participants age 12–35 at entry; ≤2 yr of active symptoms at entry; diagnosis of psychosis, depression, or anxiety disorder; and focus on functional outcomes rather than symptoms. Personality disorder diagnoses were excluded. General inclusion criteria of the larger systematic review that included this question were as follows: peer-reviewed scientific literature published in English, intervention approaches within the scope of practice of occupational therapy for the target diagnoses, and publication between 1995 and 2016. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses.
Studies included in the review provide Level I, II, and III evidence. Ratings of the strength of the evidence are based on the guidelines of the U.S. Preventive Services Task Force (2017), defined as follows:
Strong evidence includes consistent results from well-conducted studies, usually at least 2 randomized controlled trials (RCTs).
Moderate evidence indicates 1 RCT or 2 or more studies with lower levels of evidence. Some inconsistency of findings across individual well-conducted studies could preclude a classification of strong evidence and result instead in a designation of moderate evidence.
Mixed evidence indicates that the findings were inconsistent across studies in a given category.
Insufficient evidence indicates that the number and quality of studies are too limited to make any clear classification (AOTA, 2016, p. 4).
Results
Of the 25,775 citations and articles found by the research librarian, 512 were reviewed by the authors for relevance to this study question. An additional 158 articles were identified by hand search. A total of 234 full-text articles were assessed, and 30 met the inclusion criteria (see Figure 1): 22 articles provided Level I evidence, 6 provided Level II evidence, and 2 provided Level III evidence. Critical appraisal of the evidence revealed four primary categories of intervention: cognitive remediation (CR), cognitive–behavioral therapy (CBT), supported education and supported employment (SE/E), and family psychoeducation (FPE).
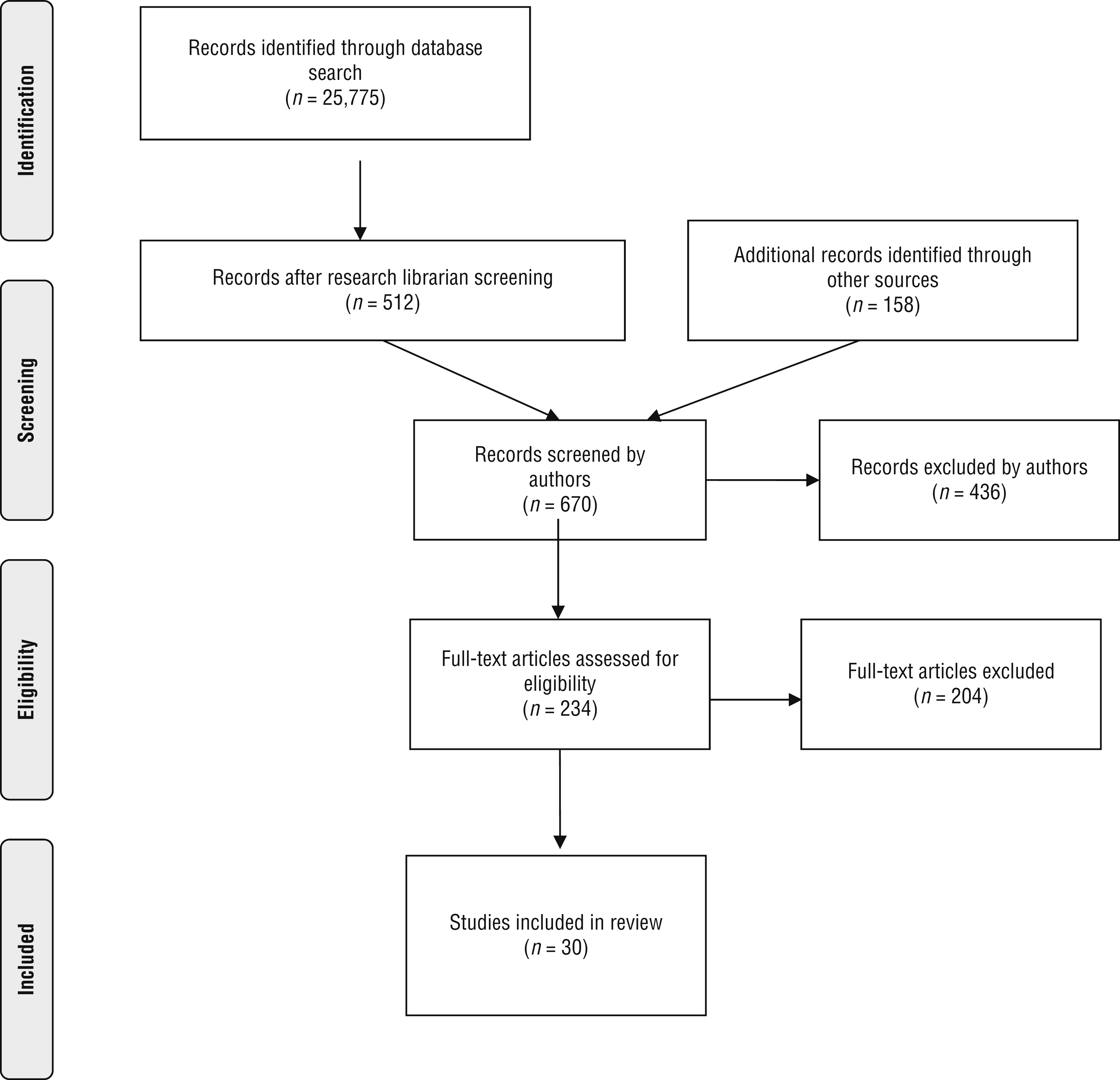
Flow diagram for studies included in the systematic review.
Risk of Bias
The risk of bias in the 28 individual studies was assessed using the methods described by Higgins and colleagues (2011). Fifteen studies were identified as using random assignment and had blinding of patient-reported outcomes, 10 studies included allocation concealment, only 1 study had blinding of participants and personnel, 14 studies had high or unclear risk of attrition bias, and 26 studies had low risk of reporting bias. The method for assessing the risk of bias in the 2 systematic reviews included was based on the measurement tool developed by Shea et al. (2007); 1 review had good rigor and the other had higher risk of potential bias in 6 of the 11 areas assessed. Supplemental Tables 2 and 3 (available online) provide the risk-of-bias assessment for all studies included in this review.
Cognitive Remediation
Six Level I RCTs and 1 Level II pre–post study provide moderate evidence for using CR in early intervention for psychosis to improve cognition, self-esteem, and social and occupational functioning. All 6 RCTs reported improvements in specific targeted cognitive areas and social and occupational functioning using computer-based cognitive training activities (Holzer et al., 2014; Lee et al., 2013; Loewy et al., 2016; Mendella et al., 2015; Østergaard Christensen et al., 2014) or paper-and-pencil activities (Puig et al., 2014). Østergaard Christensen et al. (2014) found that CR significantly improved participants’ verbal learning immediately after CR and at 12 mo and working memory at 12 mo. Improvements in verbal learning and working memory are supportive of occupational functioning.
The Level II study demonstrated improvements in participants’ cognition and overall functioning using computerized cognitive training software for those with clinical high risk for psychosis (CHR; Rauchensteiner et al., 2011). However, Puig et al. (2014) found that functional gains were not maintained at 3 mo, resulting in mixed evidence for duration of effect.
Cognitive–Behavioral Therapy
Nine Level I studies, 8 RCTs and 1 systematic review, addressed CBT’s effectiveness in treating cognitive dysfunction and symptoms to improve overall functioning. The studies focused on youth with CHR, first-episode psychosis (FEP), or depression.
Participants With CHR or FEP.
Moderate evidence for the effectiveness of CBT in improving functioning was found in 6 studies. Hutton and Taylor’s (2014) meta-analysis of 6 RCTs comparing CBT for nonmedicated youth with CHR with treatment as usual found strong evidence that CBT lowered the risk of conversion to psychosis up to 24 mo and reduced symptoms at 1-yr follow-up. Conversion to psychosis leads to decreased occupational functioning (Bird et al., 2010; Gonzalez et al., 2015). Gleeson et al. (2013) found substantially lower relapse rates and significant delay in time to relapse for a CBT intervention group compared with a control group, but these results were not sustained at 12-mo follow-up. As with conversion to psychosis, relapse leads to decreases in occupational functioning.
Jackson et al. (2008) found significantly more functional improvement in a CBT intervention group at the midway point compared with a control group, but neither group maintained improvements over time. Yung et al. (2011) studied the effects of CBT with or without medication (two intervention cohorts) with supportive therapy and control groups receiving only follow-up assessment. The CBT without medication, supportive therapy, and control groups all had significant gains in functioning, whereas the CBT plus medication group did not. Three studies (Addington et al., 2011; Bechdolf et al., 2007; Jackson et al., 2008) found no significant differences between CBT and control groups.
Depression.
Three studies evaluating CBT’s effectiveness for youth with depression demonstrated mixed results, especially for sustained improvements. Brent et al. (2015) tested a time-limited cognitive restructuring intervention with 6-mo booster sessions for youth with subsyndromal depressive symptoms. Functional outcomes were reported only at the 6-yr mark and showed no differences between groups. Clarke et al. (2001) demonstrated positive outcomes in functioning for an intervention group receiving group prevention education and treatment sessions for parents. At 2-yr follow-up, treatment effects had not been sustained. Stice and colleagues (2008) tested three different interventions against a control group and found that CBT significantly reduced depressive symptoms compared with the other two intervention groups and the control group. Depressive symptoms have a negative impact on occupational functioning.
Supported Employment and Supported Education
Moderate evidence was found in 6 studies examining SE/E for adolescents and young adults with CHR or FEP. Three Level I studies (2 RCTs, 1 systematic review) examined the effectiveness of Individual Placement and Support (IPS) for youth with FEP. Both RCTs demonstrated strong evidence that when IPS was offered in addition to treatment as usual, participants had significantly better competitive employment and education outcomes than control participants (Baksheev et al., 2012; Killackey et al., 2008). The systematic review examined 28 studies with or without vocational assistance in early intervention programs and found strong evidence that supported employment services increased employment rates (Bond et al., 2015). However, extreme variability of measures used in the studies without vocational assistance made it difficult to draw conclusions on employment and educational outcomes.
Moderate evidence was demonstrated in 2 Level II studies examining vocational assistance. Dudley et al. (2014) used a naturalistic comparison design of two matched groups and found that when IPS was offered by a vocational specialist in an early intervention program, employment for participants increased during the assistance phase but declined during the 6-mo follow-up phase. In a naturalistic cohort study, comprehensive vocational assistance services led by occupational therapists resulted in significant improvements in vocational status outcomes compared with a control condition (Major et al., 2010). One Level III pre–post design study using IPS plus education in an early intervention program demonstrated insufficient evidence that vocational assistance was beneficial. Employment rates improved during the first 6 mo of a 2-yr period of support but were not sustained through the remaining 18 mo, and attrition was high (Rinaldi et al., 2010).
Family Psychoeducation
Seven studies addressing FPE provide moderate evidence for the effectiveness of these interventions in reducing symptoms and improving functioning. Three Level II studies and 1 Level III study provide moderate evidence supporting improved functioning and reduced symptoms after intervention compared with control groups. Granö et al. (2016) matched two groups and found that FPE was effective in improving functioning compared with treatment as usual (20% vs. 6%). In a multisite study by Harder et al. (2014), standard treatment plus a manualized FPE program over 3 yr versus standard treatment only resulted in significant improvement in social functioning in the intervention group. However, results were not sustained at 5-yr follow-up. A risk-based allocation study demonstrated that structured FPE in a group format, along with other program interventions, was effective in improving functioning (McFarlane et al., 2015). A Level III study found that family-oriented meetings held in natural surroundings of youth with CHR were effective in increasing overall functioning in school and work and quality of life (Granö et al., 2009).
Four Level I studies examining FPE for youth with CHR or FEP provide strong evidence that FPE improves functioning. Calvo et al. (2014) found that group FPE for youth with FEP and their families reduced relapse rates, improved negative symptoms, and renewed interest in recreation at 6-mo follow-up compared with a control condition. Both intervention and control groups showed improved functioning. At 2-yr follow-up of the same groups, effects of the intervention were sustained, and the FPE group had fewer emergency room visits than the control group (13% vs. 50%; Calvo et al., 2015).
In an RCT examining the effects of a 6-mo FPE program on communication and problem solving for youth with CHR or FEP, Miklowitz et al. (2014) found that the intervention group showed improvements in social and role functioning. Finally, O’Brien et al. (2014) studied FPE and its effects on family communication and problem-solving skills. The FPE group received structured, individual family sessions for 6 mo, and the control group received early intervention without FPE. Results indicated improved family communication during family problem-solving interactions, leading to improved occupational functioning, compared with the control group.
Discussion
The results of this review provide occupational therapy practitioners with emerging evidence to guide practice in early intervention for adolescents and young adults with SMI. Four interventions were identified—(1) CR, (2) CBT, (3) SE/E, and (4) FPE—that address improvement and maintenance of occupational performance in adolescents and young adults at high risk for schizophrenia or after a first episode of psychosis.
It is well documented that cognitive changes occur in the early stages of psychosis and in other SMIs such as depression (B. Y. H. Lam et al., 2014; R. W. Lam et al., 2014). This review found moderate evidence for the use of CR interventions to improve cognition and general functioning across occupations in the early stages of mental illness. CBT has a growing body of evidence supporting its effectiveness for youth with depression, CHR, or FEP in preventing the progression of SMI, reducing symptoms, and promoting occupational functioning.
It is also well documented that people with SMI have low employment rates and earn less than their peers without mental illness. The more serious their mental illness, the less likely they are to work, which decreases their opportunities for developing social relationships and building occupational skills (Luciano & Meara, 2014). Recent research has demonstrated strong evidence that vocational support during the CHR and FEP phases of a psychotic illness can promote positive social and occupational outcomes in competitive employment and academics (Baksheev et al., 2012; Bond et al., 2015; Killackey et al., 2008).
Occupational therapy practitioners have the necessary skills and training to provide vocational support to youth with CHR and FEP, particularly when following the evidence-based IPS model (Major et al., 2010; Porteous & Waghorn, 2007). This review found moderate evidence for the effectiveness of supported employment in improving the employment rates of those with CHR and FEP. The evidence for engagement in supported education was mixed.
FPE in various formats has been extensively researched for decades with a variety of diagnostic populations, but most often with people with schizophrenia and other psychotic disorders. Strong evidence indicates that FPE is effective in preventing relapse and rehospitalization and improves problem-solving skills and functional outcomes for people with serious, persistent mental illness (Lucksted et al., 2012). Strong evidence also exists that FPE for youth with CHR and FEP and their families can have positive results, such as symptom reduction, relapse prevention, and improved social and occupational functioning.
Implications for Occupational Therapy Practice and Research
Occupational therapy practitioners, with their roots in mental health and human development, can uniquely add to early intervention teams with their strong focus on function through occupational engagement (AOTA, 2014). This systematic review has the following implications for occupational therapy practice and research:
CR strategies should be implemented in occupational therapy practice to enhance cognition, overall functioning, and socialization for adolescents and young adults at risk for developing depression or psychosis, as well as those in the early stages of SMI. Research indicates that these strategies promote quicker recovery, prevent progression of the illness and further cognitive decline, and help clients maintain engagement in work, school, and social relationships.
At this time, it is unclear whether the positive effects of CBT are sustained over time, indicating the need for further research in this area and the potential need for booster sessions. Because CBT targets a person’s thoughts, using it as an adjunct to engagement in meaningful occupations could promote quicker recovery and prevent progression of the illness while helping clients maintain engagement in work, school, daily living activities, and social relationships. Therefore, CBT should be considered in occupational therapy practice as an adjunct modality, and further research on the long-term impact of CBT is needed.
Occupational therapy practitioners are well suited to facilitate FPE because of their unique training in promoting social and occupational functioning and engagement in meaningful activities (AOTA, 2014). Practitioners should seek out opportunities to cofacilitate FPE groups, which requires many skills they possess.
Occupational therapy practitioners should use vocational interventions, such as IPS, in their practice when working with adolescents and young adults in the early stages of SMI.
With the growing focus on the effectiveness of EIS for adolescents and young adults at risk for developing SMI, occupational therapy practitioners should conduct research that adds to the growing body of evidence and specifically targets the effectiveness of occupational therapy interventions.
Limitations
Systematic reviews are limited by the quality of the individual studies reviewed. The studies in this review had limitations in randomization, allocation concealment, and blinding of participants and researchers and risk of attrition bias. Many studies had multiple interventions, so identifying the direct effect of one particular intervention was often difficult. Although functional status was referenced in all of the included studies, the methods of measuring functional status varied greatly, making it difficult to generalize results. Lastly, the vast majority of the studies were not conducted by occupational therapy practitioners, and the specific role of occupational therapy in providing the interventions was not the focus of the studies.
Conclusion
Research demonstrates that specific interventions with clients in the earliest stages of SMI can offset cognitive impairments and improve functioning and social relationships. Occupational therapy practitioners have the specialized training and skills necessary to provide occupation-based individual and group interventions. Evidence-based practices, such as CR, CBT, FPE, and SE/E, are approaches occupational therapy practitioners should consider to make vital contributions to early intervention teams. However, more occupational therapy–focused research is needed to conclusively demonstrate the role of occupational therapy in early intervention for clients with SMI.
Supplemental Material
Supplementary material for Early Intervention in Mental Health for Adolescents and Young Adults: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.033118.pdf for Early Intervention in Mental Health for Adolescents and Young Adults: A Systematic Review by Halley Read, Sean Roush and Donna Downing in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.