
Abstract
Vehicle modifications are often essential to ensure that drivers with disabilities can drive independently and safely. Occupational therapy driver assessors and driver rehabilitation specialists routinely prescribe vehicle modifications on the basis of individualized evaluations and support by rehabilitation interventions. After a literature review and consultation with stakeholders, we identified a resource gap in information to support an evidence-based process for vehicle modification prescription. Using an action research approach, we established content validity for draft guideline items and developed consensus-based draft guidelines for vehicle modification prescription that are ready for trialing by occupational therapy driver assessors. We also propose a practice model for vehicle modification prescription that is applicable to international contexts.
Physical limitations may influence personal, domestic, and community mobility, including the ability to drive a motor vehicle independently. Appropriate vehicle modifications (VMs) can enable people with limited use of their limbs to drive safely, enhancing independent mobility, community and work participation, and quality of life (Pellerito, 2006). Evaluation of a government-funded Vehicle Modifications Subsidy Scheme (VMSS) in Australia found that VMs “are a tangible and practical way to facilitate better social and health outcomes for people with a disability, family members and carers” (Nucleus Group, 2009, p. 3).
VMs include aids or adaptations to manage vehicle operations (e.g., steering, acceleration, and brake functions) and vehicle access (Pellerito, 2006). VMs can be simple, add-on, and low tech (e.g., pedal extensions, steering wheel aids); more complex and expensive postproduction alterations (e.g., lowered floors, automatic ramps); or high tech (e.g., integrated primary vehicle controls such as lever brake acceleration and joystick steering systems; Di Stefano, 2017; Pellerito, 2006).
In Victoria, Australia, the right to financial compensation for VMs has been legislated in landmark workplace and transportation legislation such as the Accident Compensation Act (Victorian Government, 1985) and the Workplace Injury Rehabilitation and Compensation Act (Victorian Government, 2013). Financial costs for aids, including modification of vehicles for injured drivers, can be substantial. In 2009, the Transport Accident Commission in Victoria paid AU$123.9 million for aids and equipment, including transportation support for claimants with serious injuries (Access Economics, 2009). In the United States, workers’ compensation and state vocational and rehabilitation agencies fund driver rehabilitation and VMs (Pellerito, 2006). Given the significant investment required for VMs, prescription processes should be articulated that are evidence based, defensible, and practicable to optimize not only long-term driver independence and safety but also resource use.
Occupational Therapy Driver Assessors and Driving Rehabilitation Specialists
In Australia, occupational therapy driver assessors (OTDAs), who are similar to North American driving rehabilitation specialists, are the primary health professionals supporting drivers with disabilities to establish or maintain the ability to drive independently (Occupational Therapy Australia, 2015). Although OTDAs consider functional, lifestyle, and role contexts when configuring vehicle–driver interfaces in VM application, some aspects of OTDA practice require improvement. Hopewell (2002) explored VM prescription issues and identified the need to more clearly articulate “the goals and mechanism of adaptive driving rehabilitation” and “how recommendations are to be made to the patient, to the family, and to other medical and regulatory personnel” (p. 57). This conclusion was supported by findings from an ADED (the Association for Driver Rehabilitation Specialists) member survey that identified a broader need to “clarify and define driver rehabilitation programs [for older drivers], identify types of services, and categorize levels of provider knowledge and credentials” (Lane et al., 2014, p. 178).
Studies exploring clinical decision making and OTDA driving evaluation practices have identified several unresolved challenges. Korner-Bitensky et al. (2010) examined occupational therapy driving-related clinical practices (N = 133 participants) and highlighted a need for enhanced professional capacity in assessment and intervention. Vrkljan et al. (2015) used four case studies to investigate clinical reasoning by 46 driver assessors (89% were occupational therapists). They found large variability in assessment tests used and decisions made in conducting driving evaluations for people with paraplegia. These studies support the need for consistent professional training and practice.
The first-ever postgraduate OTDA training program was conducted in Australia in 1987 (Caust, 1988). Since then, Australian OTDA practices have been based on postgraduate university coursework, general professional competency standards, and jurisdiction-based OTDA guidelines (e.g., Roads Corporation, 2008). In North America, ADED’s (2009) Best Practice Guidelines for the Delivery of Driver Rehabilitation Services provide comprehensive guidelines for driver assessment and evaluation. However, none of these resources currently provides specific, detailed support material to guide the complex process of prescribing VMs to match individual capacities (Di Stefano et al., 2012; Occupational Therapy Australia Victoria Division, 1998).
The VMSS evaluation (Nucleus Group, 2009) involved interviewing stakeholders (including OTDAs) and analyzing resource utilization and prescriber and user characteristics (drivers, passengers, family, and caregivers). Results indicated that OTDAs wanted detailed VM prescription guidelines to improve VM-related assessment, evaluation, and intervention in driver rehabilitation practice (Nucleus Group, 2009). Vehicle-related technology advances have increased the number, sophistication, and cost of VM options, resulting in more complex clinical decision making (Di Stefano, 2015; Roads Corporation, 2008). Related professional practice resources are needed that use an evidence-based approach to support reliable, consistent practice (Layton, 2008).
Research Question and Knowledge Translation Purpose
To promote consistent VM prescription practice among OTDAs, we sought to address the identified gap in VM prescription guidelines by working collaboratively with OTDAs in an action research process. Specifically, we sought to clearly articulate components and stages of the VM prescription process, establish content validity for draft guideline items, and confirm practicability of items for input into a draft set of consensus-based guidelines and an accompanying model practice framework.
Method
Design and Participants
Participatory action research methods were applied in this study. Specifically, we used a survey, focus groups, and consultation meetings to gather input from relevant stakeholders, such as expert driver assessors, clients, caregivers, and payment agencies (Bergold & Thomas, 2012). Action research processes seek to acknowledge and use participant expertise in the process of investigating phenomena, developing meaningful outcomes, and optimizing both ownership and application (Koshy et al., 2010; Meyer, 2000), making it an ideal approach for the development of guidelines for prescribing and implementing VMs.
Ethics and organizational approval was obtained from the relevant university, management committees, and state licensing authority. A project advisory group (PAG) was convened to support, inform, and ratify the research questions, methods, tools, and project outcomes. The 13 PAG members, who were identified through key driving-related stakeholder organizations and responded to email invitations, consisted of representatives from compensation providers (2), advocacy organizations (3), the licensing authority (1), and health agencies (2); occupational therapy university staff (2); a vehicle engineer (1); and OTDAs (2). The PAG met as a group twice, once at the start to ratify the survey and draft guideline items and again after survey and focus group data collection, and members undertook review tasks between meetings.
The five key stages in the project, with data collection occurring over 6 mo, are outlined in Figure 1. A literature review and ergonomic and task analysis informed the initial development and validation of the survey and draft guideline items. After PAG ratification, we implemented the survey and focus groups with OTDAs. All OTDAs in Victoria, Australia, listed with the licensing authority as being active in research, education, or practice in 2014 (N = 65) were invited by email to complete a survey anonymously over a 4-wk period and to attend a focus group held at the end of this period.
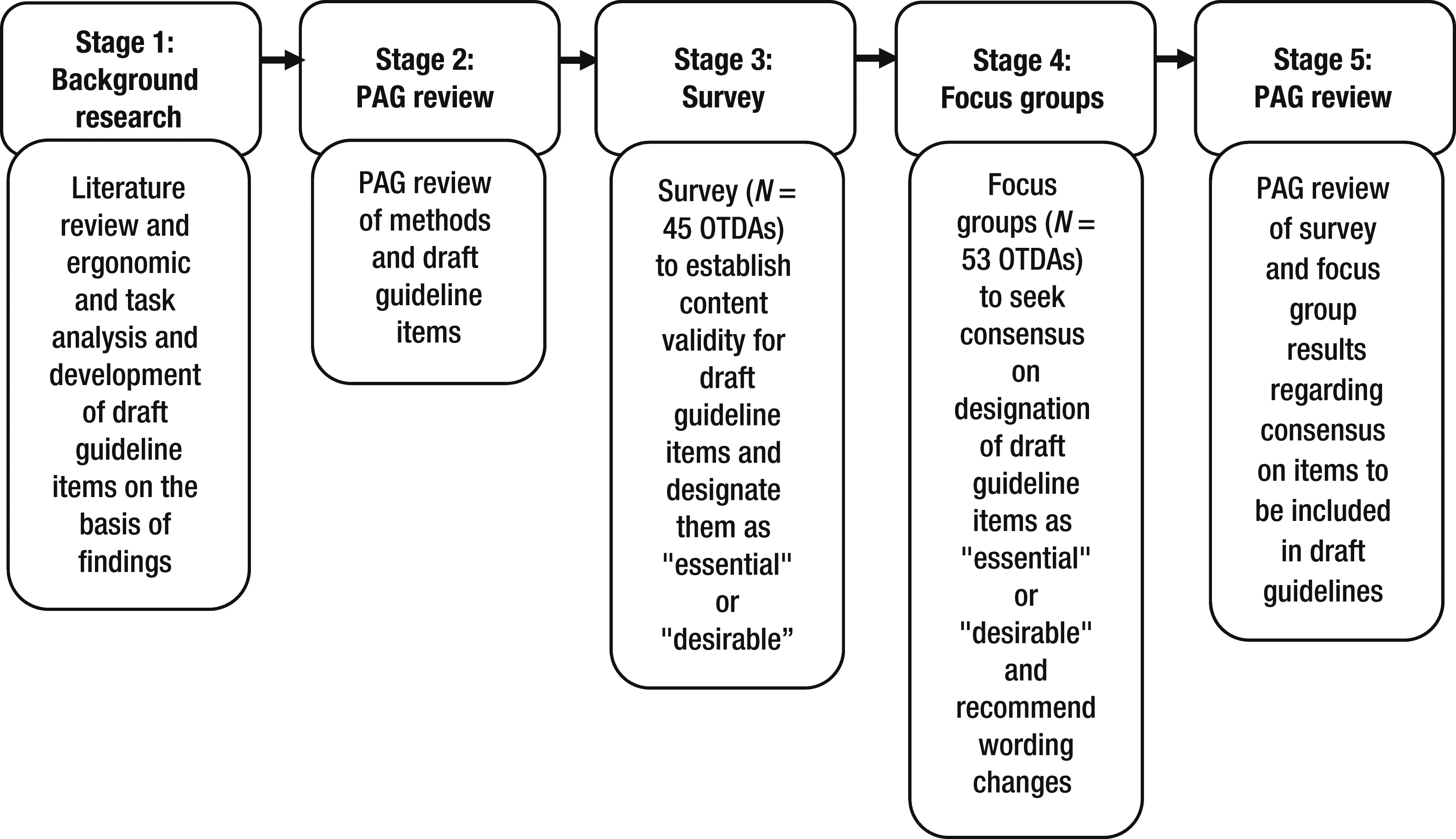
Participatory action process used for guideline development showing key stages and activities.
Of the OTDAs eligible to participate, 45 returned completed surveys, and 53 attended focus groups (81.5% overall participation rate). Of the survey sample, more than 80% had ≥6 yr of OTDA experience, and respondents worked predominantly with drivers of all ages (46%) or older drivers (43%). Most respondents worked in the field part time, and they conducted an average of eight evaluations per month.
Guideline Development Process and Resources
A literature and resource review informed the study methodology, methods for development of draft guideline items, and confirmation of content validity for the draft guidelines and practice model. After developing our research question, we used key search terms to interrogate databases (including Embase, MEDLINE, ProQuest, and CINAHL); consulted conference, university, research institution, and government websites looking for references, textbooks, resources, technical reports, and guidelines; and supplemented these sources with hand searches of reference lists. We located and appraised (using Centre for Evidence-Based Medicine, 2016, appraisal tools as relevant) 11 research articles, 6 magazine or newsletter articles reporting personal experiences with VMs, 3 practice guideline resources, and several online resources providing consumer advice. As a team, we synthesized the evidence and applied it to the ergonomic and task analysis framework to develop the first draft guidelines.
Several resources were particularly useful. The AGREE II tool (Brouwers et al., 2010), which assesses evidence-based guideline processes for development and reporting, was used to guide stakeholder involvement and ensure rigor of content development. The nationally adopted Competency Standards for OTDAs (Occupational Therapy Australia Victoria Division, 1998; a revision is currently under review) were selected as a model to enhance guideline usability. Guideline content incorporated relevant sections of the Competency Standards for OTDAs as well as the European Car-Adaptations for Disabled Drivers: Requirements, Test Methods and Best Practise Guidelines (European Committee for Standardisation, 2013) and the Vehicle Features Matrix (Independent Living Centres Australia, 2014). The Vehicle Features Matrix was developed to help clinicians identify particular vehicle design features to address specific functional limitations. Materials from the 2014 ADED conference and VM workshop supported draft item content validity (Di Stefano, 2014).
Survey Tool
A survey tool including the draft VM guidelines was used to establish content validity. In the absence of an available purpose-specific survey tool, we designed an instrument that was ratified by the PAG before distribution. Draft guideline items were informed by the literature review, the ADED workshop, and an activity and systems ergonomic analysis. This analysis identified human factors and OTDA assessment process aspects that together define important key driver–vehicle–environment interactions (Di Stefano & Stuckey, 2015).
The first two sections of the survey gathered respondent and client background information (n = 15 items). Remaining items (n = 49) elicited responses to action statements relating to proposed VM prescription principles and guidelines. Survey content followed the logical VM prescription process sequence in six sections:
General assessment and prescription principles (e.g., use standardized assessment tools when available, evaluate the current vehicle for suitability before considering a new vehicle, consider low-tech VMs before high-tech VMs)
Person-centered factors (driver variables; e.g., impairments, activity limitations, participation restrictions, ergonomic considerations, positioning)
System factors influencing VM provision (e.g., financial resources and constraints, environment of use, driver licensing authority approval and registration requirements)
Driving as an occupation (e.g., life roles requiring driving, such as homemaker, caregiver or parent, worker)
VM training issues (e.g., qualified instructors, access to equipment and modified vehicles, funding)
OTDA evaluation of VMs, including in-vehicle evaluation (e.g., compare fitted VMs to specifications provided, considerations for stationary and on-road in-vehicle use).
Sections 1–6 required respondents to rate the importance or relevance of each action statement to their own VM prescription practice as follows: all the time, sometimes, never, don’t know, or not applicable. Each section included space for comments where participants could add draft guideline items or comments (the survey is available from the first author).
Focus Groups
Three concurrent focus groups of 2 hr duration were coordinated by three facilitators experienced in focus group implementation following established procedures (Krueger & Casey, 2014). Each participant attended only one group. Written information was provided to participants before attendance as part of the survey explanatory information. The purpose of the focus groups was to systematically discuss, review, and validate all draft guideline items in the previously circulated survey and to seek consensus agreement on item inclusion as “essential” or “desirable” on the basis of percentage of participants who selected all the time or sometimes regarding relevance of items to their own practice. Facilitators also sought recommendations for changes (e.g., clearer wording). A note taker (experienced occupational therapist) recorded comments, wording changes, and number of participants who agreed or disagreed with inclusion of each item.
Data Collection and Analysis
Completed surveys were returned by mail or collected at the end of the focus groups. Focus group attendance was in person or by video conference. Quantitative survey and guideline consensus data (responses to relevance and importance ratings) were extracted and entered into IBM SPSS Statistics (Version 21; IBM Corp., Armonk, NY) for descriptive analysis. Qualitative data from the surveys (participant comments under Sections 1–6) and focus groups (note taker comments) were collated, and two researchers collaboratively applied content analysis to identify and summarize common issues (Elo & Kyngäs, 2008). Common issues and total responses to item ratings were then reviewed by the PAG. In the absence of prescribed criteria relevant to this occupational therapy practice domain, the PAG unanimously determined that 90% should be the objective cutoff score for establishing consensus agreement levels.
Results
Clients’ Vehicle Modification Needs
Survey respondents were asked to estimate the proportion of their clients who had access to different funding sources to pay for their VMs. The majority of the 45 respondents who returned completed surveys (73%) reported that <50% of their clients had VM funding from accident compensation; 32% reported funding from other government sources (e.g., VMSS). Only 25% reported that VM selection was compromised because of affordability. When reporting on types of VMs required, the majority of respondents (84%) indicated that only small numbers of clients required major (more expensive) VMs. Most respondents (84%) reported that all or most of their clients needed driving lessons targeting VM use.
Responses to Draft Guideline Items
The survey items outlining proposed guideline principles or components were validated by the PAG and grouped into seven categories (categories had different numbers of items). No survey respondent suggested a new item or rejected any of the proposed items or categories. We sought to identify consensus in the survey and focus group results on inclusion of individual draft guideline items. Survey responses revealed a consensus agreement for inclusion of the 39 (of 49) items deemed “essential” (% agreement ≥90%). Of the 10 remaining items, 9 achieved a “desirable” rating (% agreement 80%–89%). The 10 items with lower levels of agreement were generally associated with role differentiation and professional knowledge limitations. After removal of some items and integration of several items into combined items, the final draft PAG-approved guidelines consisted of 42 items, the majority labeled as “essential.” The consensus ranges for items in each category are provided in Table 1.
Consensus on Draft Guideline Items Considered Essential for Inclusion, by Category
Note. VM = vehicle modification.
Percentage of participants who selected all the time or sometimes regarding relevance of items to their own practice. bOne item in this category achieved <80% agreement and therefore was not categorized as either “essential” or “desirable.”
The content analysis of survey and focus group comments identified suggested changes to improve clarity and meaning of items. Regarding OTDA role, boundaries, and differentiation, participants clarified their perceived role as assessors as distinct from the roles of vehicle engineers, installers, and driving instructors in the following ways:
The majority of OTDAs do not have or need technical VM-related expertise if they can rely on other professionals; OTDAs focus on driver functional requirements.
The OTDA role is to prescribe or make evidence-based recommendations rather than to negotiate with insurers, installers, or suppliers regarding costs or compliance requirements.
In this jurisdiction, OTDAs do not usually follow up after installation; funders will not pay for this service, relying instead on vehicle installers.
Participants also highlighted the following concerns related to current practice that were relevant to the proposed model of practice:
Access to view, trial, and compare VMs needs to improve.
It is difficult to assess whether new products comply with applicable standards.
Training with the exact prescribed equipment can be difficult if driving instructors do not have these adaptations installed. In this jurisdiction, OTDAs do not usually have access to a test vehicle, relying instead on driving instructors to supply both vehicles and VMs for test driving.
Appropriately skilled driving instructors who are both accessible and affordable can be difficult to find.
Development of Draft Guidelines
After analysis of survey and focus group data, including PAG consultation, we addressed requests for item wording clarification and further refined the draft guidelines to 42 items in seven categories: (1) general assessment and prescription principles (8 items); (2) person-centered factors (9 items); (3) system, financial, and environmental factors (5 items); (4) occupation of driving, activity issues, and training (5 items); (5) evaluation of VMs—general (4 items); (6) evaluation of VMs—in-vehicle component (stationary; 5 items); and (7) evaluation of VMs—on-road component (driving in traffic; 6 items). The project outcomes and draft guidelines are in the public domain (Institute for Safety, Compensation and Recovery Research, 2014).
Discussion
Current guidelines for driver rehabilitation include detailed procedures for off-road impairment screening and on-road driving assessment (e.g., ADED, 2009). However, best practice guidelines have been developed only for Australia and North America (not for the United Kingdom or Europe), and these provide limited guidance on procedures for VM prescription. For example, current guidelines recommend assessment of client abilities (e.g., to operate primary controls) and of completed modification appropriateness, in the absence of decision-making cues and without specific VM-related assessments. The proposed draft guidelines provide specific supplementary details to guide reliable service delivery for occupational therapist driving specialists in any jurisdiction. The seven categories in the proposed guidelines each have multiple precise items, performance criteria, and cues to guide practice. For example, Section 5 covers the post-installation evaluation of VMs and includes four items and related criteria and cues. The following is an example of one item and its cues:
5.3 fitted aids/VMs match prescription provided and suit the driver’s capabilities
Cues: (a) Type/location of modified controls appropriate, within relevant limb’s reach envelope; (b) driver demonstrates capacity/strength to generate forces required to safely and (c) reliably operate the controls; (d) detailed requisition order/quote for products (name/model number) provided; and (e) if required, diagrams/photos showing installation location in vehicle cabin provided.
Streamlining the VM prescription process through more detailed guidelines should assist OTDAs to provide better quality service, resulting in improved client outcomes. An exploratory study by Lenker et al. (2013) used focus groups to determine the impact of various service delivery factors (including assessment procedures) on the consumer experience of assistive technology devices (including VMs). Lenker et al. identified several common negative experiences associated with device acquisition, including service and acquisition process problems, and recommended that research assimilating the consumer perspective address “whether or not a negative device acquisition experience resulted in negative long-term outcomes” (p. 377).
Gagliardi and Brouwers (2012) analyzed the implementation of health care manuals and factors affecting guideline use. They found that implementation of guidelines can be impaired by extrinsic factors (e.g., lack of resources to effectively implement recommendations) and intrinsic factors inherent in the guidelines (e.g., lack of applicability to consumers) that could best be addressed by involving consumers in development. We attempted to address intrinsic factors in guideline development by using a participative approach to ensure the incorporation of the perspectives of user groups (OTDAs and consumers), a method previously applied in the area of assistive mobility technology tools related to mobility screening and power wheelchairs (Kamaraj et al., 2014). Abrahamson et al. (2012) examined facilitators and barriers to guideline use among nurses and also identified lack of resources as an extrinsic barrier to implementation.
We identified two potential extrinsic barriers, lack of funding for acquiring VMs and lack of funding for postinstallation evaluation of VMs, both of which may be relevant to occupational therapist driving specialists in North America and internationally. Although the post-installation evaluation element of the guidelines has the potential to improve consumers’ VM acquisition experience, funding barriers may preclude implementation of this component. Lobbying funding agencies to address this gap could be considered. The finding that only a small proportion of OTDAs reported compromised VM acquisition when no funding was available could be a result of selection bias; drivers may not seek OTDA services for VMs unless they have sufficient funding resources.
Draft Vehicle Modification Prescription Model of Practice
A graphic of the draft VM prescription model (Figure 2) was developed to pictorially represent the interacting system factors that influence safe and effective VM prescription and the central role of OTDA interventions as reflected in the draft VM prescription guidelines. This VM prescription model is intended to be relevant to any practice context or jurisdiction internationally. Drawing on the Person–Environment–Occupation Model (Law et al., 1996), the model posits that occupational performance is determined by the complex interrelationships among factors centered on the person, the occupation or activity in which they are participating, and the environment in which they are situated. An occupational analysis of driving includes consideration of the driver, driving task characteristics, duration and complexity, and broader environment, including public safety and other regulatory and administrative requirements. Optimal occupational performance is promoted by occupational therapy interventions enabling a good fit among all stakeholder, driver, environment, and vehicle use considerations.
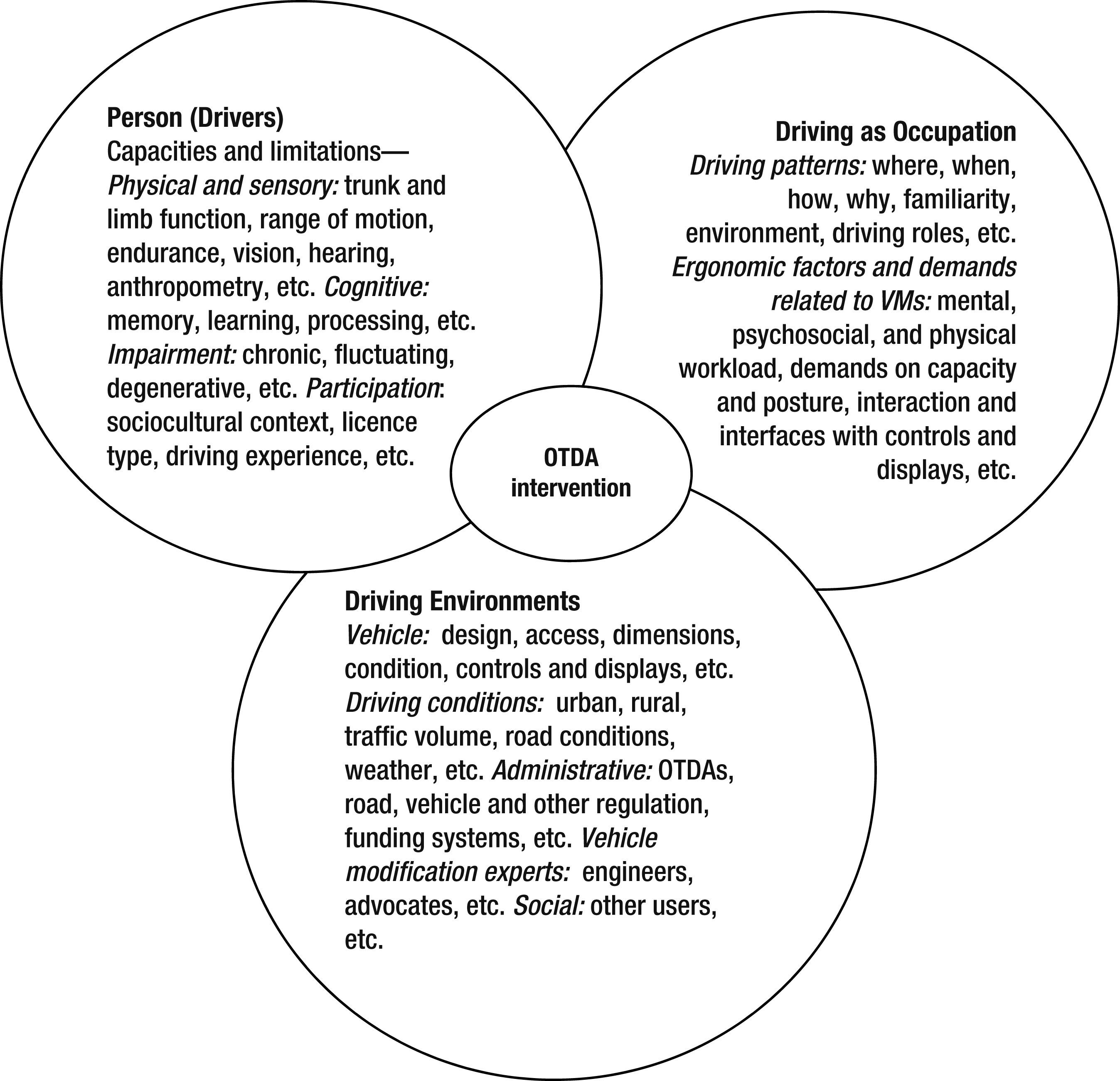
Draft vehicle modification prescription model of practice.
Future Research
The next stages for this project involve usability trialing during VM prescription to gather quantitative and qualitative data from practitioners and clients. When finalized, these guidelines will assist with OTDA and certified driver rehabilitation specialist training and improve overall consistency and reliability of service delivery, paving the way for further international applicability research.
Implications for Occupational Therapy Practice
Occupational therapy practitioners are in a unique position to provide effective driver rehabilitation services, including VM prescription. The results of this study have the following implications for occupational therapy practice:
Current VM prescription guidelines lack sufficient detail to optimize reliable standardized practice.
VM prescriptions need to be clear, concise, and appropriately matched to the driver’s needs to ensure clinical and cost-effectiveness.
These draft VM prescription guidelines are supported by a practice model, offer improvements to current practice, and are ready to be trialed.
Conclusion
This study reinforces the importance of VMs to drivers with disabilities and drew on a large sample of experienced OTDAs to develop prescription processes. A strength of this study is the active involvement of a wide range of stakeholders, including VM users, OTDAs, regulatory and funding groups, and others with expertise in the management of driver rehabilitation programs. This participative approach helps ensure the practical relevance of the research and provides a sound basis for further trialing of the guidelines. Improvements proposed are centered on operational definitions, item phrasing, and role clarification across OTDAs, driving instructors, and installers. Study findings contribute to development of the world’s first set of detailed draft VM prescription guidelines, which are now ready for usability trialing in any international jurisdiction.
Footnotes
Acknowledgments
We thank the participants, project advisory group members, VicRoads, Disabled Motorists Australia, and Australian Quadriplegics Association contributors for their support. Thanks also to the reviewers who offered helpful advice. Funding for this study was received from the Institute for Safety, Compensation and Recovery Research supported by the Transport Accident Commission and WorkSafe Victoria.