
Abstract
A landmark study by Colton and Manderscheid (2006) found that people with serious mental illness (SMI) die an average of 25 yr earlier than the general population. Most of these deaths are attributable to medical causes similar to the leading causes of death for the general population, including cardiovascular disease and cancer. Cardiovascular disease in particular is linked to preventable conditions, including obesity.
Overweight is defined as a body mass index (BMI) of 25.0 to <30.0, and obesity is defined as a BMI of 30.0 or greater (Centers for Disease Control and Prevention, 2016). Obesity rates are alarmingly high in the general population, and the prevalence of obesity is even higher among people with SMI. A systematic review found that the median prevalence of obesity in people with SMI was 40.6%, compared with 35.4% in the general population (Janssen et al., 2015).
Many factors contribute to high rates of obesity in the SMI population. Most people with SMI take antipsychotic medications, and all antipsychotic medications are associated with weight gain, with second-generation antipsychotics tending to have the worst side effect profile (Manu et al., 2015). People with SMI commonly lead more sedentary lifestyles, which is partially attributed to affective factors such as depression and anxiety (Jerome et al., 2009), and they tend to have poor diets that are low in fiber and fruit and high in saturated fat (Dipasquale et al., 2013). Challenges to healthy eating are compounded by low socioeconomic status, because more nutritious foods, such as fruits and vegetables, tend to be more expensive. The combination of all of these factors makes weight loss challenging for people with SMI.
The significance of the problem points to the need for weight loss programs for people with SMI. Many weight loss interventions are available to the general public, ranging from medications to individualized diet and exercise programs; however, many of these interventions are not ideal for people with SMI for reasons including cost and lack of attention to the particular needs of the population (e.g., cognitive impairments, use of medications, stigma). Consequently, a substantial and growing body of research, including systematic reviews, has examined weight loss interventions for people with SMI. However, many of these studies have been carried out in inpatient settings. Although it may be easier to control many factors that influence weight loss in an inpatient setting, it is more practical for people to receive weight loss interventions in community-based settings because the majority of people with SMI receive their services in such settings (Casagrande et al., 2010). In addition, many relevant studies have become available, and because of the sizeable number of studies, it is possible to limit the review to higher-quality randomized controlled trials (RCTs). The present systematic review sought to review the current literature focused on people with SMI and weight loss in the community.
Method
This systematic review is part of the series of reviews sponsored by the American Occupational Therapy Association (AOTA) Evidence-Based Practice (EBP) Project (Lieberman & Scheer, 2002). A major focus of the EBP Project is an ongoing program of systematic reviews of multidisciplinary scientific literature, using focused questions and standardized procedures to identify occupational therapy–relevant evidence and discuss its implications for practice, education, and research. An evidence-based perspective is founded on the assumption that scientific evidence of the effectiveness of occupational therapy intervention can be judged to be more or less strong and valid according to a hierarchy of research designs, an assessment of the quality of the research, or both.
A systematic review on adults with mental illness supported by AOTA as part of the EBP Project included five research questions. The questions were reviewed by review authors, an advisory group of experts in the field, AOTA staff, and the methodology consultant to the AOTA EBP Project. One question—What is the evidence for the effectiveness of interventions to improve physical health and wellness and the integration of care for people with serious mental illness?—led to the identification of four themes: (1) general wellness, (2) exercise, (3) yoga and relaxation, and (4) weight loss. This systematic review addresses the weight loss theme.
Search Strategy
Search terms for the reviews were developed by the review authors, the methodology consultant to the AOTA EBP Project, AOTA staff, and the advisory group. The search terms were developed not only to capture pertinent articles but also to make sure that the terms relevant to the specific thesaurus of each database were included. Table 1 lists the key search terms related to the population (serious mental illness) and types of interventions specific to the weight loss theme. A medical research librarian with experience in completing systematic review searches conducted the initial search, and the review team followed up with additional searches. Databases and sites searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews. Additionally, reference lists from included studies were examined.
Key Search Terms for the Systematic Review of Interventions for Weight Loss for People With Serious Mental Illness
Inclusion and exclusion criteria provide the structure for the quality, type, and years of publication of the literature that is incorporated into the review. The review was limited to peer-reviewed scientific literature published in English. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. The interventions had to be community based and within the scope of practice of occupational therapy. If participants had undergone surgical intervention or were undergoing pharmacological intervention for weight management, these studies were excluded. Only studies that were published since 2008 were included because a previous systematic review and practice guidelines by AOTA included studies up to that date (Brown, 2012).
Study Selection, Data Extraction, and Risk-of-Bias Assessment
The review authors (the authors of this article) eliminated references on the basis of citations and abstracts and then retrieved full-text versions of potential articles to determine final inclusion in the review on the basis of the predetermined inclusion and exclusion criteria. Any discrepancies were resolved through consensus.
Two reviewers (authors Geiszler and Lewis) reviewed the articles independently and extracted the necessary data for the evidence table, risk of bias assessment, and meta-analysis. The reviewers extracted data and resolved any discrepancies through consensus or, when necessary, through discussion with a third reviewer (author Brown). AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. All studies are summarized in full in Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). The risk of bias of individual studies was assessed using the methods described by Higgins and colleagues (2011; see Supplemental Table 2 online). The method for assessing the risk of bias of included systematic reviews was based on the measurement tool developed by Shea et al. (2007; see Supplemental Table 3 online).
Data Analysis
The outcome of weight loss was analyzed using a meta-analysis and Comprehensive Meta-analysis software (Biostat, Englewood, NJ). To compare study outcomes, the effect sizes for weight loss were calculated for each study using Cohen’s d. The overall effect size from all studies for which data were available was calculated for weight loss. A forest plot was constructed to graphically compare individual study results and their effect sizes with the overall effect.
Some studies (Cordes et al., 2011; Masa-Font et al., 2015; Pagoto et al., 2013) were not included in the meta-analysis because they did not provide the necessary data; however, these studies provided useful information for answering the research question. These studies, along with the studies included in the meta-analysis, were also synthesized qualitatively to identify similarities related to participants, interventions, and outcomes.
Results
The search initially resulted in 231 articles. After examining titles and abstracts, 28 full-text articles were reviewed. Five systematic reviews were eliminated because although the review was published after 2008, none of the studies included in the review met the criteria of publication after 2008. After applying inclusion criteria to the remaining articles, 19 articles were identified for inclusion in the review, including 17 studies and 2 systematic reviews (Figure 1). Fourteen studies were used to complete the meta-analysis (Figure 2). Individual studies excluded from the meta-analysis included Cordes et al. (2011), because unlike the other studies, their intervention focused on preventing weight gain instead of promoting weight loss; Masa-Font et al. (2015), because the study did not report weight loss as an outcome (although it did report changes in BMI); and Pagoto et al. (2013), because although two groups were compared, both groups received a lifestyle intervention (with one group receiving the lifestyle intervention plus behavior therapy). These studies are included in the qualitative analysis of the data.
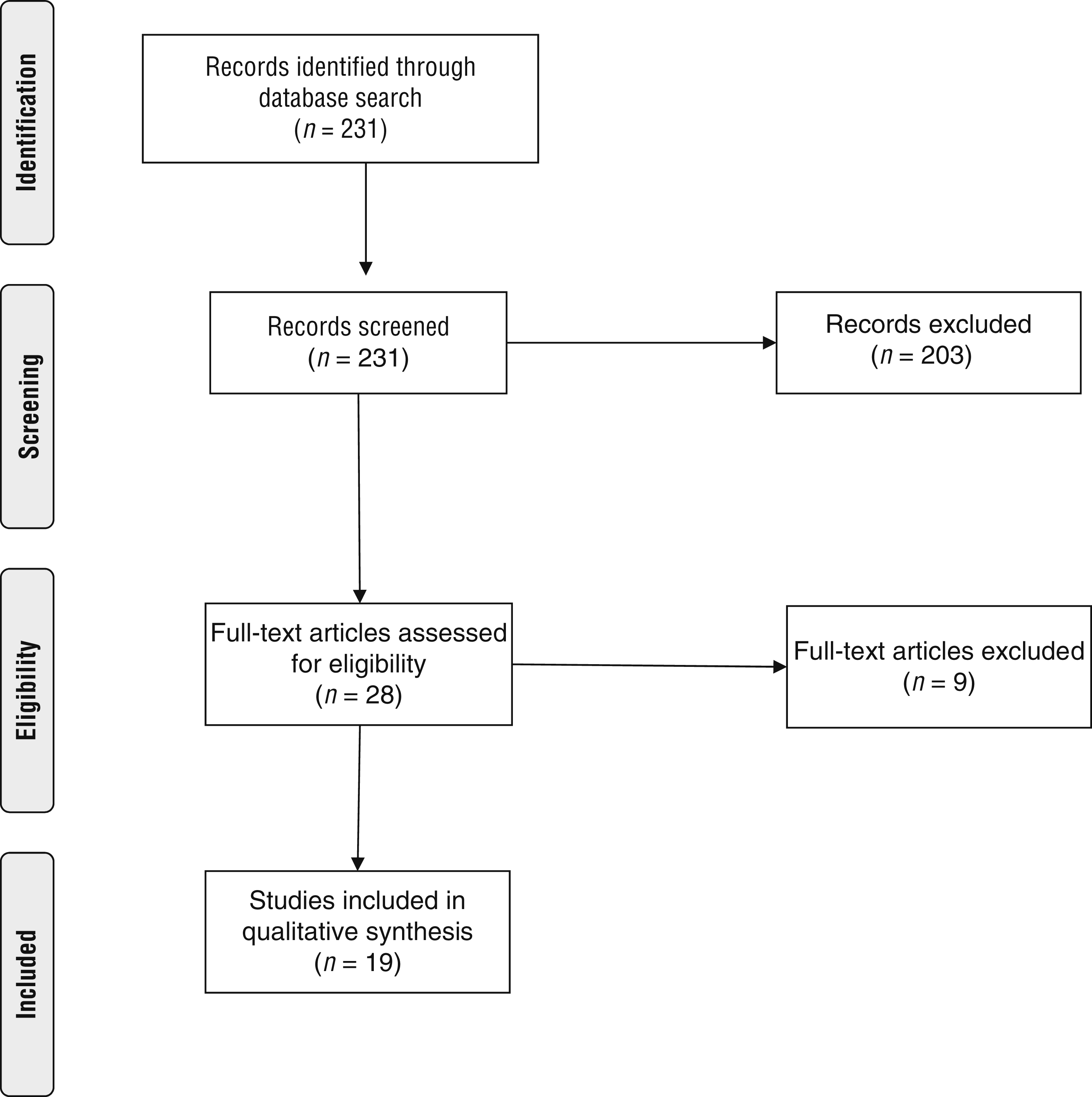
Flow diagram for studies included in the systematic review.
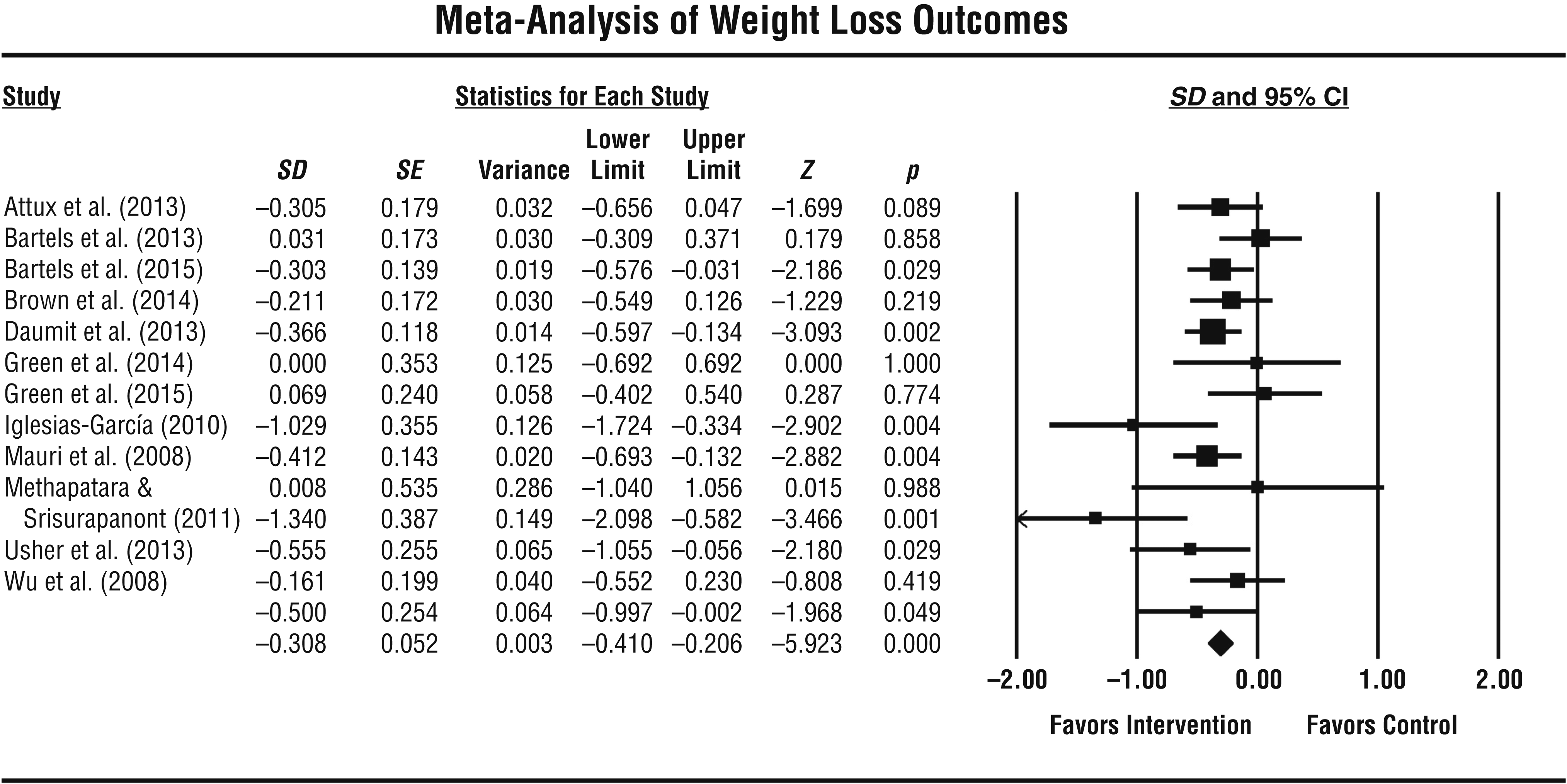
Meta-analysis of weight loss outcomes.
Two other studies merit additional explanation for the meta-analysis. In Forsberg et al. (2008), the intervention included both residents and staff at supported housing sites. However, to be consistent with the other studies, only data for the residents (who met the criteria of having SMI) were included in the study. Wu et al. (2008) included four groups in their study; one intervention group received a weight loss medication, another received the medication plus a lifestyle intervention, a third received the lifestyle intervention alone, and the control group received a placebo only. For the purposes of this review, the data from the lifestyle only group and the control group were included in the meta-analysis.
Overview of the Studies
All studies included in this review used various lifestyle interventions focused on weight loss. These interventions included a range of components such as exercise, educational sessions, motivational interviewing, mentor programs, behavior therapy, and diet changes; however, there were some similarities across the instructional methods. The instructional component of the interventions acknowledged the need to accommodate possible cognitive concerns common in the population (e.g., topics were broken down into smaller components, key points were repeated). In addition, the interventions typically focused on changing a few key behaviors (e.g., eating at least five servings of fruits and vegetables, decreasing sugary drinks), although the targets varied across the interventions.
The length of the interventions differed greatly, from 12 wk to 18 mo. The interventions were carried out in either group sessions or a combined approach of group and individual sessions. The sample sizes for the individual studies ranged from 15 to 291 participants. The mean age range for the studies was 25.8–53.5 yr, with most studies having a mean age in the 40s. The gender of participants ranged from 18% to 71% male, and most studies had more female than male participants. The amount of weight change for the intervention groups ranged from –9.9 to +3.8 lb. Details for each article can be found in Supplemental Table 1.
Of 14 studies that reported weight loss and compared an intervention and true control group, 7 studies found a statistically significant difference between the intervention and control group during at least one time point (Bartels et al., 2015; Brown et al., 2014; Daumit et al., 2013; Green et al., 2014, 2015; Mauri et al., 2008; Methapatara & Srisurapanont, 2011). Brown et al. (2014) is the only study that reported including an occupational therapist in the development of the intervention. However, only 1 of the studies (Goldberg et al., 2013) did not result in mean weight loss for the intervention participants during at least one time point. Several of the studies reported weight loss across multiple time points; however, the direction of the weight loss varied among the studies. All of the studies with multiple time points reported weight loss early in the intervention, with 4 studies finding increasingly greater weight loss over time (Attux et al., 2013; Bartels et al., 2015; Daumit et al., 2013; Green et al., 2015) and 3 studies finding initial weight loss but some weight gain over time (Bartels et al., 2013; Brown et al., 2014; Iglesias-García et al., 2010).
The 1 study reporting only BMI and not weight loss (Masa-Font et al., 2015) did find a difference between groups; however, it was the control group that experienced a greater change in BMI. The study comparing a lifestyle intervention to a lifestyle intervention plus behavior therapy found that both groups lost weight, with no significant difference between groups (Pagoto et al., 2013). The 1 study examining prevention of weight gain did not find a difference between groups (Cordes et al., 2011).
Two systematic reviews were included in this review. Bruins et al. (2014) included a meta-analysis and found that weight loss interventions had a moderate long-term effect on weight loss compared with control conditions (p = .02). This review also examined prevention of weight gain programs and found a large effect (p = .0002). Krogh et al. (2014) focused exclusively on exercise interventions and found little evidence of weight loss.
Several studies found benefits outside of weight loss for the intervention group. Three studies found improvements in fitness levels (Bartels et al., 2013, 2015; Masa-Font et al., 2015), and 2 studies found better fasting glucose levels (Cordes et al., 2011; Green et al., 2015). Pagoto et al. (2013) reported improvements in depression.
Meta-Analysis
The 14 studies included in the meta-analysis had a total of 1,578 participants. The data entered for the calculation included the total weight lost at the end of the intervention, which did not necessarily reflect the time point at which the greatest weight loss occurred. Effect sizes were calculated, and a negative effect size reflects a positive weight loss outcome. The individual study effect sizes ranged from –1.340 to 0.069. The overall effect size of the interventions on weight loss was –0.308 (Figure 2), representing a small to medium effect size (Cohen, 1992). Overall, the various lifestyle-focused interventions had a significant effect on weight loss (p < .001).
The forest plot (Figure 2) depicts the standardized difference in means for the intervention and control groups for each study individually and the total effect when all studies are combined. The size of the square for each study indicates the weight or importance of that study for the overall effect, which is largely influenced by the sample size of the study. A value of 0.00 indicates no difference between the groups, whereas a negative number favors the intervention group and a positive number favors the control group. Most of the studies’ results favored the intervention group, indicating that the intervention group lost more weight than the control group. Bartels et al. (2013), Forsberg et al. (2008), and Goldberg et al. (2013) had more neutral findings indicating little difference between the intervention and control groups. The confidence intervals are indicated numerically by the lower and upper limit values and graphically by the lines that emanate from the squares in the graph. A large confidence interval indicates more variability within the group (i.e., the amount of weight loss differed for participants in the group). The forest plot indicates that many studies had large confidence intervals.
A fail-safe N was calculated on the basis of the procedures outlined by Orwin (1983). Orwin’s fail-safe N estimates the number of unpublished studies reporting null results needed to reduce the cumulated effects across studies to a specified level. The specified level in this case was an effect size of 0.20, representing a small effect. The fail-safe N indicates that 8 studies (or more than 50% of the number of actual studies included in the meta-analysis) with null results would be needed to obtain a reduction in effect size to 0.20.
The studies with the largest effect sizes were Mauri et al. (2008), with an effect size of –1.34 and weight loss of 9.9 lb, and Green et al. (2014), with an effect size of –1.029 and weight loss of 6.7 lb. Both of these studies were shorter-term studies of 24 and 12 wk, respectively, with interventions that included educational and practice components of lifestyle change with a heavy emphasis on specific dietary recommendations. However, 2 other studies to note include Bartels et al. (2015) and Daumit et al. (2013), which stand out in terms of their weight in the meta-analysis, effect size, smaller confidence intervals, and weight loss. These studies are similar in that both were longer-term studies of 12 and 18 mo with weight loss of 5.3 lb and 7.48 lb, respectively. The interventions in these studies were similar in that they were longer term, targeted both nutrition and physical activity lifestyle changes, and included a group and an individual component.
Discussion
This review examined the effectiveness of weight loss interventions delivered in community-based settings for people with SMI. The meta-analysis found a statistically significant difference in overall amount of weight loss between the intervention and control groups; however, the amount of weight lost was relatively small. Although most participants in the studies did not meet the criterion of weight loss of >5% of body weight for metabolic changes to be expected (Franz et al., 2015), people are likely to receive other benefits from participating in a weight loss intervention. Note that individual variability in weight loss exists, and the mean loss is not representative of every person. Furthermore, the goal of preventing further weight gain has its own impact on health.
In addition, the amount of weight loss found in this review is consistent with weight loss studies for the general population. An important systematic review (LeBlanc et al., 2011) found an average weight loss of 6.6 lb in behavioral weight loss studies for the general population. The studies with the greatest effect sizes in this review were comparable to (Bartels et al., 2015; Green et al., 2014) or exceeded (Mauri et al., 2008; Daumit et al., 2013) the findings of the LeBlanc et al. (2011) review.
Results of the meta-analysis showed that overall the interventions did result in weight loss with a small to medium effect size. In addition, the weight loss interventions found positive results related to fitness levels, glucose metabolism, and depression. With systematic reviews such as this, additional focus can be placed on factors that appear to be most important for improving weight loss outcomes.
Although there was great heterogeneity among the interventions used and the durations of the interventions in the different studies, some common elements were identified that require further investigation. The greatest effect sizes were found in two short-term studies that focused on specific dietary recommendations (Green et al., 2014; Mauri et al., 2008). The long-term studies that resulted in the greatest effect sizes were those that used a combined group and individual approach. Previous research with the general population suggests that group-based interventions are more effective than individual interventions for obese adults (Paul-Ebhohimhen & Avenell, 2009; Renjilian et al., 2001). We could not identify studies in the general population that looked at a combined approach. For the population in this review—people with SMI—the combined approach may be more effective because of the need to individualize instruction and provide additional support and reinforcements. The added benefit of individual approaches may be vital to the success of interventions for this population.
A systematic review by Bruins et al. (2014) included in this review yielded similar results, demonstrating reliability of the findings. Both reviews showed an overall effect size that supported lifestyle interventions for weight loss. Both also support the use of combined group and individual interventions. One difference was the magnitude of the effect size, with Bruins et al. (2014) finding a greater effect.
Implications for Occupational Therapy Practice
On the basis of the evidence contained in this systematic review, the following recommendations are made for implementation of community-based interventions targeting weight loss for people with SMI:
Approach the process of weight loss realistically with participants, acknowledging the variability in amount of weight loss that will occur among individuals.
Include content that addresses behavioral changes related to both nutrition and physical activity.
Focus content on a few key goals of behavioral change, including specific dietary recommendations.
Modify instruction on dietary recommendations and physical activity to account for common cognitive impairments seen in people with SMI.
Include a combined approach of group and individual sessions that occur at least weekly and for at least 12 mo.
Implications for Future Research
This review indicates that people with SMI can lose weight with targeted interventions; however, more research is needed to determine the most effective approaches and amount of time needed to achieve weight loss goals. Only 1 study in the review involved an occupational therapist (Brown et al., 2014). Greater involvement by occupational therapy practitioners in the development of weight loss interventions and then study of those interventions using RCTs could contribute to a better understanding of what aspects of weight loss interventions are most important. For example, occupational therapy practitioners have the expertise to develop interventions that address the cognitive impairments associated with SMI and promote lifestyle changes through the promotion of healthy routines. In addition, none of the interventions specifically addressed the role of culture in weight loss and weight gain. Because food and activity are linked to culture, occupational therapy interventions have the potential to be sensitive to the cultural needs of participants (Dillard et al., 1992).
Limitations of the Review
There were limitations in our review design and in the studies included. One of the most significant limitations encountered was that several studies that fit our criteria had to be excluded from the meta-analysis because of lack of adequate data to calculate the effect size. In addition, unpublished research was not included in this review.
Variability in study duration, intervention content, and intervention strategies used made it difficult to make side-by-side comparisons of the studies and therefore difficult to draw specific conclusions about the most important ingredients of a weight loss intervention. Future research is needed to determine the effectiveness of individual intervention components and to identify strategies to increase the amount of weight lost and the maintenance of weight loss over time.
Conclusion
Overall, community-based interventions for people with SMI are effective for weight loss. Some features of the most effective interventions are provision of nutrition and exercise components with specific dietary recommendations, at least weekly sessions, and a combined group and individual approach. The interventions included in this review are within the scope of occupational therapy practice. Occupational therapy practitioners can provide weight loss interventions to address the wellness needs of their clients. Because more research is needed, occupational therapy practitioners should contribute to the continued development and study of weight loss interventions for people with SMI.
Supplemental Material
Supplementary material for Effectiveness of Interventions for Weight Loss for People With Serious Mental Illness: A Systematic Review and Meta-Analysis
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2018.033415.pdf for Effectiveness of Interventions for Weight Loss for People With Serious Mental Illness: A Systematic Review and Meta-Analysis by Catana Brown, Lydia C. Geiszler, Kelsie J. Lewis and Marian Arbesman in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman for her guidance and support during the systematic review process and Barbara Nadler for her assistance with the search. This systematic review was presented preliminarily at the 2017 AOTA Annual Conference & Expo, Philadelphia.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.