
Abstract
The author describes personal and professional milestones in becoming an occupational therapist and his early experience in the first behavior disorder program for neurologically based aggression in the world. A real clinical example is used to bring these early lessons into vivid focus. New evidence underlines occupational therapists’ unique role in skill–habit training in clients with severe neurological impairment. For clients with milder impairments, irrespective of diagnosis, strategy training may maximize community independence and reduce hospital recidivism. The concept of functional cognition is described as an important development for the profession. Even in an environment of rapid innovation, occupational therapists need to recognize that it is the commonplace activities that have meaning for the individual that really matter. This is both the art and science of occupational therapy, and it will never be superseded by technological innovation because true creativity and genuine empathy cannot be mechanized.
Gordon Muir Giles, PhD, OTR/L, FAOTA

Much of what occupational therapy practitioners do involves training skills–habits or teaching strategies. In this Eleanor Clarke Slagle Lecture, 1 I focus on work with adult neurological populations to illustrate these treatment approaches, but much of this discussion also applies to other client populations. So my hope is that most readers will find something in what follows that is relevant to their practice. After some brief personal reflections, I describe working with a very challenging client and how this work influenced my thinking. The main part of this lecture focuses on how skills- or strategy-based approaches can be used to improve clients’ occupational performance. I then discuss the concept of functional cognition as a link between those two constructs, and I conclude with some further personal reflections.
Becoming an Occupational Therapist
My parents were paranoid, and their outlook had a powerful influence on my personal and professional life. Like most parents, they were doing the best they could, or at least what made sense to them, but growing up around them was difficult. They were not mentally ill, but the fundamental attribution error (FAE) dominated their thinking.
The FAE is the tendency to view other people’s unpleasant, irritating, or obnoxious behavior as both fully under their control and the result of moral weakness (Ross, 1977), whereas when we engage in similar behaviors, we account for these behaviors as accidental, unintended, or an unavoidable reaction to circumstance (i.e., we make dispositional attributions and ignore situational constraints; Jones & Harris, 1967). The more threatening and uncomfortable we find the other person’s behavior, the more likely we are to display the FAE and to hold the other person morally culpable (Manchester, 2002).
My parents were convinced that anything others did that caused them even mild irritation was the result of that person’s willful malevolence. Although I found this philosophy unappealing, I also found myself rather lost, and this feeling of not knowing quite who I was or who I wanted to be continued through my undergraduate studies until I found myself in occupational therapy school.
In the United Kingdom in the 1980s, students were admitted directly from high school to occupational therapy programs. However, I was lucky enough to be one of the first four students with a bachelor’s degree to be admitted to an occupational therapy program. I attended St. Andrew’s School of Occupational Therapy on the grounds of St. Andrew’s Hospital, at the time the United Kingdom’s premier psychiatric hospital. I was excited to be there, but after a couple of weeks in the program, I told the director that I was restless and needed more to do. She was really good with me and suggested that I volunteer at Kemsley, a new unit on the hospital grounds for people with neurologically based behavior disorders (mostly from traumatic brain injury [TBI]). I volunteered, and after I graduated I joined the Kemsley rehabilitation team.
Early Lessons From Learning Theory and Social Psychology
The interventions at Kemsley centered around a token economy (Eames & Wood, 1985a, 1985b). Clients could earn tokens that could be traded for special food or other rewards in an attempt to reduce verbal and physical aggression and to foster prosocial behaviors. I had doubts that the token economy contributed much to clients’ improvements, but it provided a holding environment for staff and guided us when otherwise we would not have known what to do.
The work was enthralling. For one thing, every client care conference became a debate over some nuance of learning theory. Also, I felt that I could understand the clients’ behavior. I tend to be concrete in my thinking, so when, for example, a client was urinating into the trash can, it seemed obvious to me that it was because the trash can was in a corner of the room, and round, and white, and looked like a toilet—it just seemed so obvious. It bewildered me that some of my colleagues did not recognize the causes of clients’ behavior. Some colleagues, despite being kind and caring professionals, appeared to take clients’ behavior as a personal affront. The idea that so much could be lost as a result of a TBI—something that could happen to anyone, that could be the result of an accident, and that could happen to their own loved ones—was so frightening that these colleagues could not tolerate the idea, so instead they came to believe that clients’ behavior was both deliberate and willful. I have now come to understand this response to be the result of the FAE.
Another thing that made working at Kemsley exciting was that we were attempting to use learning theory–based interventions with clients recovering from severe TBI. Because at the time no clinical intervention had been shown to work with this population, we looked at what evidence there was about how neurologically healthy people learn skills. In the 1940s and 1950s, Clark Leonard Hull, a psychology professor and researcher from Yale University, demonstrated in animals and in neurologically healthy adults that the relationship between repetition and habit development follows an asymptotic curve in which there is increasing automaticity with repetition (Clark-Wilson et al., 2014; Hull, 1943, 1951; Lally et al., 2010). These findings were promising, but we still had no evidence that the same principles applied to clients after severe TBI, and from a clinical viewpoint our clients’ obviously impaired conscious recall suggested that learning might not be possible.
But in 1980, shortly before Kemsley opened, Edgar Miller, a physician working at Addenbrooke’s Rehabilitation Hospital in the United Kingdom, published an article on the learning characteristics of adults with severe TBI (Miller, 1980). Miller used the Minnesota Spatial Relations Test (MSRT; American Guidance Services, 1979) to examine how quickly neurologically healthy participants and participants with severe TBI (all of whom had posttraumatic amnesia [PTA] in excess of 14 days) could complete the four form boards that made up the MSRT across learning trials. Figure 1 shows that compared with the healthy control participants, those with severe TBI started out being very slow, but that after continued practice their level of performance approximated that of the neurologically healthy participants. What we took from this work was that people with severe TBI could learn skills. And being occupational therapists, we were not interested in teaching them how to complete form boards; we wanted to know whether we could use learning theory–based interventions to teach clients activity of daily living (ADL) and instrumental activity of daily living (IADL) skills after severe TBI, something that in the mid-1980s had not been tried before.
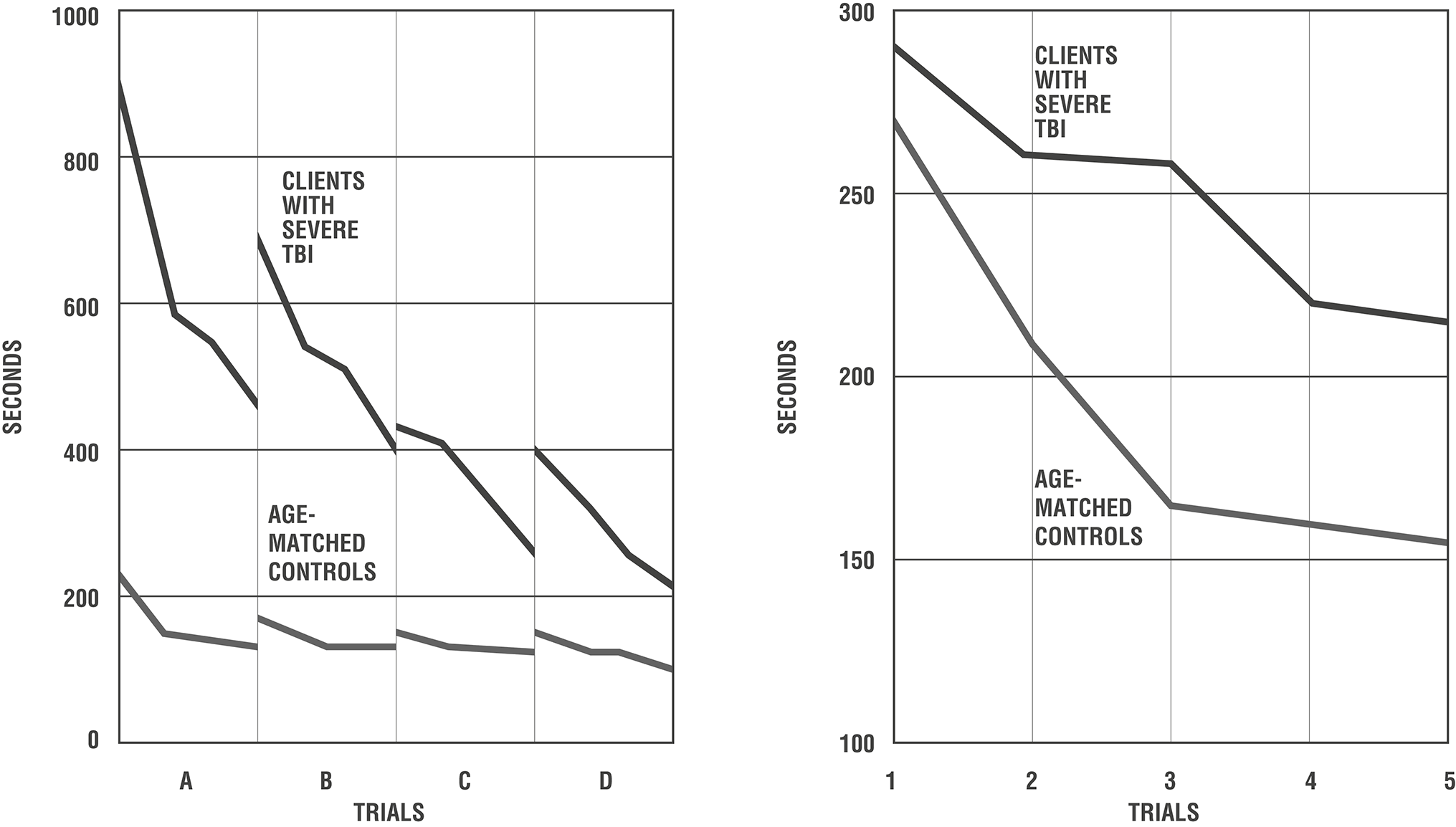
Left: Mean times on successive trials on the four form boards of the Minnesota Spatial Relations Test. Right: Relative rates of learning of the neurologically healthy control participants and participants with severe TBI when matched for initial performance levels.
The client on whom I will focus, whom I will call Dave, did not have a TBI. Dave had been a student in mechanical engineering, and at 6 ft 6 in. tall was training for a U.K. Olympic team. One day, when Dave was 24 years old, he told his mother that he felt light-headed and that he “smelled a funny smell.” Four days later, after a grand mal seizure, he was admitted to his local hospital in a delirium, and 2 days after that he was transferred to the Royal Hospital for Neurological Diseases in Queen Square, London (Greenwood et al., 1983).
Dave had herpes simplex encephalitis (caused by the cold sore virus), which, once in the brain, has a particular affinity for midbrain and medial temporal lobe structures (Damasio & Van Hoesen, 1985; Gnann & Whitley, 2017). Dave was treated with the antiviral medication acyclovir, and as he began to recover, the consequences of the infection and resulting brain damage became apparent. He was hyperoral and constantly hungry, and he had a category-specific semantic disorder for biological entities (i.e., living things and food; Bunn et al., 1998; Warrington & Shallice, 1984). Dave couldn’t tell the difference between food and nonfood objects: He would attempt to eat his bedsheets and drink shampoo or the urine from his urinal.
By the second month of his hospitalization, he had made a full physical recovery, but he had profound memory impairment and could not retain information for more than a few seconds. One of his therapists suggested that he compensate for his memory impairment by writing things down. He was also depressed, irritable, and physically aggressive. On at least two occasions he asked his parents to help him commit suicide.
Dave was discharged home to the care of his mother, but things began to deteriorate almost immediately. His attitude toward those around him could best be characterized as sullen lack of cooperation. But he had taken the therapist’s advice to heart and was obsessive about writing everything down in his “diary” “before I forget.” Unfortunately, Dave never read anything he had written, so the diary served no practical purpose. Rather, it consisted of a continuous bitter commentary on the futility of everything that he was being asked to do.
One day, when his mother told him that they were going to go out shopping, but then stopped to answer the phone, Dave chased her into the upstairs bathroom with a kitchen knife, yelling, “You made me lie in my diary!” A neighbor, hearing the screaming, called emergency services.
Dave spent the next 5 years going from one psychiatric hospital to another and being sedated with antipsychotic medications, from which he developed the movement disorder tardive dyskinesia, until eventually he was admitted to Kemsley. Did I mention that Dave was 6 ft 6? Anyway, he was a big, angry guy, and when he arrived at Kemsley he was a pretty intimidating figure. He would stand over me, glaring down with his odd shoulder and facial movements and huffing and snorting from the tardive dyskinesia, exclaiming, “How long does it take for a pointless place to admit they can’t help your illness?”
Dave was still constantly writing things down but not reading what he had written. On a couple of occasions, I got to read what he had written about me, which usually began, “The big blond bastard has just told me to . . .” (see Figure 2). Dave was indignant and resentful in general, and he would not do anything that we asked him to do, including participate in any form of therapy. His entire attention was focused on writing down how we did not know what we were doing and how we were conspiring against him—though he used more colorful language to express these ideas. It is not that he was wrong. We truly did not know how to help him, and from his perspective, we were conspiring against him. But his focus on these beliefs prevented him from seeing any way forward.
The “big blond bastard”: The author at age 22 with a perm (it was the 1980s, and that is what people did). People lose a lot when they age: At 60, I can no longer summon the level of petulance that is evident in this photo.
The staff at Kemsley made many attempts to engage Dave in therapy, and finally and with great reluctance we came to the conclusion that to get Dave to participate in rehabilitation, we would have to divert him from his preoccupation with writing things down. We decided to take away his diary. Because by this point there was no actual diary, just any paper that he could get ahold of, what this really meant was that we had to remove all of the paper and writing implements he might be able to access. We were disturbed about taking away one of his only coping mechanisms but could not see any other solution.
The week we took away his diary, he was repetitively physically assaultive, but the next week the assaults were less frequent. The week after that, we found him occasionally stealing pens and trying to write notes on bathroom tissue, but we were able to interact with him, and we felt that at least there was the potential that we could work with him.
Among his other problems, Dave was markedly malodorous, making him even more difficult to be around. But we observed that he would decide not to bathe on the basis of attempted verbal self-regulation: He would look out of the window and say, “It is snowing outside, so I can’t have been sweating, so I don’t need to bathe.”
Even when Dave attempted to bathe and dress, it did not go well. Dave was physically capable of doing everything required to bathe and dress, but he could not organize the subtasks of bathing and dressing into an effective morning hygiene routine. His memory impairment was so severe that on one of the baseline recording days, he brushed his teeth 8 times in a row. Each time he finished brushing, he immediately forgot what he had just done but then noticed that his teeth felt funny, so he brushed them again, and again, and again, until some unknown impulse led him to interrupt this pattern and to wash his face, something he also had already done.
Using verbal self-regulation as a rehabilitative intervention was popular at the time (Cermak, 1976; Wilson, 1984), and because Dave attempted to verbally self-regulate spontaneously, a psychology intern and I thought we might attempt to use verbal self-regulation in a retraining program. The goal of self-regulation interventions was to have the client say and then do. However, despite learning to say the words, clients trained with this method often failed to actually perform the behavior. The psychologists developing these programs were having the clients say what they were going to do, but because they were psychologists and not occupational therapists, they did not have the clients practice the activity that they were supposedly verbally self-regulating (Cermak, 1976). So, in fact, they were training the clients to say and then not do. I and my psychology colleague, however, were going to have Dave verbally self-regulate a morning hygiene program while actually carrying it out. It took two of us, because neither of us was willing to be alone in the room with Dave. We gave him chocolate Smarties—the U.K. equivalent of M&Ms, but better. This was a powerful incentive for Dave, who, as you recall, was hyperoral and constantly hungry.
Dave was responding to the program, but the director of nursing was complaining that we were using too many bars of soap. We would find what looked like half-eaten bars of soap in the sink. I think Dave was leaving the soap in the sink and running water over it. But it did look like he was eating it, and whatever was happening to the soap, it was a problem for the director of nursing, so it was also a problem for us. I decided that I could address the problem by going into town to buy Dave a bottle of liquid soap. When I got back to the unit, I saw Dave and told him, “Dave, we have been having some problems with using too much soap, so I want you to use this liquid soap instead of the bar soap.” He looked down at me and said, “You big blond bastard, I am never using that soap!”
This is an example of psychological reactance (Brehm & Brehm, 1981), which is the tendency of people who feel that their liberty is being curtailed to increase their efforts to maintain that liberty. Despite not knowing what psychological reactance was at the time, I did recognize that the interaction could have gone better. So I went outside, walked around the building, came back in, waved to Dave, and said “Dave! Dave! I’ve bought you that liquid soap you wanted!” Dave said, “Really, really?” and looked pleased. I said “Great! Quick, let’s have you sign a note about how much you like the liquid soap, and we will post it next to your bathroom sink.”
Figure 3 shows Dave’s personal hygiene program, and Figure 4 is a graph of his improvement. Verbal regulation peaked by Week 10 and then decreased as Dave spontaneously combined three of the cues into the single statement “wash the body, top to bottom.” Dave learned to wash and dress and stopped being malodorous, and we were hoping that his improved personal hygiene would have an effect on people’s attitudes toward him.
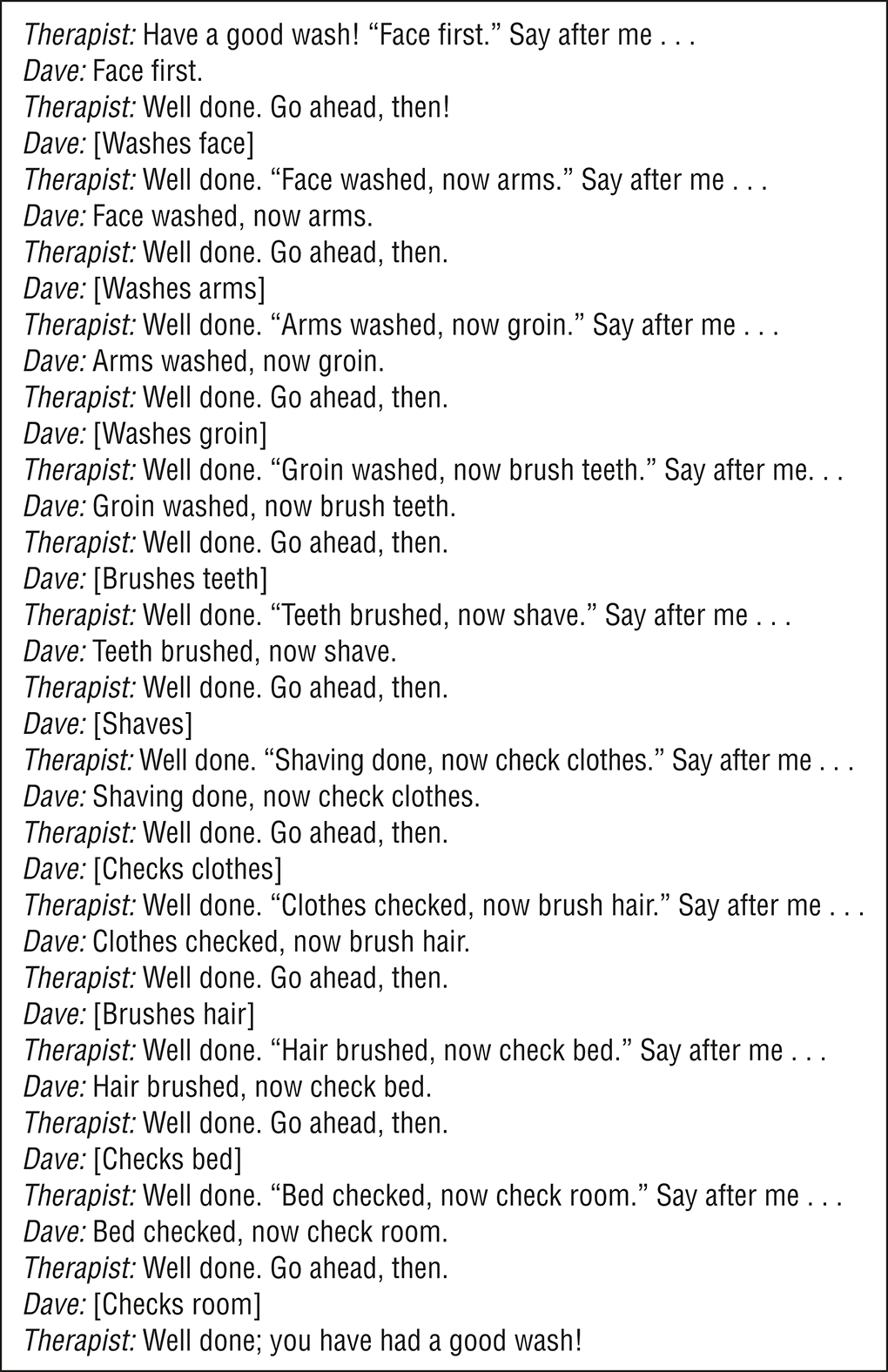
Dave’s washing and dressing program.
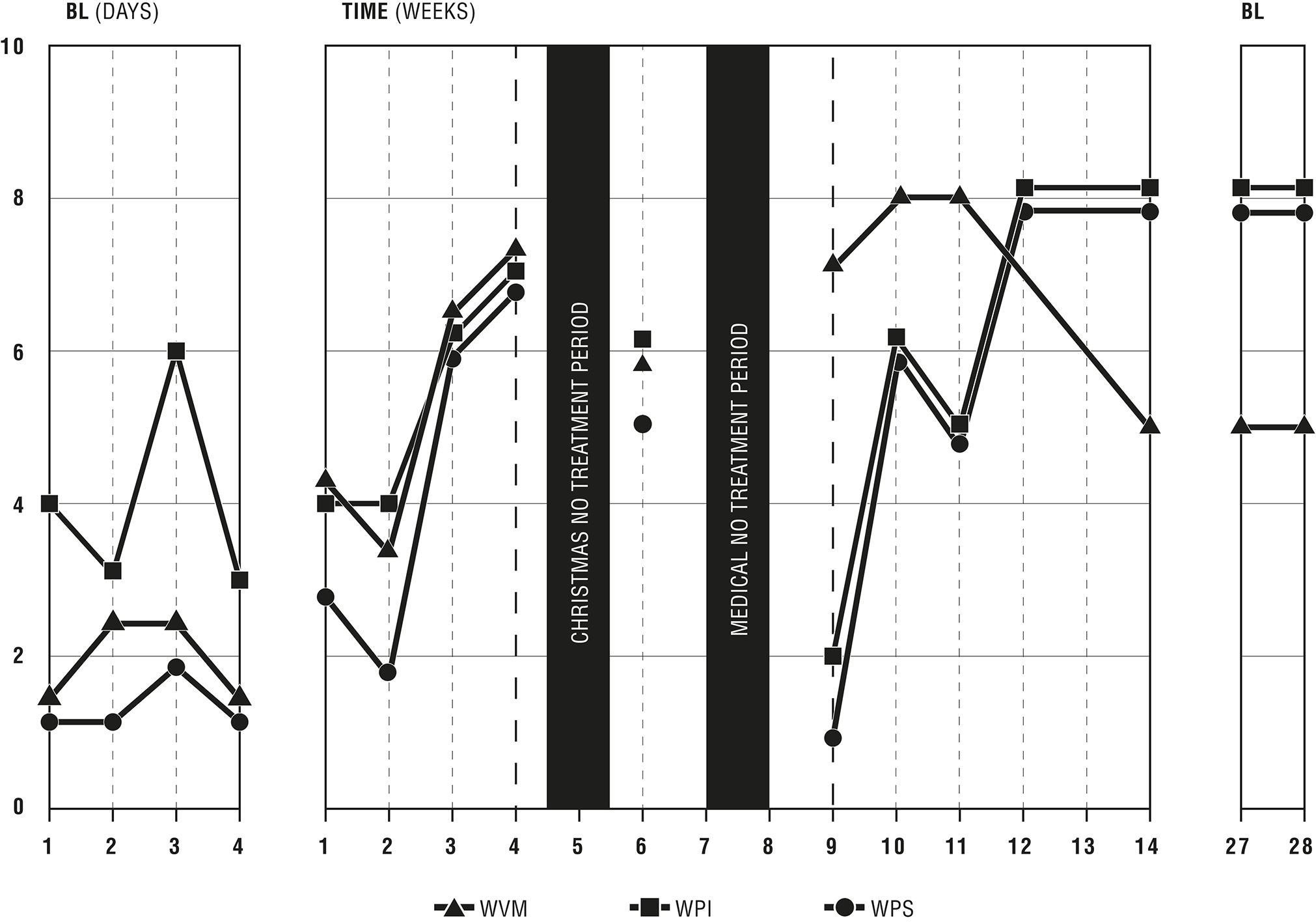
Results of Dave’s washing and dressing retraining program.
Because Dave was hyperoral and constantly hungry and could not tell the difference between food and nonfood objects, he believed that staff were trying to starve him. (We once found him in the laundry room eating laundry powder with a spoon.) In a garage or workshop, he could give you the name and state the purpose of every tool, but he could not name anything in the kitchen. He did not know what a saucepan was, or what boiling meant. Nonetheless, being occupational therapists, we decided that we could address his food-related concerns by teaching him how to cook a meal for himself.
The first step was to perform an individualized task analysis of Dave’s attempts to make beans-on-toast. This was the United Kingdom in the 1980s, which was not known for culinary excellence, and although I am personally vaguely nauseated by the prospect of eating beans-on-toast, Dave loved it. Panel A of Figure 5 shows the results of my attempts to develop a set of written cues that Dave could check off as he performed them and that would reliably result in him making himself beans-on-toast. It took me 10 days to develop written cues that Dave could follow without error in the same way each day.
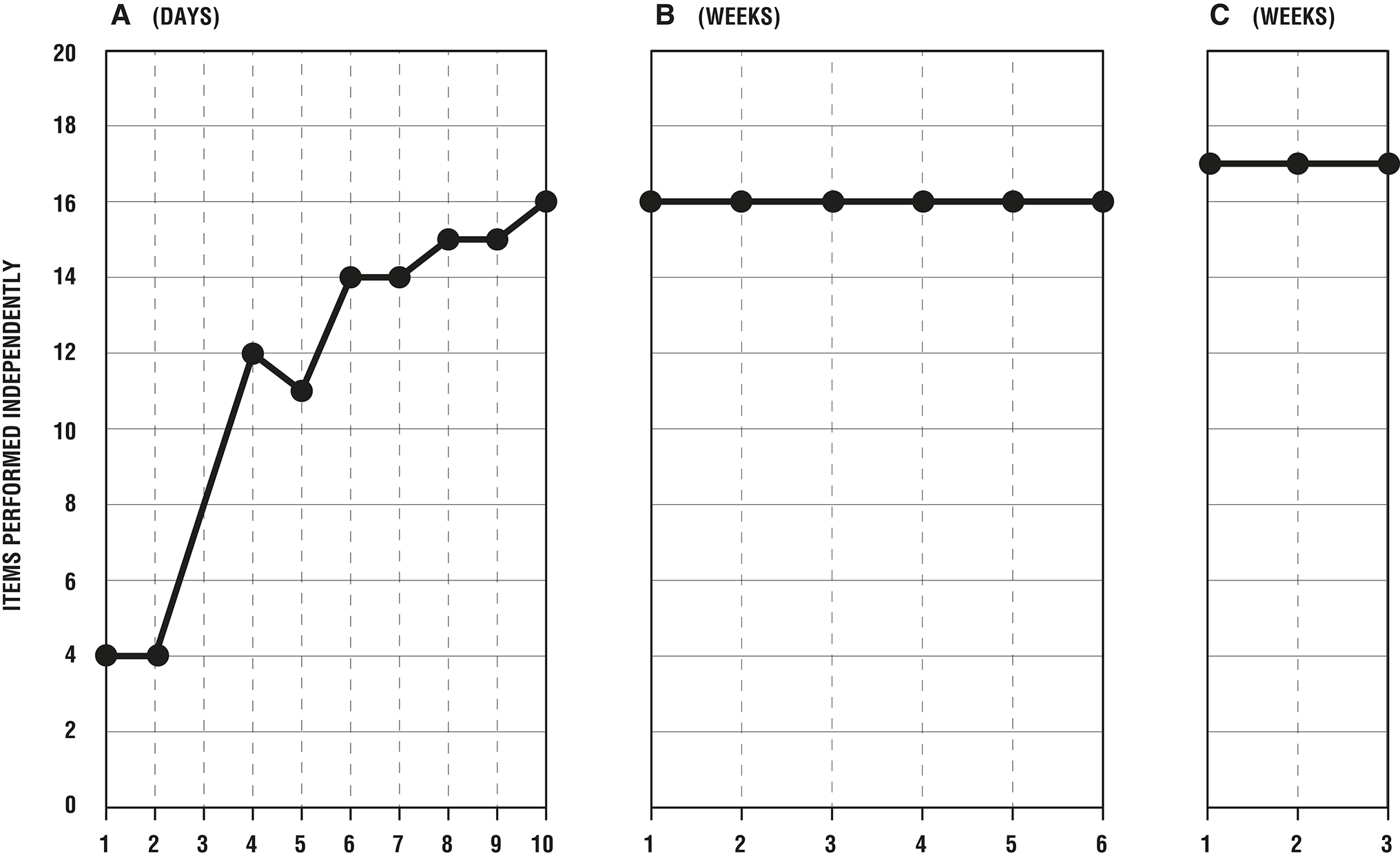
Results of Dave’s meal preparation training program. (A) Food and instruction sheet on counter, with additional verbal prompts when necessary. (B) Food and instruction sheet on counter. (C) Food in cupboard, with no instruction sheet.
From then on, the principal obstacle to Dave’s participation in the training program was getting him into the kitchen. He was very confident that he could not make his own breakfast; in fact, he would state that he could not make his own breakfast loudly as two or three of us were manhandling him into the kitchen and closing the door behind him. The door was a wire-reinforced glass door, so I would gesticulate through the door that he should check the instructions by the side of the tray where I had laid out the bread, the can of baked beans, the can opener, and so on. From my current vantage point, we should certainly have found another way to get Dave into the kitchen; what we actually did was to frog-march him into the kitchen, and I would do this very differently today (see Figure 6).
Definition of frog-march.
Each day, we frog-marched Dave into the kitchen while he vehemently asserted that he was incapable of cooking for himself. And each day, he would eventually happen upon the instructions and make the beans-on-toast. After a while, we were able to remove the instructions and he could still make the beans-on-toast, but we still had to manhandle him into the kitchen each day over his protests.
Dave loved beans-on-toast, but we felt bad about giving him the same thing every day, so we varied the content of the cans, using the same instructions: baked beans, SpaghettiOs, beans with little sausages, and ravioli. These variations went unrecognized by Dave because each day he was unaware that he had ever made breakfast.
One morning, I arrived on the unit and immediately noticed that something was up; people were looking at me strangely, and when I asked what was going on, they pretended that they had not heard me, or they looked away. As I rounded the corner, there was 6-ft-6 Dave smiling and shaking people’s hands. Dave never smiled, ever—it was disconcerting. But “smiling” does not quite capture it—he was trembling, he was vibrating with joy. And as he was smiling and shaking the hand of every person he met, he was saying over and over again, “I can make my own breakfast. I can make my own breakfast!” The daily repetition of the program over time appeared to have done an end run around his impaired episodic memory, allowing him to become consciously aware of the implicit procedural skill he had acquired.
Almost immediately, his attitude toward the staff changed. He was never a warm or particularly engaging person, but he never assaulted us again. In fact, we became so confident in his behavior in the community that we purchased him a bike and would send him out with step-by-step instructions to go downtown to make his own purchases. There was a problem with the frequency with which he lost his bike, so we painted it shocking pink to make it easier for him to find and less likely to get stolen when he forgot to lock it. We tried to set him up in his own apartment but admitted defeat after he tried to dry his plastic lunchbox on the gas stove. Nobody died, but it was an indication that we were aiming for too much independence, and we opted for a board-and-care home.
Lessons From Working With Dave
Early on, when Dave still had his “diary,” it taught me that people remember what they think, not what you tell them. So if you are telling someone that they should do X, Y, and Z and they are thinking that you are a fool, then what they will remember is that you are a fool.
Sometimes the unhelpful things that people tell themselves are inadvertently prompted by others. When you are working with people with a behavior disorder and you admonish them and ask them why they just did that thing that you wish they had not done, you are likely to have made them worse because you have put them in the position of justifying what they did (Miller & Rollnick, 2013). Maybe they were momentarily irritated by someone vocalizing and they hit out. No one says, when asked why they did that thing, “Gosh! I have a severe brain injury and I am impulsive.” But by asking them why they did that thing, you force them justify the behavior (e.g., “He deserved it”). The same principle applies to your private life. Don’t ask your loved ones why they did that obnoxious thing, because they will come up with a reason, and you have made the situation worse by having them tell both you and themselves a story about why their behavior was justified. Instead, ask them to do what it is that you need them to do, or prompt them to think of a better way to handle the situation. But I digress, and I will leave how you choose to interact with your loved ones up to you.
I learned the power of practice and how important it is to prevent errors during practice (Terrace, 1963). Neither Dave’s hygiene program nor his meal preparation program were completely without error, but strenuous efforts were made to minimize errors and rectify them when they occurred as rapidly and unobtrusively as possible (Haslam & Kessels, 2018). Dave’s training programs therefore represent some of the first practical applications of errorless practice principles published in the TBI literature (Giles & Clark-Wilson, 1993; Giles & Morgan, 1989). Later, the robustness of skill–habit learned in this way would become evident; Dave’s caregivers reported that he continued to perform the ADL and IADL routines in the same way 10+ years after he had been taught them.
The central thing I learned from working with Dave was the importance of finding the meaning of an activity for the client. For another person, making beans-on-toast would have been OK at best, but for Dave it was a game changer. He didn’t care about not smelling bad or being independent in bathing. What he cared about was making his own breakfast.
Dave was no longer asking, “How long does it take for a pointless place to admit they can’t help your illness?” but even though he could make his own breakfast, he was no less cognitively impaired than he had been before he could make his own breakfast. So I learned that even limited occupational performance goals can be of central importance to the client and have a major impact on the client’s quality of life and engagement in the therapeutic process.
There is another interesting aspect to this work with Dave. We had deliberately taught Dave two specific skills, personal hygiene and how to make breakfast, but we soon learned that we had accidentally taught him a generic strategy—when you don’t know what to do, look for instructions—because when he became confused in a situation, that is exactly what he did; he looked for instructions. So we started to leave written instructions all over the place so that when he became confused, he would find the instructions and then follow them.
I hope that you will see in the work with Dave two distinct approaches to neurological rehabilitation: specific skill–habit training and (in this instance accidental) strategy training. In specific skill–habit training, the practitioner attempts to teach a specific functional task. The intervention is directed toward a behavior of clinical importance. To be really useful, the skill–habit should become automatic (i.e., used spontaneously and habitually) by the end of treatment. The strategy training approach asks the client to deliberately use thinking strategies to enable performance of behaviors that he or she previously had performed spontaneously without the use of these thinking routines. Both skill–habit training and strategy training are based on the premise that the processes that previously supported occupational performance are degraded to the degree that they can no longer support occupational performance and that these processes cannot be restored through rehabilitation (Clark-Wilson et al., 2014). Rehabilitation therefore focuses on teaching specific functional skills or compensatory strategies to manage problems in living. The interventions are quite different, and I will argue that the types and severity of problems the two different approaches are best targeted toward are also quite different.
A Constraints Model and Three Useful Constructs
Constraints Model
In thinking about what to do in rehabilitation, I use a constraints model. I apply clinical reasoning questions such as “What occupations are central for the client?” “What are the constraints imposed on the client by the neurological insult or injury?” and “How do we get around those constraints so the client can engage in those occupations that make his or her life meaningful?” Cognitive deficits are considered not as targets of intervention but as obstacles to circumvent to improve performance skills. Domain-specific cognitive assessments are used to explicate performance breakdowns so that interventions can be developed that enhance occupational performance (Bar-Haim Erez & Katz, 2018).
Cognition is not an intervening variable between brain and occupational performance. Just because a construct is useful—and helps us understand the ways in which a client’s performance breaks down—does not mean that it accurately represents an “underlying process” or that such a process is remediable through challenge and repetitive exercise (Clark-Wilson et al., 2014; Giles, 2018). It would be great if practicing cognitive functions—by, for example, engaging the client in paper-and-pencil activities or gamelike computer programs—improved cognition and thereby had an effect on occupational performance. However, the majority of studies offer little realistic evidence that these activities have any impact on occupational performance. When a client practices a functional activity that is believed to be related to a cognitive process, it is the functional activity, and not the hypothesized underlying cognitive process, that improves (das Nair & Lincoln, 2007; Robertson & Murre, 1999; Rohling et al., 2009; Wilson et al., 2009; Zickefoose et al., 2013). But cognitive constructs are useful in understanding how occupational performance breaks down.
Controlled and Automatic Processes
The first cognitive construct I want to talk about comes from the seminal work of Schneider and Shiffrin in the 1970s (Birnboim, 2003; Schneider & Shiffrin, 1977; Shiffrin & Schneider, 1977). Schneider and Shiffrin talked about the distinction between controlled and automatic processes. Controlled processes are effortful and capacity limited. Automatic processes can be carried out without conscious awareness and can be very complex. Automatic processes require practice in stable contexts and are developed by doing: They are based on experience. As we all know if we think about it, the key to skill development is practice.
Memory
The second cognitive construct that is important is memory (Tulving, 1983). As end users of memory, we tend to think of memory as a single function (Hasselmo, 2013). But we know that there are multiple memory systems and that actual remembering is likely supported by many memory systems that overlap and work together seamlessly and without our awareness.
A major distinction in the memory literature that I find very useful is the distinction between declarative and nondeclarative memory. Declarative means that you can declare it: You know that you know it. It is available to introspection. Declarative memory is usefully divided into 2 subcategories: episodic and semantic memory. Episodic memory is memory for individual discrete events with the sensory and temporal associations still attached. Semantic memory is knowledge of facts about oneself, the world, historical dates, and so forth (e.g., Dave had impaired semantic memory for biological entities).
The other major memory category, nondeclarative memory, is often conceived of as an array of learning systems that include priming, some types of stimulus–response learning, classical conditioning, implicit procedural learning, and so forth. The central characteristic of implicit procedural learning is the ability to express acquired information through performance and in the absence of consciously recalling anything (Eichenbaum & Cohen, 2001; Reber, 2013). Implicit procedural learning is an emergent property of the combination of experience and the general plasticity of the brain (Reber, 2013). Only activities that are practiced in the same way and in the same context are retained in implicit procedural memory. The more practiced they are, the more available they are to the person, and the more likely they are to be repeated when cued in the appropriate circumstances.
Initiation
The third cognitive construct I want to discuss is initiation—the capacity to independently start a behavior to meet a personal goal. I was working in Texas with 30 people with very severe TBI. We had spent a few therapy sessions talking about how to do laundry. But on this particular day, we were going out to the local laundromat. Everyone had their dirty laundry in trash bags, and they successfully got their laundry into the washing machines and got the machines running. Then it was time for a soda and a smoke. I sat for close to 30 min as the washing machines clunked to the end of their cycle and people smoked their cigarettes or drank their soda, but no one transferred their clothes from the washer to the dryer. I asked if there was anything that people should be doing—blank stares. But it was also not lack of knowledge or of cooperation, because as soon as I said, “OK; do what you need to do next to finish doing your laundry,” everybody put their clothes in a dryer. This was a problem in initiating an action based on mental checking of a known action sequence.
James T. Reason (1984, 1990), a psychology professor at Manchester University in the United Kingdom who studies human error and action control, called the process of checking the progress of a known action sequence to determine whether action is needed act–wait cycles. Chevignard et al. (2000) called the development of a plan of action script generation and the carrying out of the plan script execution. For example, if we have an appointment across town, we mentally plan out the steps that are necessary to get to the appointment on time and then work backward to create a mental timeline (script generation). Periodically we compare plan time to real time to know whether we should act or wait (script execution). The realization that many of the clients with whom we work do not create an action plan in imagination prior to performance has been central to my understanding of the real-world problems of clients with severe impairments (Allain et al., 2012; Giles & Clark-Wilson, 1993).
Skill–Habit Training
A skill–habit training program can help people make needed functional behaviors automatic. Automaticity reduces the situational cues needed to elicit behaviors and reduces the need for in-the-moment decision making (see Figure 7). Automaticity also reduces dependency on impaired memory systems and makes impaired initiation skills less problematic. Almost 25 years ago, my colleague Jo Clark-Wilson and I built on concepts from social psychology and learning theory and on implicit procedural skill development and errorless learning to develop the skill–habit training approach we call the neurofunctional approach (Clark-Wilson et al., 2014; Giles & Clark-Wilson, 1993).
Elements of a retraining program.
In the neurofunctional approach, the occupational therapist first has to establish goals with the client. How goal setting is conducted after TBI depends on the client’s place in the arc of recovery. In the acute care setting, it is about interviewing the family and developing verbal interactions that can engage the client. In postacute care settings, the therapist needs to conceptualize how the client understands his or her situation and to find a way to work with the client that the client finds acceptable (Clark-Wilson et al., 2014; Giles, 2018; Giles & Clark-Wilson, 1993).
Next, the occupational therapist observes how the client attempts to perform the behavior. During observation, cues to initiate the occupational performance within a specific domain should be as minimal as possible (e.g., “Show me how you would normally get up and dressed [or “Show me show you would normally cross the street]”). The therapist then performs an individualized task analysis to identify the subroutines that the client can do well and the key action points where performance breaks down. This individualized task analysis is used to generate a retraining program composed of a series of cues that, if followed, will result in accomplishing the ADL or simple IADL task that is targeted (Clark-Wilson et al., 2014; Giles, 2018). The cues must reliably elicit a stable, functionally equivalent behavioral response from the client (cue experimentation is used to establish cues that reliably elicit the desired behavior).
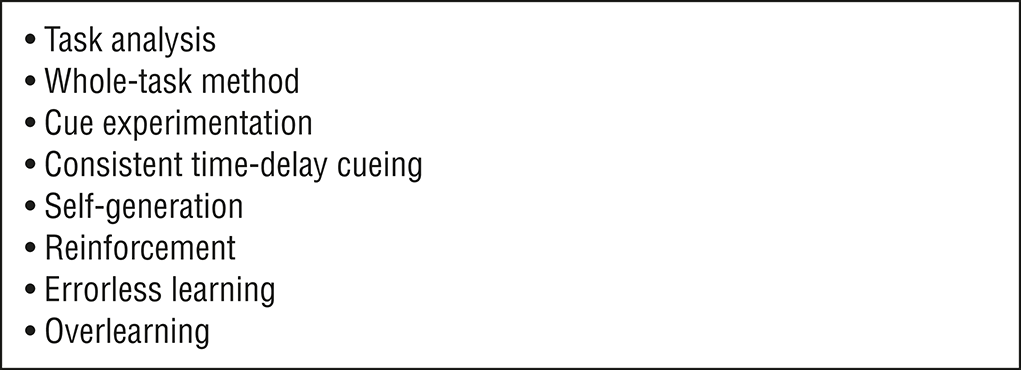
Once the cueing system is complete, the client must practice it. Physical assistance may be required initially, but the goal is to develop a physical routine that the client can accomplish independently. Cueing is provided so as to prevent errors (i.e., errorless practice). Learning in this way is experiential: Errors must be avoided so that the client does not learn the errors (Haslam & Kessels, 2018). As learning takes place, the series of cues initially needed for behaviors (e.g., “Wash your face: pick up the washcloth, put soap on the washcloth, rub your face with the washcloth, then your right ear, then your left ear,” and so forth) can be consolidated (e.g., “Wash your face”). A program that began with 50 cues might be progressively consolidated, becoming shorter as the complexity of the behavior that the client can produce to a single cue increases until the entire behavior becomes automatic (Giles, 2018). Figure 8 lists some techniques that we use in retraining ADLs and simple IADLs.
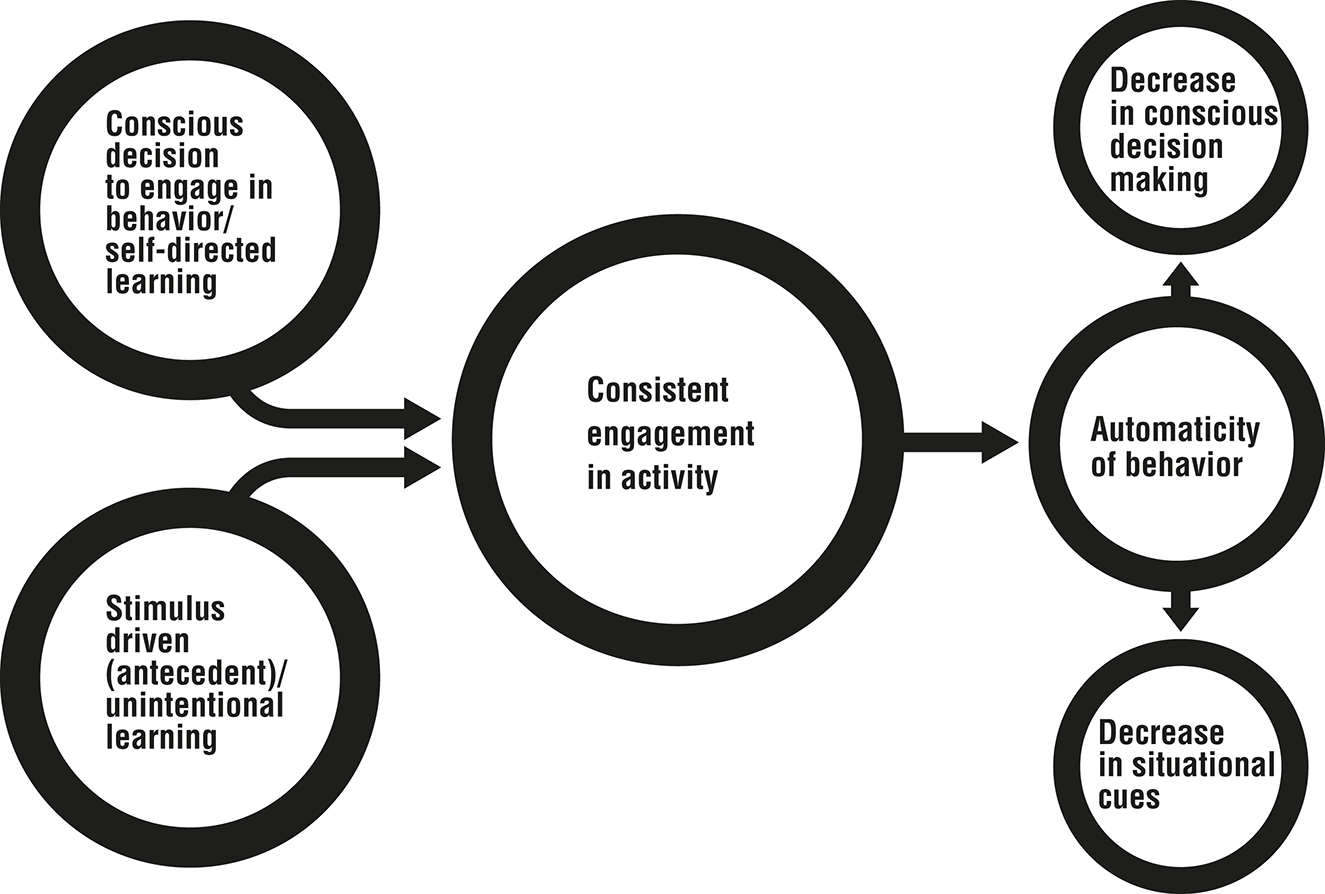
Schematic representation of two routes to the development of automaticity and the consequences of the development of automaticity. Repetitive enactment of a response to a stimulus results in the development of automaticity, which results in a reduction in the salience of cues needed to elicit the behavior and a consequent reduction in the need for online conscious decision making.
This rehabilitation method has limitations. The client can be taught to master only routine activities (ADLs and simple IADLs), and this approach does not equip the client to manage true novelty. Nonetheless, the neurofunctional approach has been validated in several randomized controlled trials (RCTs) in both acute rehabilitation and postacute settings (Rotenberg-Shpigelman et al., 2012; Vanderploeg et al., 2006, 2008).
As many of you know, posttraumatic amnesia is a period of memory impairment and delirium that follows moderate to severe TBI. I am excited to tell you that the neurofunctional approach has recently been shown in a major RCT by a group of researchers in Australia to be superior to usual care during PTA and to accelerate the slope of recovery after TBI (Trevena-Peters et al., 2018). Its application did not increase agitation, and nonsignificant but consistent findings suggest that use of the approach actually decreased agitation during PTA (Trevena-Peters et al., 2017). The neurofunctional approach is now the only occupational therapy approach to have been shown in an RCT to be effective during PTA, and it is pretty much the only evidence-based intervention shown to accelerate improvement during PTA. So if the approach is validated in subsequent trials, occupational therapy practitioners will have the only approach demonstrated to be superior to standard care during the period of PTA after TBI (Trevena-Peters et al., 2017, 2018).
Strategy Training
The other major class of intervention for people with acquired neurological impairments is strategy training. Strategy training relies on the client’s adopting new thinking routines that support his or her occupational performance. Joan Toglia’s Dynamic Interactional Model, and the multicontext approach in particular, has been central to advancing the ways we address the occupational performance difficulties of people with mild to moderate impairments after neurological insults (Toglia, 1989, 2018). Much of the focus in occupational therapy has been on the use of global metacognitive strategy learning in which the client is taught to use higher order compensatory strategies—for instance, internal scripts—intended to facilitate problem solving in areas that the client finds problematic.
The Cognitive Orientation to daily Occupational Performance (CO–OP) approach is an example of a global compensatory strategy approach (Dawson et al., 2017; Polatajko & Mandich, 2005). CO–OP was developed for and has been validated with children with developmental coordination disorder, but it has also been used to teach adults with executive dysfunction how to overcome occupational performance deficits (Dawson et al., 2017; Thornton et al., 2016). CO–OP teaches a global strategy derived from the work of Meichenbaum (1977)—goal, plan, do, check—and uses this global strategy in a process of guided discovery to help clients develop strategies to solve specific self-identified performance problems. The client identifies the performance problem (goal) and then identifies and evaluates potential strategies to solve the problem (plan). The client then implements that strategy (do) and checks to see whether it worked (check). CO–OP has been applied with people with stroke and TBI, and positive outcomes have been reported (Dawson et al., 2017).
My colleague M. Tracy Morrison, a professor at the Universities of Minnesota and Missouri, has been using assessments of metacognition and executive functioning and developing interventions to support clients’ ability to learn ways to reduce everyday performance limitations (Morrison et al., 2013, 2015). Morrison began this work using the Multiple Errands Test with clients with mild impairments from frontal lobe lesions (Morrison et al., 2013, 2015). Later, she recognized that use of a specific debriefing interview could assist clients in recognizing how they came to make poor decisions and in generating their own compensatory strategies. Part of this therapeutic process is to help clients cope with the distress associated with recognizing their errors. In the treatment of adolescent and adult clients with high-functioning autism, Morrison has adopted “fail forward” as a mantra for learning from mistakes and using them to improve performance.
Assessing Functional Cognition
The last major concept I want to address is functional cognition, a term first associated in occupational therapy with Claudia Allen’s (1985) Cognitive Disabilities model. Functional cognition is defined as the ability to use and integrate thinking and performance skills to accomplish essential ADLs and IADLs (Bar-Haim Erez & Katz, 2018; Giles et al., 2017; Wesson et al., 2016). Unlike what psychologists or speech–language therapists think of as cognition, functional cognition integrates all of the client’s personal resources, such as the ability to understand his or her own strengths and weaknesses (metacognition) and the ability to employ strategies in the service of occupational performance. In terms of performance skills, functional cognition involves habits, routines, and skills that support occupational performance (e.g., organizational habits; Giles et al., 2017).
Rather than relying solely on self-report or the report of family members, occupational therapy practitioners can assess functional cognition using performance-based testing. We can ask clients to engage in complex pseudofunctional tasks that allow for the use of strategies and that mimic actual functional tasks (Morrison et al., 2015). In general, these tasks have more than one route to satisfactory performance, have greater cognitive than physical emphasis, require the integration of multiple sources of information, and require the sequencing of multiple action steps for goal completion (Giles et al., 2017).
Occupational therapy practitioners have a tradition of observing how clients make macaroni and cheese or brownies in the occupational therapy kitchen or how they perform other personally relevant complex tasks so as to infer their ability to perform other complex tasks. Having clients engage in these activities is compelling both for us and for the clients. But brief observations and inferences based on these observations unsupported by standardized measures are not enough. Occupational therapy practitioners cannot tell the difference between the types of errors made by people with and without mild cognitive impairment through observation alone (Bottari & Dawson, 2011). Reporting our concerns on the basis of our client having trouble in the occupational therapy kitchen is one thing, but we need to be articulating our distinct approach to assessment to the multidisciplinary health care community in a way that the wider community can understand and endorse.
Baum and Edwards’s pioneering work on the Executive Function Performance Test (Baum et al., 2003) and Toglia’s (2015) Weekly Calendar Planning Activity are standouts in enabling us to analyze the level of support needed for task achievement. But until recently, other than a very few examples, occupational therapists have not been creating standardized performance-based measures sensitive to mild impairments that have sufficient rigor to stand up to scrutiny from outside the profession, and as a profession we have not been systematically adopting these measures in our professional practice. We need to develop and adopt psychometrically sound performance-based measures of functional cognition. Evidence is accumulating that performance-based assessment of functional cognition is more indicative of actual IADL and community independence than more traditional cognitive testing approaches or self- or proxy-report measures.
The wider health care community is beginning to embrace the occupational therapy concept of functional cognition, but this recognition is a double-edged sword. We have great things to offer, but we are behind some other professional disciplines in systematizing our assessment approaches and implementing them across practice settings. Our distinct disciplinary focus is needed to improve client care and outcomes. If we fail to meet this need, another discipline will.
To place this need in context, as many as 20% of all people discharged from acute hospitalization are readmitted within 30 days (Herrin et al., 2015), and unmanaged cognitive deficits are often implicated in these readmissions (Barnett et al., 2015). As part of the American Occupational Therapy Association’s (AOTA’s) response to the Improving Medicare Post-Acute Care Transformation (IMPACT Act) of 2014 (Pub. L. 113–185), two independent groups of researchers—Edwards, Baum, Morrison, Wolf, and I (Giles et al., 2017) and Rogers, Chisholm, Holm, and Skidmore (Rodakowski et al., 2014; Skidmore, 2017)—have been developing performance-based measures of functional cognition that we hope can identify people who have mild cognitive deficits that are significant enough to lead to hospital recidivism. We have been suggesting to the Centers for Medicare and Medicaid Services that this type of measure could be used to identify people who need occupational therapy or enhanced community support services to maintain independence (Giles et al., 2017). Our arguments are strengthened by the fact that occupational therapy is the only discipline for which increased spending has been shown to reduce the rate of hospital readmission (Rogers et al., 2016).
The adoption of performance-based measures of functional cognition has the potential both to help us identify new populations of people who need occupational therapy and to direct us to the types of interventions most likely to be useful for people across diagnoses. People who can recognize and remember their errors and then alter their responses can probably make use of strategy training, whereas those who have major impairments in functional cognition (e.g., impaired memory or self-awareness) are probably best assisted using a skill–habit training approach.
Occupational therapy practitioners have opportunities at both ends of the spectrum of severity of client impairment. We can identify and support people with mild impairments by using performance-based assessments of functional cognition and by offering them strategies to solve novel problems. For severely impaired clients, we need to develop routines clients can use to achieve their goals, and then we need to help them practice these routines until they become automatic.
This effort requires that we adopt some new practices and move out of our comfort zones. For clients on the mild end of the spectrum, we need to not overfocus on the definitions of cognitive impairment from other disciplines and to not defer to better-known psychological approaches to assessment and treatment, but rather to truly focus on occupation. We need to stop assuming that a client is unimpaired because he or she is independent in ADLs or because we “just know” if someone has cognitive impairment—the evidence is unequivocal that we don’t just know and that we need to test (Edwards et al., 2006). For clients on the severe end of the spectrum, we need to finally and unequivocally reject the notion that if they cannot remember our treatment sessions, then they cannot respond to therapy (Clark-Wilson et al., 2014; Trevena-Peters et al., 2018). Finally, we have to recognize that for clients with the most severe impairments, independence is overrated. Appropriate goals for some clients may be to increase quality of life through creating islands of independence while they continue to receive support in other areas (Clark-Wilson et al., 2014).
Helping Clients Find Their Own Way Forward
I would like to end as I began—on a personal note. Most of my ideas about clinical practice have been driven by my own tendency toward concreteness. I have turned my cognitive limitations to my advantage, and maybe that is why I understood client responses that some of my colleagues at Kemsley did not understand. Damage to some of our more sophisticated cognitive mechanisms reveals the foundational nature of our behaviors: Brain damage helps show us who we are. Brain damage does not make a person alien or other; it just reveals the underlying mechanisms that are part of being human.
I have come to the understanding that people (ourselves and our clients) are mostly doing the best that they can, and if they are not doing the best that they can, then they are doing what makes sense to them. In addition to being an occupational therapist, I have a PhD in clinical psychology, and as part of that training I was taught the Rorschach inkblot test. When you administer the Rorschach, you show an inkblot and say, “What might this be?” Invariably, people say, “It’s an inkblot,” and you say, “Yes, this is the inkblot test; what else might it be?” In my current life I do not give the Rorschach, but two additional phrases from Rorschach administration are constantly in my head. When a person tells you what the inkblot might be, you say, “Help me see it like you do” and “I want to see it like you do.” I think wanting to see the client’s situation as the client does, from the client’s own point of view, is central to finding an intervention that can help the client see a viable way forward.
In some ways, you can see my 35 years of clinical practice as an occupational therapist as a reaction to my parents’ paranoia. Just like my parents, there will always be those who will try to tell you that there is them and us, but there is only us. No matter how uncomfortable Dave’s behavior made us, he was not bad. He was distressed, resentful, and angry—very human reactions to trauma and loss. When stressed by our clients’ behaviors, it is important to combat our own exercise of the FAE and to notice how quickly we can judge others negatively. Once we have labeled our clients as uncooperative, unmotivated, or just plain bad, we have given up on our ability to be effective. My colleagues and I who work at Crestwood Neurobehavioral Treatment Center in Fremont, California, call our approach to behavior disorders “relational,” and a key component of this approach is “relentless kindness” (Giles et al., 2013, 2014; Kalapatapu & Giles, 2017).
There will always be advances in science and in our understanding of brain function, and they are important, but as occupational therapy practitioners we recognize that it is the simple things—the commonplace activities that have meaning for the individual—that really matter (Baum, 1980; Peloquin, 1995). Engaging the client in meaningful activity is the art and science of occupational therapy, and it will never be superseded by technological innovation because true creativity and genuine empathy cannot be mechanized.
We occupational therapy practitioners are privileged to work in a profession in which we can help others find their own way forward, and we can have fun doing it, an important value in itself. So with the understanding that those who follow us—today’s and tomorrow’s students—will further advance the practice of occupational therapy, we can be confident in the future of the profession we love. We have the potential to truly contribute to the well-being of those around us, and really, what could be better than that?
Footnotes
Acknowledgments
I thank my friends and colleagues Jo Clark-Wilson and Karen Scott; my supporters from Samuel Merritt University (SMU); students, past and present; my chairperson, Kate Hayner; Ginny Gibson and the SMU faculty who have supported me as I worked on what I wanted to say; and Donna Breger-Stanton, who nominated me for the Eleanor Clarke Slagle lectureship. Thanks also go to Amy Lamb, president of AOTA, and the chairperson and members of the AOTA Volunteer Leadership and Development Committee.
1
This article is an adaptation of the Eleanor Clarke Slagle Lecture presented at the 2018 AOTA Annual Conference & Expo, Salt Lake City, UT.