
Abstract
Impaired arm function after stroke limits engagement in daily life and warrants active rehabilitation (Hatem et al., 2016). Robot-assisted therapy (RT) may elicit better performance of the affected arm in activities of daily living, arm function, and arm muscle strength (Mehrholz et al., 2015) in patients with stroke, but evidence for the benefits of RT compared with intensity-matched control treatment (CT) is inconsistent. Lo et al. (2010) found no significant difference between RT and intensity-matched CT in improvement in Fugl-Meyer Assessment (FMA; Fugl-Meyer et al., 1975) scores, but Hsieh et al. (2011) showed that patients who received RT achieved a 3-point higher mean difference on the FMA than those who received intensity-matched CT.
RT has involved a variety of robotic devices and treatment protocols, which may be one of the causes of inconsistent results among studies. For example, two of the most-studied devices, the InMotion (IMT) 3.0 robot (Interactive Motion Technologies, Watertown, MA; Krebs et al., 2007) and the Bi-Manu-Track (BMT) robot (Reha-Stim, Berlin, Germany; Hesse et al., 2003), involve different protocols. The IMT focuses on training of the paretic arm, whereas the BMT emphasizes bilateral arm training. Unilateral and bilateral RT could result in differential improvements in stroke patients. Previous studies have shown that the bilateral BMT may be favorable for decreasing motor impairments in the proximal arm, whereas the unilateral BMT may be optimal to improve the efficiency of affected arm function (Wu et al., 2013; Yang et al., 2012). Although initial studies compared the effects of unilateral and bilateral BMT, evidence of the relative effectiveness of different types of robotic therapy is limited (Marchal-Crespo & Reinkensmeyer, 2009).
A better understanding of the relative advantages of the robotic devices through head-to-head comparisons is critical for delivering effective and customized rehabilitation (Iosa et al., 2013). In this preliminary study, we compared the effects of two robot-assisted devices (IMT vs. BMT) and of the RTs and intensity-matched CT on motor function of the affected arm and self-reported arm use in daily living in patients with chronic stroke. We hypothesized that RT based on the IMT and BMT devices would produce different benefits for motor function and daily use of the affected arm in patients with stroke and that they would be more effective than a CT in improving motor function.
Method
We used a single-blind randomized controlled design to compare the effects of two RT regimens. Eligible outpatient participants were randomized into the IMT, BMT, or CT group using a computerized random number table. Four certified occupational therapists were trained in the intervention protocols and principles before administering the treatments. The assessors were three occupational therapists blinded to participants’ group. Outcome measures were administered before and immediately after the intervention by the same assessor for each participant. The outcome measures were identified before analyses.
Participants
Occupational therapists screened and recruited 30 community-dwelling patients between August 2014 and July 2015 from the occupational therapy departments at two hospitals in Taiwan. The institutional review boards of the participating hospitals approved the study. Participants were blind to the study hypotheses. During the intervention period, participants stopped their original occupational therapy sessions, but other routine rehabilitation programs (e.g., physical therapy) were conducted as usual.
The inclusion criteria were ≥6 mo after the first-ever unilateral stroke; an initial score of 10–45 on the FMA Upper Extremity (FMA–UE) subscale (Fugl-Meyer et al., 1975; Gladstone et al., 2002); no excessive spasticity in any joints of the affected upper limb (Modified Ashworth Scale [MAS] score ≤3; Bohannon & Smith, 1987); ability to follow study instructions (Mini-Mental State Examination score ≥24; Folstein et al., 1975; Skidmore et al., 2010); no other neurological, neuromuscular, or orthopedic disease; and willingness to sign the informed consent. The exclusion criteria were stroke lesion in the cerebellum or brainstem, comorbidity with other severe neurological or neuropsychological impairment (e.g., epilepsy, global aphasia, severe attention deficits), and poor physical condition that might limit ability to complete the intervention.
Intervention Protocols
All participants in the three groups received interventions of 90–100 min/day, 5 days/wk for 4 wk. The intervention began with 5 min of muscle tone normalization as needed. The BMT and IMT groups received 70–75 min of RT. After the RT, functional-based activities were practiced for 20 min. These groups were matched in duration and frequency of intervention but not in movement repetition as a result of the different characteristics of the protocols (e.g., bilateral vs. unilateral, resistance vs. assistance).
The BMT robot (Hesse et al., 2003) offers bilateral symmetrical practice of two movement patterns: (1) forearm pronation–supination and (2) wrist flexion–extension, in three modes (Mode 1: passive–passive; Mode 2: active–passive, with the unaffected arm driving the affected arm; Mode 3: active–active, with resistance). The treatment protocol included both movement patterns for 600–800 repetitions each in Modes 1 and 2 and 150–200 repetitions in Mode 3. The therapist set and adjusted the amount of resistance in Mode 3 according to the participant’s ability (Hsieh et al., 2011).
The IMT robot (Krebs et al., 2007) provides two types of unilateral movement patterns: (1) forearm pronation–supination and (2) wrist circumduction. Three tasks provided by the IMT were used in this study: (1) the passive-stretch task, (2) the one-way-record task (affected arm going actively), and (3) the adaptive task (assisted when needed). The treatment protocol included 120–160 repetitions of passive-stretch tasks, 12–48 repetitions of one-way-record tasks, and 320–480 repetitions of adaptive tasks that provided adaptive robot assistance for each movement pattern. Additional information about the robot devices is provided in the supplemental materials (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”).
Functional-based activities involved tasks of two types. One type simulated the robot-assisted movements (i.e., forearm and wrist movements), such as pouring water, turning a doorknob, and opening a jar, and the other involved tasks different from the robot-assisted motions, such as dressing, sweeping the floor, and wiping a table.
The CT group received individualized occupational therapy mediated by a therapist. The training programs were modified according to each patient’s needs and level of impairment. The CT programs generally consisted of muscle tone normalization, fine motor training, gross motor training, muscle strengthening, and functional activity practice.
Outcome Measures
The primary outcome measures were the FM–UE and the MAS. The FMA–UE has 33 items assessing reflexes, movements, coordination, and speed (Fugl-Meyer et al., 1975; Gladstone et al., 2002). Each item is scored from 0 to 2, and a higher score indicates better motor function. We assessed the overall (66), proximal (0–42), and distal (0–24) scores on the FMA–UE to compare different UE elements (Yang et al., 2012). The MAS grades spasticity from 0 (no increase in muscle tone) to 5 (affected part is rigid in flexion and extension; Bohannon & Smith, 1987). We calculated the mean scores of the overall, proximal (shoulder and elbow), and distal (forearm, wrist, and finger) portions of UE muscle tone.
Secondary outcomes were the Motor Activity Log (MAL) and the Medical Research Council (MRC) scale. The MAL is a self-report instrument that uses a semistructured interview to measure the amount of use (AOU) and the quality of movement (QOM) of the affected arm in 30 activities of daily living (van der Lee et al., 2004). Each activity is scored from 0 to 5, with a higher score indicating more frequent use of the affected arm (MAL–AOU) or higher quality of movement (MAL–QOM). The MRC (Medical Research Council of the United Kingdom, 1976) measures the muscle strength of the proximal (shoulder flexors, shoulder abductors, elbow flexors, and elbow extensors) and distal (wrist and finger flexors and extensors) parts of the affected arm. The MRC score for each muscle ranges from 0 (no muscle contraction) to 5 (normal strength).
Statistical Analysis
We used Fisher’s exact test for categorical data and the Kruskal–Wallis rank-sum test for continuous variables to compare the baseline differences among the three groups. The pretest and posttest differences within each group were analyzed using the Wilcoxon signed-rank test. Treatment efficacy was calculated by computing the change scores from pretest to posttest. Treatment efficacy among groups was compared using the Kruskal–Wallis rank-sum test with the change scores between pretest and posttest. The Mann–Whitney U test was used for post hoc comparisons. The effect size (r) for the post hoc comparison was calculated with the following formulas for each variable to illustrate the magnitude of group difference:

with an r of at least .50 for a large effect, .30 for a moderate effect, and .10 for a small effect (Cohen, 2013; Fritz et al., 2012). Statistical analyses were performed with IBM SPSS Statistics (Version 19.0; IBM Corp., Armonk, NY). The level of statistical significance (α) was set at .05.
Results
Thirty participants completed the clinical evaluation and intervention. Baseline characteristics did not differ significantly among the three groups (Table 1).
Participant Baseline Characteristics
Note. BMT = Bi-Manu-Track robot-assisted therapy; CT = control treatment; FMA–UE = Upper Extremity subscale of the Fugl-Meyer Assessment; IMT = InMotion 3.0 robot-assisted therapy; MMSE = Mini-Mental State Examination.
Categorical variables are shown as the number of participants and were analyzed with the two-tailed Fisher exact test. Continuous variables are shown as the median (Quartile 1–Quartile 3) and were analyzed with the two-tailed Kruskal–Wallis rank-sum test.
For the primary outcomes (Table 2 and Figure 1), the mean change scores of the overall FMA–UE were 8.0 points in the IMT group, 5.5 points in the BMT group, and 2.5 points in the CT group. The pretest to posttest changes in the scores of the three groups were significant on the overall, proximal, and distal FMA–UE. The differences among the three groups were significant on the overall and proximal FMA–UE scores. In the post hoc analysis of the FMA–UE scores, the increase was nonsignificant but with a moderate to large effect size in favor of the IMT group over the BMT group (overall r = .52, p = .06; proximal r = .47, p = .08) and was significantly better in the IMT group than in the CT group (overall r = .85, p < .01; proximal r = .84, p < .01). The difference between the BMT and CT groups was nonsignificant (overall r = .45, p = .08; proximal r = .17, p = .30).
Descriptive and Inferential Statistics for the Outcome Measures
Note. AOU = amount of use; BMT = Bi-Manu-Track robot-assisted therapy; CT = control treatment; FMA–UE = Upper Extremity subscale of the Fugl-Meyer Assessment; IMT = InMotion 3.0 robot-assisted therapy; K–W test = Kruskal–Wallis rank-sum test; MAL = Motor Activity Log; MAS = Modified Ashworth Scale; MRC = Medical Research Council scale; Q1 = first quartile; Q3 = third quartile; QOM = quality of movement.
p value of two-tailed Wilcoxon signed-rank test for within-group differences.
The Kruskal–Wallis (K–W) test used for comparison of treatment efficacy among the three groups.
Lower MAS scores indicate better function.
Statistically significant (p < .05).
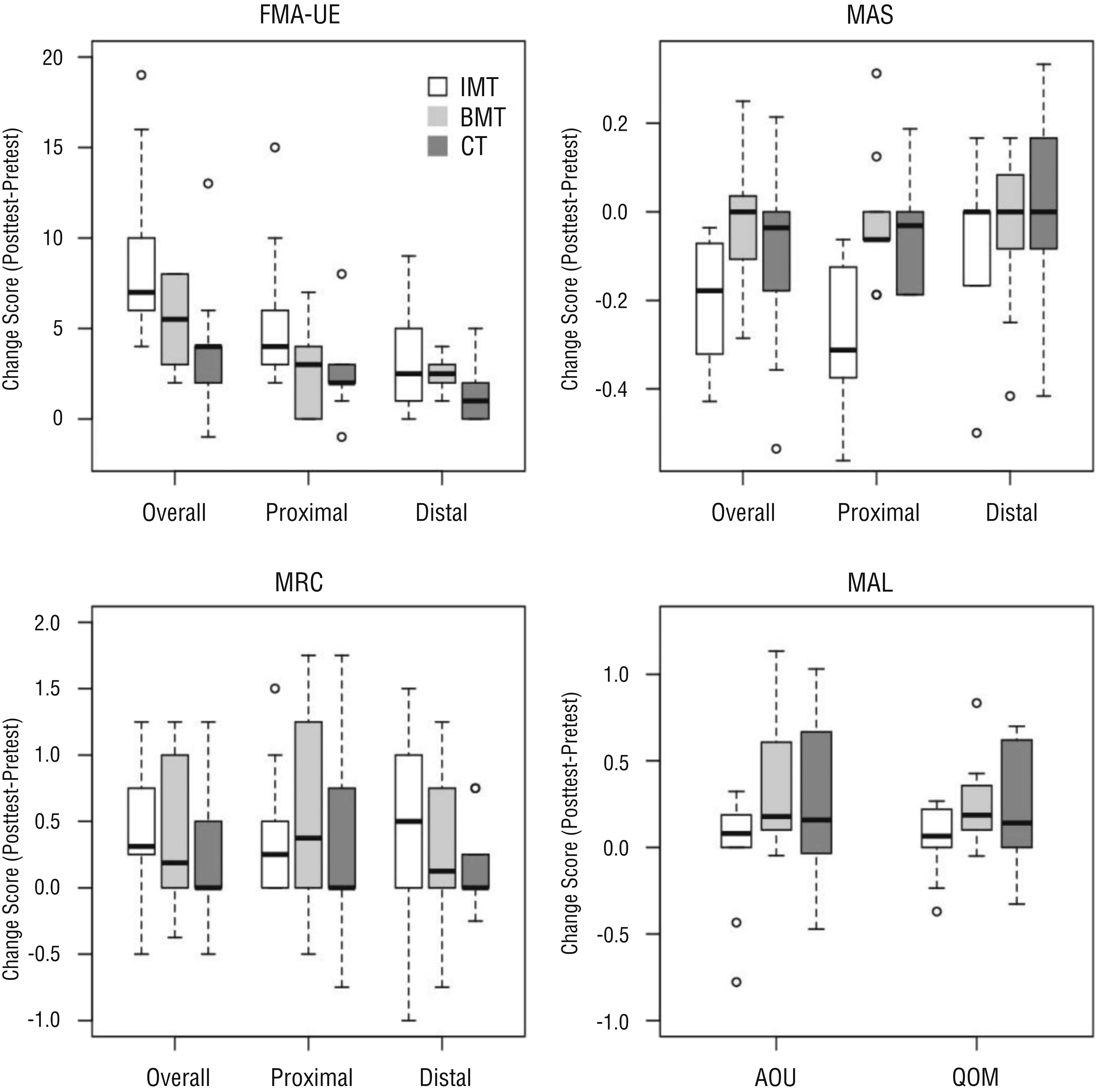
Box-and-whisker plot showing the score changes of outcome measures in the three study groups. The horizontal line in the middle of each box indicates the median, the top and bottom borders of the box mark Quartile 1 and Quartile 3, the whiskers above and below the box extend 1.5 interquartile ranges in either direction, and the circles indicate outliers.
The mean change scores of the overall MAS were 0.20 in the IMT group, 0.01 in the BMT group, and 0.13 in the CT group. The overall and proximal MAS scores were significantly decreased in the IMT group but not in the other two groups. The Kruskal–Wallis rank-sum test also showed a trend for between-group differences in overall and proximal MAS scores. The post hoc analysis showed that muscle tone was decreased in the IMT group compared with the BMT and CT groups in overall (r = .77, p = .01, and r = .54, p = .05, respectively) and proximal (r = .98, p < .01, and r = .61, p = .03, respectively) MAS scores.
For the secondary outcomes, the mean change scores of the overall MRC were 0.75 for the IMT group, 0.62 for the BMT group, and 0.12 for the CT group. The mean change scores of the MAL–AOU and MAL–QOM were 0.18 and 0.19 in the IMT group, 0.15 and 0.16 in the BMT group, and 0.10 and 0.15 in the CT group. The differences in secondary outcomes among the three groups were not significant (all ps > .05). In the within-group analysis, the IMT group showed significant differences between pretest and posttest in the overall and proximal scores on the MRC. The BMT group showed significant changes in MAL–AOU and MAL–QOM scores over time, but the other two groups did not.
Discussion
This preliminary study provides a head-to-head comparison of the IMT (unilateral-based) and BMT (bilateral-based) devices in therapy for patients with stroke. The results indicate that the IMT might lead to greater motor improvements than the BMT and CT. Although both RT groups showed enhancements in muscle power, no between-group difference in muscle power or self-perceived use of the affected arm was found.
The change scores on the overall FMA for the IMT group (8.0 points) and the BMT group (5.5 points) reached a clinically important difference (4.25 to 7.25 points; Page et al., 2012), and the moderate to large effect sizes between the RT groups and the CT group indicate that the motor improvements of the RT groups were more likely to be clinically meaningful than those of the CT group. The comparison between RT and CT was inconsistent in previous studies (Hsieh et al., 2011; Lo et al., 2010). Corresponding to the results of Hsieh et al. (2011), who reported greater motor improvement after RT combined with functional task practice, the benefits for the RT groups in the present study may be associated with the combination of RTs and functional task practice. The RTs might help as a motor priming (Stoykov & Madhavan, 2015), and the functional practice might consolidate the motor learning effects built on the RTs (Hung et al., 2016). However, without the comparison treatment of RTs alone, we could not explicate whether the motor improvements were derived from the combination of RTs and functional practice or from the RTs alone.
The IMT and BMT groups showed changed MRC overall scores (0.75 and 0.62 points) exceeding 10% of the total score, indicating that the change after treatment may be clinically relevant. The IMT group had significantly decreased muscle tone in the proximal upper limb. Previous studies of unilateral RT (Krebs et al., 2007; Yang et al., 2012) indicated a carryover effect in motor function from distal-segment training to the proximal segment. However, the data on the carryover effect on muscle tone were scant.
In the current study, the BMT group did not demonstrate the advantage for proximal motor function reported by previous studies comparing unilateral and bilateral treatments (Lin et al., 2009; Yang et al., 2012). On the basis of research findings that deficits in proximal arm muscle synergies are correlated with motor function (Roh et al., 2015), the proximal arm motor improvements in the IMT group may be related to the normalization of proximal muscle synergies.
In addition, a previous study lent support for the benefits of unilateral intervention on functional improvements (Lin et al., 2009), but our results showed small improvement in the MAL–AOU score (<0.20) for the three groups. These results may reflect the unsuccessful transference of improved function to real life reported in review studies (Hatem et al., 2016; Mehrholz et al., 2015). In contrast, some RT-related studies showed progress in functional use of the affected arm assessed using accelerometrics (Liao et al., 2012). The accelerometer may help detect change that is not large enough for participants to choose a higher score on a self-reported outcome (e.g., the MAL).
Limitations and Future Research
The small sample size may have contributed to the clinically relevant score changes without statistical significance. In the future, researchers should recruit at least 21 participants per group (α = .05, f = 0.40, power level = 0.80) to validate the findings. In addition, adherence to the intervention may have differed by group. Further research could use self-report scales for the measurement of adherence (Bassett, 2003; Chan & Can, 2010). In addition, future research needs to evaluate long-term outcomes and retention of therapeutic gains.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Different therapeutic robots may provide varying benefits, and the devices should be chosen according to therapeutic goals.
RT combined with activity-based practice could be effective in improving upper limb motor function after stroke.
RT may have limited effects on self-perceived daily use of the affected arm. Transition-to-function regimens are needed to facilitate functional transfer to daily life.
Conclusion
This comparative efficacy study suggests that the IMT and BMT devices may provide different benefits for people with chronic stroke. IMT may help patients increase motor function and decrease muscle tone. IMT, BMT, and CT may have similar effects on muscle power, although the IMT and BMT potentially improve muscle power more than the CT. However, the transfer from motor function to functional use of the affected arm was limited in the three groups. Further research based on a larger sample with follow-up assessments is needed to validate the findings of this study.
Supplemental Material
Supplementary material for Comparative Assessment of Two Robot-Assisted Therapies for the Upper Extremity in People With Chronic Stroke
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.022368.pdf for Comparative Assessment of Two Robot-Assisted Therapies for the Upper Extremity in People With Chronic Stroke by Chung-shan Hung, Yu-wei Hsieh, Ching-yi Wu, Keh-chung Lin, Jui-chi Lin, Li-min Yeh and Hsin-pei Yin in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This study was supported in part by the National Health Research Institutes (NHRI-EX105-10403PI, NHRI-EX106-10403PI, NHRI-EX106-10604PI, and NHRI-EX107-10403PI), the Ministry of Science and Technology (104-2314-B-002-019-MY3 and 107-2314-B-002-052), the Healthy Aging Research Center at Chang Gung University (EMRPD1G0241), and Chang Gung Memorial Hospital (BMRP553 and BMRPD25) in Taiwan. The study was registered at ![]() (NCT02319785).
(NCT02319785).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.