
Abstract
According to the World Health Organization (WHO; 2017), more than 500 million people experience mental health disorders worldwide, including nearly 10 million adults in the United States with severe mental illness (SMI). The Substance Abuse and Mental Health Services Administration (SAMHSA; 2017) has defined adults with SMI as people age 18 or older who have a diagnosable mental, behavioral, or emotional disorder that has interfered with or limited at least one major life activity within the past year.
Most states and countries keep track of people with diagnoses and those who access services, but outcomes are modest and services fewer than needed because of cost and availability (SAMHSA, 2017; WHO, 2012, 2017). Although occupational therapy in the United States has its roots in mental health practice, over the years it has become less prevalent, and only recently have occupational therapy practitioners been reclassified nationally as providers of mental health services (American Occupational Therapy Association [AOTA], 2017).
Although societal mental health needs continue to increase, resources such as mental health providers and quality mental health care programs remain limited (SAMHSA, 2017; WHO, 2015, 2017). Many mental health care teams and clients have limited access to occupational therapy practitioners and services. Occupational therapy practitioners train in psychosocial and mental health interventions as part of their educational experiences (Accreditation Council for Occupational Therapy Education (ACOTE®; 2012). As clinicians, they provide a holistic perspective, meaningful activities, and occupation-based interventions focused on helping clients gain, regain, and sustain function in everyday life. Thus, occupational therapy practitioners are well suited to provide mental health rehabilitation services in a variety of inpatient, outpatient, and community settings as essential team members and program developers. However, understanding the effectiveness of interventions benefiting people with SMI is essential in providing the best-quality care.
The purpose of this systematic review was to update the existing Occupational Therapy Practice Guidelines for Adults With Serious Mental Illness (Brown, 2012) and provide occupational therapy practitioners with current evidence supporting interventions that improve and maintain performance and participation in activities of daily living (ADLs), instrumental activities of daily living (IADLs), social participation, leisure, and rest and sleep for people with SMI. The areas of work and education were excluded from this review and are covered in a separate review in this issue (Noyes et al., 2018). The research question addressed by this systematic review was, “What is the evidence for the effectiveness of interventions to improve and maintain performance and participation in ADLs, IADLs, social participation, leisure, and rest and sleep for people with serious mental illness?”
Method
Process
The Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guided the method for this review (Moher et al., 2015). The research question and search terms for the review were developed by the AOTA Evidence-Based Practice (EBP) Project methodology consultant, AOTA staff, and an advisory group in consultation with the review authors. The search terms were related to population (adults with SMI), mental health diagnoses, areas of occupational performance, and study and trial designs; see Table 1 for a list of key search terms. A medical librarian experienced in completing systematic review searches conducted all searches and confirmed and improved the search strategies. Databases and sites searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews.
Key Search Terms for the Systematic Review of Interventions to Improve and Maintain Occupational Performance and Participation for People With Serious Mental Illness
The EBP Project methodology consultant did the first review of the search results, eliminating all articles not relevant to the research question. These results were exported to the review authors (the authors of this article), who reviewed citations and abstracts to determine which full articles to appraise. The review authors retrieved and evaluated the full-text articles, and those selected for inclusion were abstracted in an evidence table. All tables were reviewed for quality control by the AOTA advisor and EBP Project methodology consultant and discussed with the review team.
Inclusion and Exclusion Criteria
Included in this systematic review are peer-reviewed journal articles published in English between January 2008 and June 2016 describing studies of interventions within the scope of practice of occupational therapy for adults age ≥18 with SMI. The occupational therapy scope of practice includes client-, group-, or population-based therapeutic use of everyday tasks, activities or occupations, preparatory methods, education, training, advocacy, adaptations, and remediation to promote health, well-being, and participation in daily life (AOTA, 2014). This review includes articles at Level I (systematic reviews, meta-analyses, randomized controlled trials [RCTs]), Level II (two groups, nonrandomized studies), and Level III (one group, nonrandomized) on the basis of AOTA levels of evidence consistent with those described by Sackett et al. (1996). Excluded were dissertations, theses, presentations, proceedings, and articles published prior to review, as well as articles providing Level IV and V evidence.
Data Extraction
The reviewers worked together to evaluate all articles at all stages of the review. Each reviewer performed an eligibility assessment of each article in an unblended, standardized manner. Reviewer disagreements were resolved by consensus. Synthesis of the articles consisted of a detailed reading of each and completion of an evidence table describing each study. Figure 1 shows the flow of abstracts and articles though the process, and Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) provides abstracted content from each study included in this review. The articles were grouped into occupational performance areas identified in the Occupational Therapy Practice Framework: Domain and Process (3rd ed., or OTPF–3; AOTA, 2014) and then analyzed for intervention methods and themes.
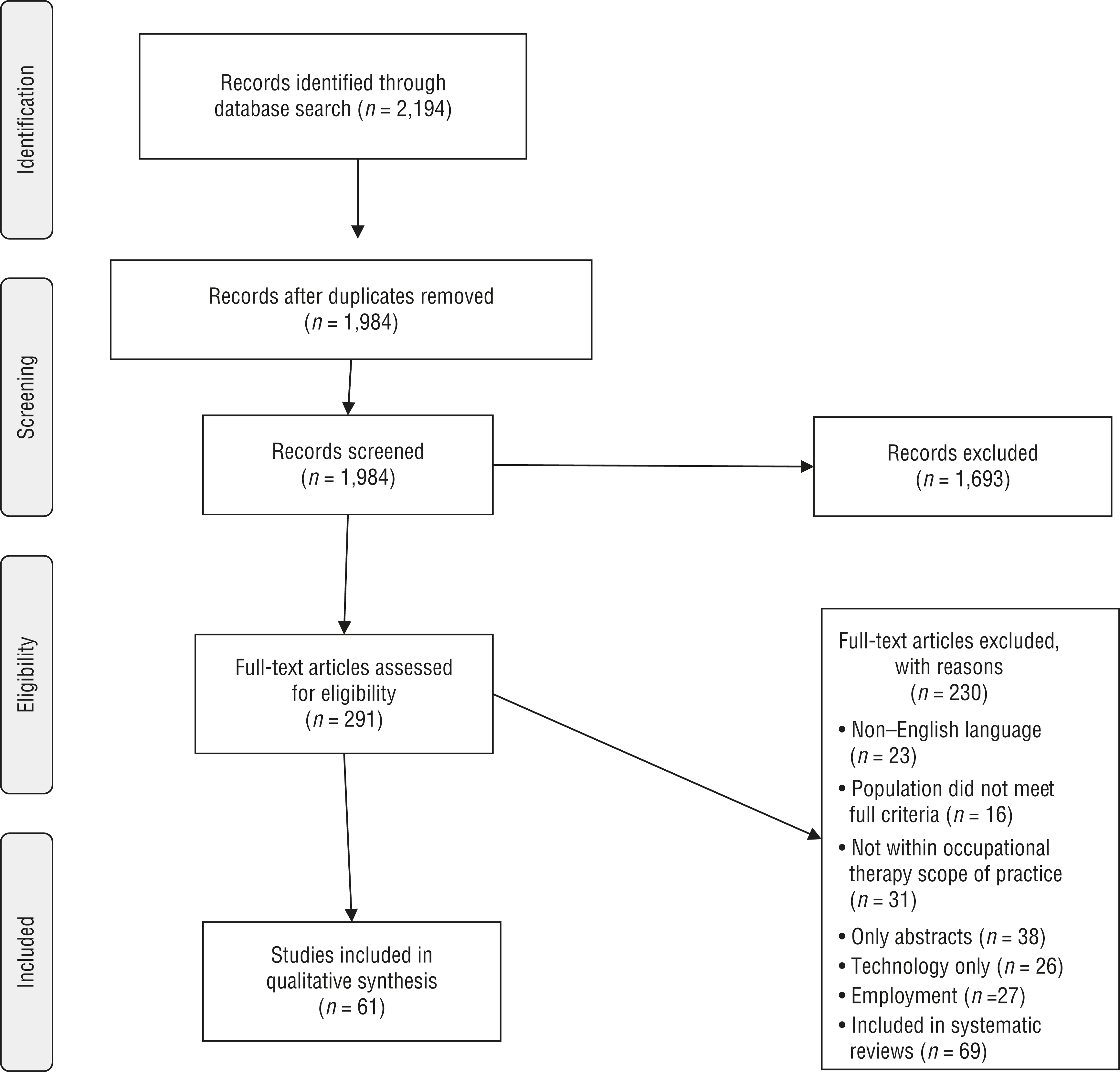
Flow diagram for studies included in the systematic review.
Analysis and Synthesis
Analysis of study design, outcomes, and risk of bias determined which studies were assessed as strong or moderate evidence. Strong evidence typically includes two or more well-designed RCTs. Moderate evidence includes one RCT, two or more studies providing lower-level evidence, or inconsistent findings from well-designed projects. Mixed evidence indicates that findings were inconsistent across studies in a given category. Limited evidence indicates few relevant studies or flaws in the available studies. Insufficient evidence indicates that the number and quality of studies are too limited to classify. Only selected articles from the systematic review are mentioned in this article; see Supplemental Table 1 for descriptions of all studies included in the review. Because of the heterogeneity of the studies reviewed, a meta-analysis was not possible; therefore, results are presented qualitatively.
Risk of Bias
The Cochrane risk-of-bias guidelines described by Higgins et al. (2011) were used to assess bias of individual studies (see Supplemental Table 2, available online). Assessment of Multiple Systematic Reviews (AMSTAR) guidelines by Shea et al. (2007) were used to determine risk of bias of included systematic reviews (see Supplemental Table 3, online).
Results
The review identified 61 articles for inclusion in the final synthesis. Risk-of-bias results using the Cochrane guidelines demonstrated higher rigor and less bias in more than half of the 50 Level I–III studies compared with the previous review (Gibson et al., 2011). However, questionable or inconsistent reporting about blinding or attrition was noted in 16 of the 39 Level I RCTs. Almost all the systematic reviews assessed for bias using the AMSTAR guidelines demonstrated high attention to rigor, especially those completed after 2010.
Five major intervention themes became apparent during the analysis: (1) occupation-based interventions, (2) psychoeducation, (3) skills training, (4) cognition-based interventions, and (5) technology-supported interventions. Along with these specific methods, several studies identified the significant benefit of individualized client-centered interventions. Many of these interventions are reported under the specific intervention themes, and several studies combined aspects or methods from multiple categories. Details of each study can be found in Supplemental Table 1. Results are reported according to intervention methods relevant to all occupational performance areas.
Occupation-Based Interventions
The evidence for the use of occupation-based interventions for ADLs and IADLs was strong, especially when addressed with individualized client-centered goals. Four studies examined occupational therapy interventions for life skills, empowerment, ADLs, IADLs, safe community participation, improved skills, and occupational goals (Clark et al., 2015; Helfrich & Chan, 2013; Katz & Keren, 2011; Thomas et al., 2011). Roldán-Merino et al. (2013) and Lindstrom et al. (2012) found that individualized interventions in residential settings significantly improved ADL and IADL performance for clients with schizophrenia. These individualized interventions addressed specific ADLs and IADLs identified by each client, such as shopping, meal preparation, and self-care, and were conducted in context.
The evidence for use of leisure activities in intervention was moderate. Studies by Carta et al. (2014) and Cramer et al. (2013) demonstrated moderate evidence for occupation-based intervention to improve leisure activities. Participants engaged in leisure activities during the intervention process, but participation was not sustained afterward.
The evidence for occupation-based interventions for rest and sleep was moderate. Rethorst and colleagues (2013) found that exercise as a daily occupation, along with medication, significantly improved sleep regardless of exercise dosage in participants with nonremitted major depression disorder.
The evidence for occupational therapy–based and occupation-based social participation interventions was strong. Five articles examined programs found efficacious for improvement in social participation and occupational engagement (Chen et al., 2015; Cook et al., 2009; Fitzgerald, 2011; Štrkalj-Ivezić et al., 2013; Tatsumi et al., 2012). Chen and colleagues’ (2015) Life Adaptations Skills Training (LAST) resulted in improvement in sleep, coping, and lifestyle and social participation, but most of the outcomes for this study were measures of symptomatology. Three studies investigating occupational therapy programs demonstrated significant improvement in social participation and occupational performance (Cook et al., 2009; Štrkalj-Ivezić et al., 2013; Tatsumi et al., 2012). Fitzgerald (2011) implemented the Social Inclusion Program (SIP) and found that participants demonstrated significant improvement in motivation for occupational engagement and patterns of occupational behavior, indicating that this occupational therapy program improved occupational performance of daily living activities and social participation in forensic services.
Insufficient evidence was found supporting animal-assisted therapy to improve social participation and engagement for people with schizophrenia. Two RCTs examined such programs and found inconsistent results (Berget et al., 2008; Chu et al., 2009).
Psychoeducation
Strong evidence supports manualized programs using psychoeducation methods to improve and maintain ADL and IADL performance. Five studies used psychoeducation as a major method of intervention for people with SMI (W. T. Chien et al., 2016; Levitt et al., 2009; Lin et al., 2013; Salyers et al., 2014). W. T. Chien and colleagues (2016) found that the adherence therapy program improved outcomes in ADLs, IADLs, relationships, and living skills. Lin et al. (2013) and Salyers et al. (2014) found that the Illness Management and Recovery program resulted in significant improvement in targeted functions of medication and illness management. Levitt et al. (2009) demonstrated that their program resulted in significant improvement in medication management, illness management, and psychosocial function. Although implementation was different across studies, all found significant improvement in functioning of intervention participants compared with control participants.
Pandor et al. (2015) and Walsh et al. (2014) found moderate evidence supporting psychoeducation programs to improve sexual activity safety. Methods included education, role-playing, and social, communication, and assertiveness skills training. Both articles reported increases in condom use, protected intercourse, and understanding of HIV/AIDS.
Response to psychoeducation interventions may vary by diagnosis. Some studies were specific to people with bipolar disorders, some had populations with varying diagnoses, and others were specific to schizophrenia spectrum disorders.
Mixed evidence was found for psychoeducation for adults with refractive bipolar disorders and schizophrenia spectrum disorders. Three systematic reviews compared psychoeducation to treatment as usual (TAU) or placebo for participants with these diagnoses and found inconsistent results (Batista et al., 2011; Bond & Anderson, 2015; Xia et al., 2013). Batista et al. (2011) found improved social function and medication adherence for some participants, Bond and Anderson (2015) found improved medication adherence, and Xia et al. (2013) found some support for psychoeducation for people with schizophrenia in these same areas.
Swildens et al. (2011) and vanderVoort et al. (2015) provided tailored client-centered psychoeducation intervention. Swildens and colleagues found significant improvement in attaining social participation goals and social contacts. VanderVoort and colleagues found increased autonomy of function and leisure but no difference between groups for social life.
Skills Training
Three systematic reviews found mixed evidence for skills training. Almerie and colleagues (2015) found mixed results on the basis of quality of studies and interventions. Gibson et al. (2011) found strong or moderate evidence, depending on the type of skills training provided, such as social, ADL, or IADL skills. Tungpunkom and colleagues (2012) found no difference in outcomes between skills training and control groups on the basis of quality of studies included. All three systematic reviews identified limited follow-up after intervention as a common limitation.
Bartels et al. (2014) and Mueser et al. (2010) implemented the year-long weekly skills training program Helping Older People Experience Success (HOPES). Both found significant improvements in community living skills, health care use, social functioning, and negative symptoms for older adults with SMI, providing moderate evidence for the HOPES program. Rus-Calafell et al. (2013) provided social skills training and found significant improvements in social skills, interpersonal communication, and quality of life.
Cognition-Based Interventions
Insufficient evidence exists for the use of cognition-based interventions to improve ADLs and IADLs. An RCT by Sánchez et al. (2014) found significant improvements in general assessment of function, cognitive performance, social competence, and functional disability, but no mention of specific ADLs, for participants in REHACOP, a program encompassing neuropsychological rehabilitation, cognitive remediation, and functional adaptation skills training.
Four studies used cognition-based intervention programs with inconsistent results. Farhall et al. (2009) and Matsunaga et al. (2010) combined cognitive–behavioral therapy (CBT) with TAU and had conflicting results. Farhall et al. found no group differences, whereas Matsunaga et al. found improved depressive symptoms and social functioning in treatment-resistant patients. Velligan et al. (2009) and Kidd et al. (2014) implemented the Cognitive Adaptation Training program, a formalized home-based intervention using environmental supports. Kidd and colleagues found significant improvements in adaptive functioning, symptoms, and goal attainment in a small sample with ongoing support from case managers. Velligan and colleagues found significantly improved grooming and hygiene among participants who used program supports compared with generic environmental supports.
Strong evidence was found for cognition-based interventions to improve and maintain performance in rest and sleep. Three RCTs and 1 Level II study found significant improvement in sleep outcomes for participants who received cognition-based interventions of mindfulness practices, breathing, and CBT (Chan et al., 2012; H. C. Chien et al., 2015; Hsu et al., 2015; Taylor et al., 2015).
Mixed evidence was found for cognition-based interventions combined with aspects of social interaction or skills training to improve social participation. Five RCTs using cognition-based interventions with a social skills or relationship component demonstrated significant improvements in social interactions, relationships, and quality of life versus social skills alone or TAU (Briki et al., 2014; Bucci et al., 2013; Granholm et al., 2013; Michalak et al., 2015; Tas et al., 2012). Ten studies evaluated social cognition-based programs (Cavallo et al., 2013; Gil Sanz et al., 2009; Granholm et al., 2009, 2014; Hasson-Ohayon et al., 2014; Horan et al., 2011; Poletti et al., 2010; Roberts et al., 2014; Taylor et al., 2016; Yip et al., 2013). All reported significantly improved cognitive functions but mixed social performance outcomes. Hasson-Ohayon et al. (2014) and Taylor et al. (2016) investigated implementation of the Social Cognition and Interaction Training (SCIT) program. Hasson-Ohayon et al. found significantly improved social engagement outcomes after combining SCIT with social mentoring. Taylor et al. found significantly improved facial affect recognition for participants with schizophrenia. A computerized cognitive remediation therapy program combined with standard rehabilitation treatment resulted in significantly improved interpersonal relations at 6- and 12-mo follow-up compared with standard treatment (Poletti et al., 2010).
A systematic review by De Silva et al. (2013) evaluated psychosocial interventions of CBT, social skills training, exercise, alternative therapies, and art therapy. They found moderate evidence for improved social functioning for participants with depression but mixed evidence for participants with schizophrenia.
Technology-Supported Intervention
Technology use as part of intervention for SMI has become more frequent, although the evidence regarding the effect on IADLs is insufficient. An RCT by Kaplan et al. (2014) addressed parenting skills online, and 2 Level II studies (Lin et al., 2008; Pijnenborg et al., 2010) reported positive results for the effectiveness of technology when combined with other interventions. No study yielded significant results, and further study is required to identify any long-term effects. Pijnenborg et al. (2010) used short text messages in addition to a psychoeducation program and found improvement in doing and maintaining IADLs, but performance dropped below baseline with withdrawal of the text messages.
Discussion
Of particular note in this systematic review is the significant increase in studies of occupation-based interventions and outcome measures and in programs implemented by occupational therapy practitioners since the AOTA systematic review by Gibson and colleagues (2011). These recent studies provide Level I, II, and III evidence. Occupation-based interventions focused on client-centered goals demonstrated better outcomes in all performance areas and social participation than programs with general expectations. Occupation-based programs created or implemented by occupational therapy practitioners had better outcomes in performance and symptomatology than TAU, whether services were provided individually or in group settings (Chen et al., 2015; H. C. Chien et al., 2015; Cook et al., 2009; Fitzgerald, 2011; Katz & Keren, 2011; Kidd et al., 2014; Lindstrom et al., 2012; Štrkalj-Ivezić et al., 2013; Tatsumi et al., 2012; Thomas et al., 2011; Tungpunkom et al., 2012).
Participants in cognition-based interventions demonstrated significantly improved problem solving and cognitive skills; however, improvement specific to ADLs and IADLs was not found. Cognition-based interventions combined with social skills, social activity, or social mentoring interventions improved social function and quality of life. Cognition-based interventions were most effective in helping participants engage in relaxation and coping for sleep preparation and rest. The evidence for the efficacy of skills-based intervention is limited by mixed outcomes, varied duration of implementation, and few long-term follow-up studies. In multiple studies, skills were found to remain intact for the duration of intervention and then dissipate without sustained use.
Manualized psychoeducation programs focused on illness management, self-management, medication adherence, and problem-solving behaviors incorporating units related to self-care and community interactions, IADLs, relationships, and communication were found to be effective. Psychoeducation programs demonstrated effectiveness; however, there are major gaps in the reporting and use of occupational performance measures. Technology-based interventions require further research.
Holistic client-centered individualized programming, whether conducted in group settings or individually provided, improved performance in ADLs, IADLs, leisure, rest and sleep, and social participation. Occupation-based programs such as SIP, HOPES, and LAST require further investigation of their effectiveness. The need remains for higher-quality occupation-based research and increased reporting of occupation-based outcome measures.
Implications for Occupational Therapy Practice
The findings of this systematic review have the following implications for occupational therapy practice:
Occupational therapy practitioners are well suited to provide holistic client-centered intervention using occupation-based, cognition-based, skills-based, and psychoeducation methods for people with SMI (see Table 2).
Occupational therapy practitioners should use evidence-based methods when providing care to people with SMI related to client needs.
Occupation-based programs provided by occupational therapy practitioners or other mental health care team members demonstrate better occupational performance and health outcomes whether services are provided individually or in group settings.
Occupational therapy practitioners should be involved in program development for people with SMI in inpatient, outpatient, and community-based settings to support engagement in recovery and wellness through occupational performance.
Technology-supported interventions require further investigation.
Summary of Intervention Recommendations to Improve and Maintain Occupational Performance and Participation for People With Serious Mental Illness
Implications for Research
The findings of this systematic review have the following implications for occupational therapy research:
Gaps persist in the research, and rigorous studies are needed to investigate occupation-based outcome measures specific to ADLs, IADLs, leisure, and rest and sleep.
Many studies recognized the complexity of mental health care for people with SMI; combined intervention methods need to be studied further.
Function is still reported in a general fashion rather than in relation to occupational performance as defined by the OTPF–3 (AOTA, 2014).
Symptom measurement as outcome remains predominant, and future studies need to focus on measurable functional outcomes.
Limitations
Limitations of this systematic review result from the individual studies’ limitations in design, method, outcome measures, sample size, and length of interventions. Many studies focused primarily on reduction of symptoms for people with SMI and failed to report occupation-based outcomes.
Conclusion
Occupational therapy practitioners working with people with SMI have strong evidence to support current practice and improve future practice. More research is needed focusing on measurement of occupational performance changes, length of intervention, and length of sustained performance after intervention.
Supplemental Material
Supplementary material for Evidence for Interventions to Improve and Maintain Occupational Performance and Participation for People With Serious Mental Illness: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.033332.pdf for Evidence for Interventions to Improve and Maintain Occupational Performance and Participation for People With Serious Mental Illness: A Systematic Review by Mariana L. D’Amico, Lynn E. Jaffe and Jennifer A. Gardner in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman, program director of the AOTA Evidence-Based Practice (EBP) Project, for her guidance and support during the process of this review; Marian Arbesman, EBP Project methodology consultant (2005–2017); Gary Kaplan, the medical librarian who conducted the searches for this project; Beth Hunter, the current EBP Project methodology consultant; and Mirtha Whaley for contributions to some tables. No potential conflicts of interest are reported.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.