
Abstract
After formal rehabilitation, people with chronic stroke are recommended to continue exercising independently to prevent deterioration (Billinger et al., 2014) of body functions and structures and to maintain and improve their functional abilities and health-related quality of life (Broeks et al., 1999). This recommendation is especially important for the weaker upper extremity (UE), which people with chronic stroke often do not use enough in daily living (Rand & Eng, 2015) because of restricted motor ability and learned nonuse (Taub et al., 1993). However, motivation for self-training is low, and self-training is frequently discontinued (Nicholson et al., 2013).
The Graded Repetitive Arm Supplementary Program (GRASP) was developed to provide the opportunity for ongoing training of the weaker UE during inpatient subacute stroke rehabilitation (Harris et al., 2009). This self-training program includes exercises and activities that incorporate the weaker UE and use everyday items that are presented in a structured, illustrated manual. Self-training using the GRASP has been reported to be more effective than an educational program in improving the weaker UE of patients with subacute stroke during rehabilitation and as effective as using video games at home (Adie et al., 2017).
Active video games, which are known to enhance enjoyment and motivation (Lohse et al., 2013; Saposnik & Levin, 2011) by using music, entertainment, and embedded competition, can facilitate purposeful movements of the body and UEs (Rand et al., 2014). In addition, video games elicit challenging, intensive, repetitive and task-specific training, which may help induce favorable neuroplasticity (reorganization) of the brain (Nudo, 2007; Saposnik & Levin, 2011). Over the past decade, clinicians have used active video games in therapy sessions to achieve therapeutic goals (Weiss et al., 2014). For example, several active video game consoles have been used to improve active UE movement of people with chronic stroke in individual (Pietrzak et al., 2014) or group (Givon et al., 2016) settings while supervised by a therapist.
A few home-based specialized programs using video game technology have been assessed for feasibility and initial effectiveness. For example, the virtual glove, which encourages repetitive hand movements such as reaching and grasping while playing three games, was developed and found to be feasible (Standen et al., 2015) with varying levels of independent use by 17 people with chronic stroke. A program using a dynamic wrist and hand orthosis combined with a video game was developed for self-training of the weaker UE of people with chronic stroke (Nijenhuis et al., 2015). Twenty-four participants who independently performed self-training for a mean of 105 min/wk improved their UE function and quality of life (Nijenhuis et al., 2015). However, these tools are costly, not widely available for clinical use, and require the use of devices worn or attached to the hand. The use of commercial video game consoles for self-training might be more available, affordable, and easier to use despite the fact that these consoles were not developed for rehabilitation.
Recently, the Nintendo Wii (Nintendo, Redmond, WA) has been successfully used in a large randomized controlled trial that offered home-based training for participants with subacute stroke (Adie et al., 2017). However, the Wii movements made with the Wiimote are not monitored by a camera, and even small hand movements are often sufficient to play the games. Therefore, this console might not be the best choice for UE self-training, but whether other consoles can be used successfully for self-training is unknown.
The aims of our study were to compare the feasibility of, adherence to, and satisfaction with a newly developed self-training protocol using commercial video games and a traditional self-training program for participants with chronic stroke.
Method
Population
Stroke was defined according to the World Health Organization definition (Sacco et al., 2013, p. 2065): “rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.” Diagnosis was confirmed by clinical assessment and a positive computed tomography or magnetic resonance imaging scan. Eligibility criteria were as follows: age 18–80 yr, onset of stroke within 6–36 mo before the study, living in the community with a family member or a caregiver (for physical support and safety and to enhance motivation to achieve greater UE improvement; Harris et al., 2010), ability to walk at least 10 m (with or without assistance), mild to moderate UE weakness (defined by a Fugl-Meyer Motor Assessment [FMA; Fugl-Meyer et al., 1975] UE subtest score between 15 and 55 of a maximum of 60 points), and no significant cognitive impairment that might interfere with training adherence (Mini-Mental State Examination [MMSE; Folstein et al., 1975] score > 21 points). The FMA is commonly used to assess the motor impairment of the weaker UE and is valid and reliable (Hsieh et al., 2009), and the MMSE is a valid and reliable screening test for cognition poststroke. Participants with other neurological conditions or epilepsy were not included in the study.
This study was approved by the Chaim Sheba Medical Center Helsinki Committee and Tel Aviv University’s ethics committee. All participants provided written informed consent. Participants were recruited from discharge lists from a large rehabilitation center; in addition, advertisements were hung up in other outpatient settings.
The following assessments were used to characterize the participants: The Functional Independence Measure® (Keith et al., 1987), administered as an interview (Daving et al., 2001), was used to assess the participants’ independence in basic activities of daily living (BADLs), and the Functional Reach Test (FRT; Duncan et al., 1990) was used to assess their dynamic standing balance. The FRT measures the distance between the length of the arm and a maximal forward reach in the standing position while maintaining a fixed base of support. The difference in centimeters between standing and leaning forward was calculated. The Timed Up & Go (TUG) test (Podsiadlo & Richardson, 1991) is a performance-based tool to assess balance and mobility in people who have had a stroke (Hollands et al., 2010). The TUG test measures the time it takes to stand up from a chair, walk 3 m, turn around and walk back to the chair, and sit down. The time taken to complete the TUG test has been shown to predict falls in community-dwelling older adults and people with stroke (Ng & Hui-Chan, 2005). Grip strength of the weaker hand was also assessed using a Jamar dynamometer, and it was measured in kilograms on the basis of the mean of three trials. The assessments were administered by experienced occupational therapy practitioners who were blind to allocation to the self-training condition.
Self-Training Protocol
Video Game Self-Training Protocol.
In the experimental group, participants received a video game console and were requested to play video games that facilitated UE and trunk movements. One of two commercial video game consoles was used for the self-training protocol: the Microsoft Xbox Kinect (Microsoft Corp., Redmond, WA) and Sony PlayStation EyeToy (Sony Interactive Entertainment, Tokyo, Japan). Both consoles are considered to be video-capture systems; they include a sensor (Kinect) or camera (EyeToy) to capture the UE and trunk movements used to play the games.
One of the occupational therapy practitioners brought the video game console to each participant’s home and connected it to the television. She also arranged a safe playing area (moved furniture, placed a chair close by for support, etc.) and taught the participant how to perform the self-training. Three to five games were selected for each participant.
Participants who were safe to play while standing were encouraged to stand. Safety status was determined on the basis of the FRT’s cutoff scores for risk of falling (<15 cm; Acar & Karatas, 2010), which assess dynamic standing balance; the TUG test (>14 s; Andersson et al., 2006), which assesses mobility; and the therapist’s impression after watching the participant play for a few minutes while standing. If the occupational therapist did not think the participant was safe to stand and play, she instructed the participant to play the video games while seated. Participants who played video games while seated were given the EyeToy, which can be played while seated, instead of the Xbox Kinect, which reacts well only when playing in standing. All participants were encouraged to play the games with their weaker arm.
Traditional Self-Training Protocol.
For the control group, the GRASP (Harris et al., 2009) was used. The GRASP includes instruction manuals for three different levels of exercises and activities and an equipment kit (including everyday items such as a towel, a ball, and pegs). Participants were requested to perform the exercises with their weaker arm. Three additional lower extremity exercises (stretching, marching, and stepping) were added to the GRASP. All upper and lower extremity exercises were performed seated, as the GRASP was originally developed.
Outcome Measures
Adherence.
During the 5-wk intervention period, participants documented their self-training time on a log sheet. The total training hours per week and total training hours for the 5 wk were calculated. Self-training time during the 4-wk follow-up period was also calculated.
Satisfaction.
For each daily session, participants rated their perceived enjoyment on a scale ranging from 1 (did not enjoy it at all) to 5 (enjoyed it very much) and their perceived exertion on the Borg Rating of Perceived Exertion scale (Borg, 1990), which ranged from 6 (no exertion at all) to 20 (maximal exertion). Weekly mean daily enjoyment and perceived exertion were calculated. In addition, satisfaction was assessed after the 5-wk self-training intervention by means of a questionnaire on which participants were asked to rate their overall satisfaction with and enjoyment of the self-training program on a 5-point Likert scale ranging from 1 (not satisfied/did not enjoy) to 5 (extremely satisfied/enjoyed). Participants also rated their perceived benefit from the program in terms of improving their weaker UE and balance on a 5-point Likert scale, ranging from 1 (no perceived improvement) to 5 (substantial improvement). Participants also rated the amount of family assistance they needed to perform the self-training (very little, some, and substantial).
Procedure
We used a simple block randomization procedure (ratio 1:1) to randomly allocate participants to receive either video game or traditional UE self-training for 5 wk; all participants were requested to perform self-training for 1 hr/day, 6×/wk (30 sessions overall).
Protocol Delivery and Follow-Up of the 5-Week Self-Training Intervention.
A home visit was conducted by an occupational therapy practitioner who instructed the participants in how to perform the self-training and to follow the instructions of the color illustrated manual. Participants were also taught to log their self-training time and to rate their enjoyment and perceived exertion after each training session. Participants were requested to report any adverse effects such as pain, dizziness, sore muscles, or falls that occurred during or after the self-training sessions. An additional home visit took place 2 wk after the first one to verify that the self-training was performed according to the protocol and to problem solve issues if they arose. For the first week, the occupational therapist was in daily contact (by phone or text message) with the participants, then weekly contact took place in Weeks 2–5. Participants sent their log page (using their smartphone or by fax) to the therapists at the end of each of the 5 wk. Participants were encouraged to contact the therapist if they experienced any adverse effects or if they encountered any technical problems.
4-Week Follow-Up Period.
At the end of the 5-wk intervention, participants were instructed to keep the equipment (console or exercise kit) for an additional 4 wk, but the self-training was optional and did not include the weekly contact with the therapist. At the end of the 4-wk follow-up period, participants from both groups were requested to return the equipment to the rehabilitation center, where the follow-up assessments were conducted. Data from the daily log sheets were then taken and calculated.
Data Analysis
Each participant’s data are presented separately to allow an in-depth understanding of potential suitability of the self-training programs for other participants. Statistical analyses were conducted using IBM SPSS Statistics (Version 23.0; IBM Corp., Armonk, NY). Descriptive statistics for the population, self-training time, enjoyment, and perceived exertion and satisfaction are presented. Differences between groups regarding demographic and stroke information, self-training time, enjoyment, and exertion were analyzed using an independent-samples t test for continuous variables and χ2 test for dichotomous variables. Statistical significance was set at p < .05. Because this was a pilot study, sample size calculation was not performed.
Results
One hundred forty-two people with chronic stroke were approached and screened by phone, and 24 participants were recruited into the study and were randomized (Figure 1). Of these, 13 participants (9 men, 4 women; ages 33–74 yr; mean [M] time poststroke = 19.9 mo, standard deviation [SD] = 11.3) took part in the video game self-training program, and 11 (6 men and 5 women; ages 58–80 yr, M time poststroke = 13.0 mo, SD = 6.0) took part in the traditional self-training program. They were independent in BADLs and had intact cognition. Table 1 describes each of the 24 participants in terms of demographics, stroke information, and motor and functional ability. No significant differences were found between groups for age, t(22) = −1.5, p > .05; education, t(22) = −0.28, p > .05; months since stroke, t(22) = 1.7, p > .05; gender, χ2 = 0.069, p > .05; dominant hand affected, χ2 = 1.5, p > .05; and use of walking aid, χ2 = 1.9, p > .05. However, the participants in the video game group had significantly higher Functional Independence Measure scores, t(22) = 2.2, p = .05, indicating that they were more independent in BADLs.
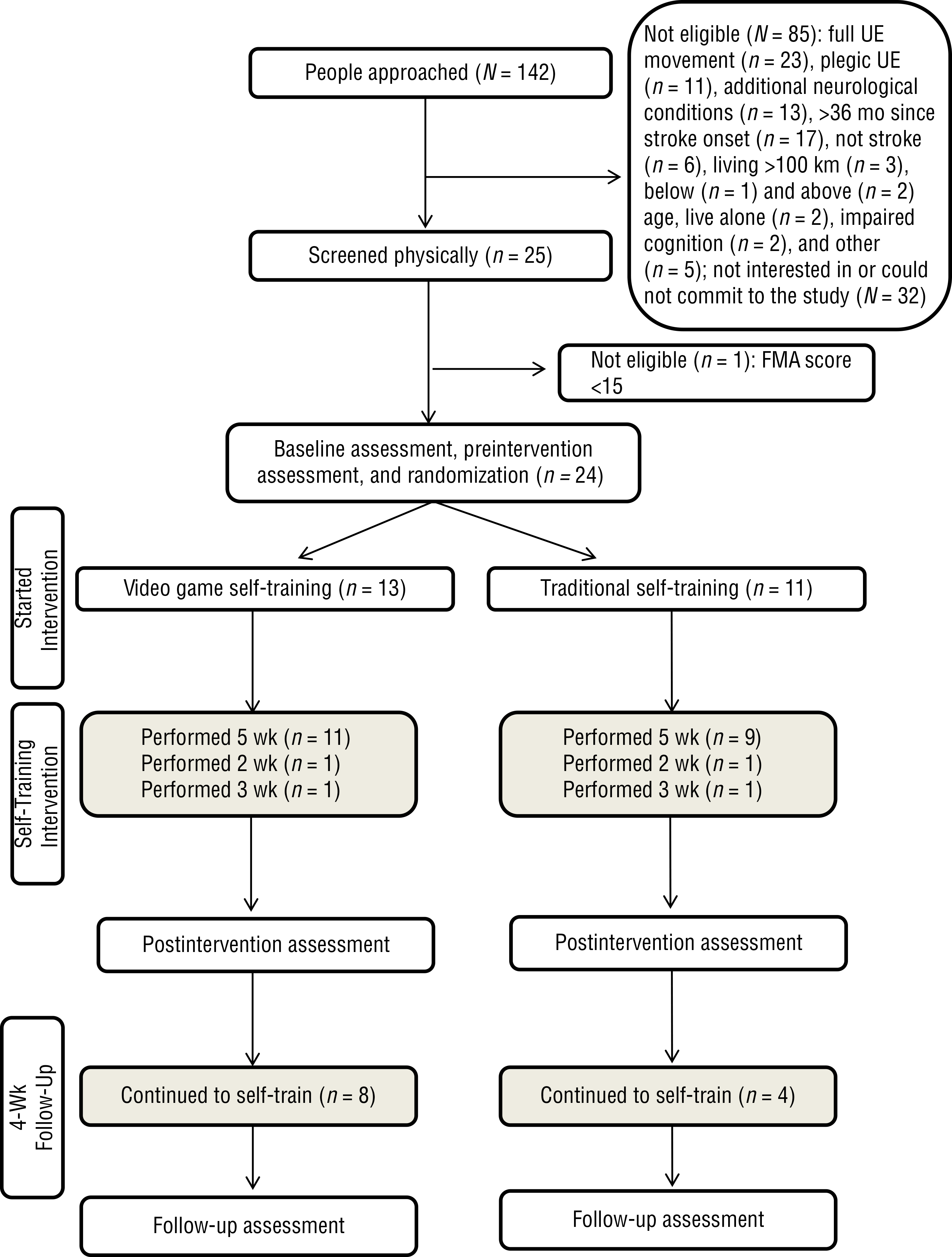
CONSORT flow diagram of recruitment and adherence.
Demographics, Stroke Information, and Motor and Functional Ability of Each Participant
Note. For the FMA, scores could range from 0 to 60; for the MMSE, scores could range from 0 to 30; and for the FIM, scores could range from 18 to 126. F = female; FIM = Functional Independence Measure; FMA = Fugl-Meyer Motor Assessment; FRT = Functional Reach Test; M = male; M = mean; MMSE = Mini-Mental State Examination; N = no; SD = standard deviation; TUG = Timed Up & Go Test; Y = yes.
Participant played the video games seated.
Missing data for some measures because participant became tired and did not complete all assessments.
Of the 13 participants in the video game self-training group, 10 played video games while standing; 9 used the Xbox Kinect, and 1 participant did not have enough UE movement to operate the Xbox Kinect and played the EyeToy standing. Three participants used the EyeToy while seated. Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) lists the video game console, CD, and games most often used by each of the 13 participants. Set up of the console was often challenging but was overcome by the therapists. Falls or other adverse effects were not reported during the 5-wk intervention or 4-wk follow-up periods for any of the 24 participants.
Adherence
Eleven of the 13 participants in the video game self-training group and 9 of the 11 participants in the traditional self-training group completed 5 wk of self-training. Two participants from the video game self-training group discontinued training for personal reasons after 2 and 3 wk, respectively. Two participants from the traditional self-training group stopped training after 2 and 3 wk (because of boredom with the intervention and unwillingness to continue). During the 4-wk follow-up period, 8 of 11 participants (72.7%) in the video game group continued to play video games, and only 4 of 9 participants (44.4%) in the traditional group continued to perform the traditional self-training intervention.
The following descriptive analysis of the training time includes 11 participants from the video game and 9 participants from the traditional self-training groups who completed the 5-wk training. The participants in the video game group played a mean 3.7 hr/wk (SD = 1.6, range = 1.3–6; M total training time for the 5-wk intervention = 18.8, SD = 8.0). Participants in the traditional group performed a mean 6.8 weekly training hours (SD = 5.4, range = 1.9–6.6; M = 27.4 total training hours for the 5-wk intervention, SD = 5.6) . This difference was statistically significant, t(18) = −2.7, p = .014. Table 2 presents the mean daily training time, perceived enjoyment, and perceived exertion of each of the participants in the video game and traditional self-training interventions for each of the 5 wk.
Adherence to and Satisfaction With the Video Game 5-Week Self-Training Intervention
Note. UE = upper extremity.
Participant played the video games seated.
Participant did not come to the postintervention assessment and fill in the satisfaction questionnaire.
Satisfaction
The perceived enjoyment of the participants in the video game group was slightly higher than but not significantly different from that of the participants in the traditional group, t(18) = 1.1, p = .26. Participants in the video game self-training group reported enjoying it very much (M = 4.1, SD = 0.84, out of a maximum of 5 points), and participants in the traditional self-training group reported enjoying it “quite” to “very much” (M = 3.7, SD = 0.75). Exertion was perceived to be light and similar for both groups (Ms = 11.8 and 11.4, SDs = 2.7 and 2.7, respectively, out of a maximum 20 points), t(22) = 0.2, p = .7. Figure 2 presents the mean daily self-training time, enjoyment, and exertion for each of the 5 wk.
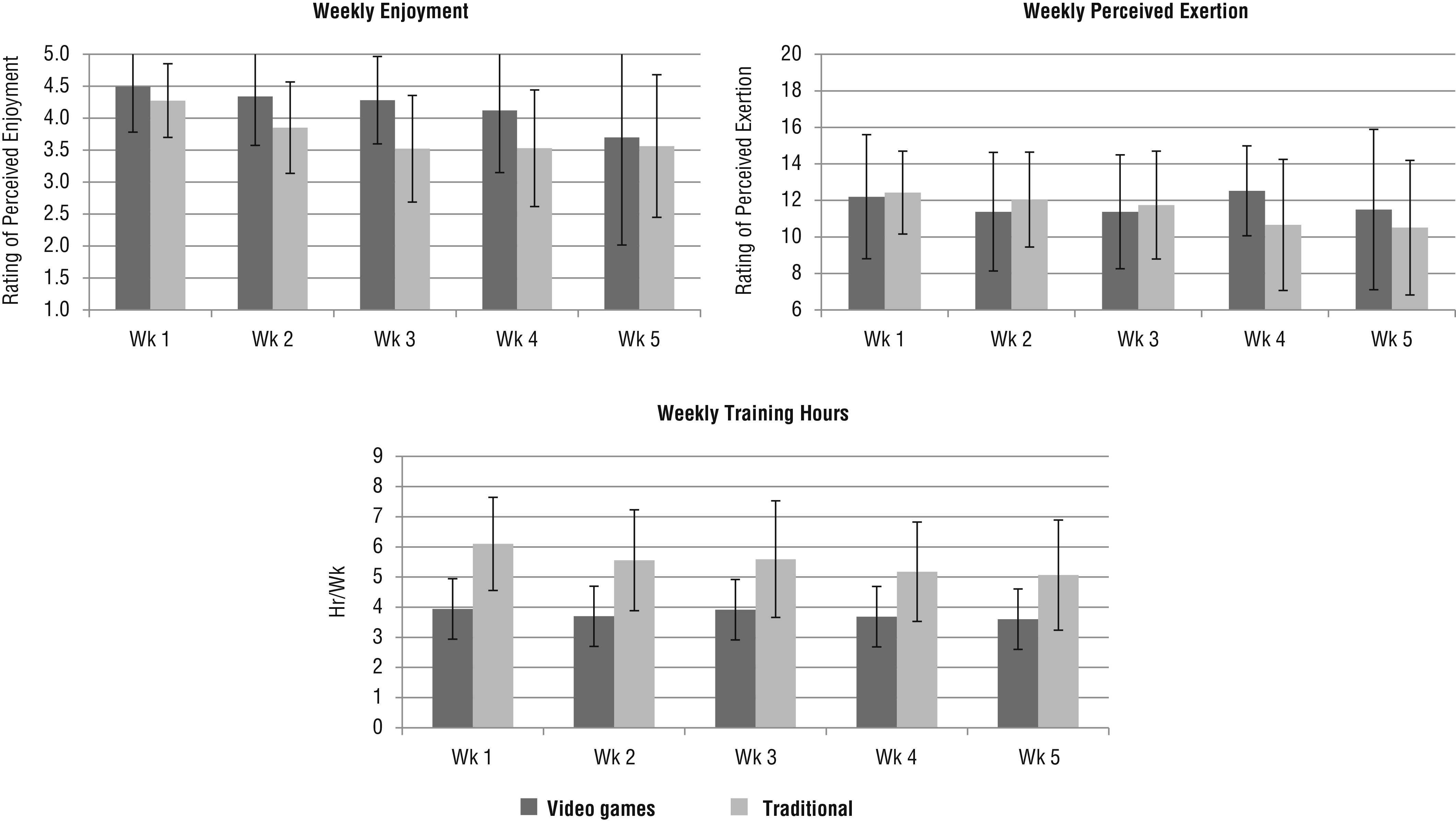
Mean (standard deviation) weekly enjoyment, exertion, and time (hr) for the self-training from Wk 1 to Wk 5 for the 11 participants in the video game group (dark gray) and the 9 participants in the traditional group (light gray).
Satisfaction with both programs was moderate to relatively high and not significantly different, t(22) = 0.59, p = .5 (M = 3.9, SD = 1.0, for the video game group, and M = 3.6, SD = 0.7, for the traditional group, out of 5 points). Four participants (30%) in the video game self-training group were extremely satisfied (rating of 5 out of 5), but none of the participants in the traditional self-training group rated their satisfaction as 5. Five (38%) of 13 participants from the video game group and 7 (63%) of 11 participants from the traditional training group reported perceived functional improvement of their weaker UE. More video game participants (n = 9; 69%) than traditional training participants (n = 3; 27%) reported perceiving some or substantial balance improvement. Eight (61%) of 13 participants from the video game intervention and 6 (54%) of 11 participants from the traditional group reported needing “very little” assistance from their family to perform the self-training.
Discussion
This pilot study demonstrates the feasibility, satisfaction, and compliance with two UE self-training programs for people with chronic stroke. The GRASP traditional self-training program, which has previously been demonstrated to be feasible and effective (Adie et al., 2017; Harris et al., 2009), was successfully used by our participants with chronic stroke. Our study assessed additional factors, such as satisfaction and perceived benefit of this program, that have not previously been reported.
In the video game group, participants managed to independently operate, follow, and carry out the self-training in their homes. Home-based use of commercial video games without the supervision of a therapist—specifically, the Wii—has been reported to improve the balance of people with multiple sclerosis (Prosperini et al., 2013) and has recently been used in UE training for people with subacute stroke (Adie et al., 2017) who were seated. This study is novel because different video game consoles were used, and participants were encouraged to play while standing. Standing while playing active video games encourages whole-body movement, not only UE movement, which can also lead to improved postural control (McCombe Waller & Prettyman, 2012).
Standing while playing was implemented with only 10 of 13 participants, despite the careful selection of the participants into the study. Perceived improved balance after the intervention was reported by 9 of these 10 participants. Weight transfer and trunk and body stabilization, performed spontaneously while playing, may possibly have improved their balance, as reported in other studies (Vorderer et al., 2003). This study was unique, however, because there was no physical support or therapist supervision. Despite this fact, falls were not reported, which may be explained by the participant selection, the careful set up of the playing environment, and the clinical reasoning regarding whether the participants could stand while playing.
An additional 30 min per day of UE self-training has been shown to be sufficient to improve the UE functional ability of people with subacute stroke (Adie et al., 2017; Harris et al., 2009). Participants from both groups achieved this daily training time, which also led to improvement in their UE functional and daily use (Rand et al., 2017). Participants from the traditional group performed significantly longer daily self-training sessions than those in the video game group. This was surprising because video games are considered to be fun and motivating (Coupar et al., 2012; Givon et al., 2016; Lohse et al., 2013; Schoene et al., 2013), which we thought would lead to longer training time. The longer training time for the traditional group might be the result of the very structured GRASP. Participants received the illustrated GRASP manual, which specifies the exercises and number of repetitions per exercise. Participants were requested to perform self-training for 1 hr, but we later discovered that they performed all of the exercises in the manual in each session, even if it took longer. This structure was difficult to attain in the video game group because of the games’ varying playing times (better performance in a game allows longer playing time, and vice versa). Therefore, participants were requested to play three to four specific games but could not be instructed to play each game a specific number of times. This possibly led to their finishing the training in less time. Nevertheless, less training time has been reported for other programs using technology for home-based training despite the fact that those participants were followed up very closely by a therapist. For example, 24 participants performed a mean of 1.75 hr (SD = 1.1, range = 0.2–4.7) per week using a technology-supported training system that encouraged proximal and distal movements in playing three games (Nijenhuis et al., 2015) while supervised remotely by a health care professional who visited them once a week. The need to don and doff the orthosis and the requirement to calibrate the system might explain this result. Compared with telerehabilitation programs (Vorderer et al., 2003), in which the practice time is fixed and scheduled ahead of time, participants in this study had the flexibility to perform the self-training at times that were convenient for them.
Although it could be expected that older stroke participants would encounter more difficulties using tech devices, participants using video games did not require more family assistance or support, and they felt that the amount of preprogram training was sufficient, similar to the participants who received traditional self-training. Technical problems were uncommon and were easily overcome with the therapists’ support. After the consoles were connected to the television, the participants could easily operate the games to perform their daily training. These findings are similar to those with 114 participants who played Wii games for 4 wk (Adie et al., 2017).
Video games are known to enhance motivation and fun because of their competitive nature, use of music and graphics, and scoring (Coupar et al., 2012; Givon et al., 2016; Lohse et al., 2013; Schoene et al., 2013). More participants in the video game self-training reported extreme enjoyment of the self-training than in the traditional group, in which 1 participant reported stopping training because of boredom, and another continued the self-training despite reporting that the exercises were boring and not challenging. The enjoyment from playing the video games for 5 wk is similar to the enjoyment rated after playing different video games in a one-time session (Rand et al., 2008). Enjoyment, which is a key factor to ensuring ongoing participation in exercise programs (Givon et al., 2016; Schoene et al., 2013), possibly led to a higher percentage of participants continuing to play the video games compared with performing the traditional exercises during the 4-wk follow-up period.
Two participants asked to keep the console after this period, and 2 additional participants said they would like to purchase it. Some participants reported playing the games with their grandchildren and children who came to visit, which did not occur in the traditional self-training group. This aspect of the study highlights the potential of using video games to increase compliance with maintaining ongoing activity.
The video games, which have been identified to facilitate more and faster purposeful UE movements (Rand et al., 2014) and were played by most of the participants while standing, require whole-body movements. The participants who played video games reported similar levels of light exertion but for less training time than participants who performed traditional self-training, which was performed seated. It is interesting to see that even after 3 or 4 wk of training, the video games provided participants with a stimulating environment for training. Further research should compare perceived exertion after training sessions of similar duration; perhaps longer training time playing video games will increase the level of exertion a bit to 13 (somewhat hard), which is the recommended level for exercising (Gordon et al., 2004).
Study limitations include the small sample size and short duration of intervention and follow-up. An additional limitation might be that training time was self-reported. However, because family members and therapists were closely involved, we trust that the data are accurate. The study population was high functioning and cognitively intact; therefore, these findings might not generalize to people with lower functioning.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Using commercial video game consoles for daily training of upper extremity and body movements is feasible and enjoyable and has potential to maintain long-term activity.
Participants with chronic stroke demonstrated high adherence to and satisfaction with both self-training programs to train their weaker upper extremity; therefore, occupational therapy practitioners should offer participants a self-training program to continue practicing upper extremity movements at the chronic stage poststroke.
Conclusion
To conclude, this pilot study demonstrated the feasibility of, adherence to, and high satisfaction with two UE self-training programs that required minimal family assistance. Commercial video games not specifically developed for rehabilitation can be successfully used (in standing) by people with chronic stroke. More participants continued to play video games after the intervention, indicating its potential to provide a sustainable solution for maintaining ongoing activity. Future research should provide much longer duration of self-training and follow-up on adherence and benefits.
Supplemental Material
Supplementary material for Feasibility of, Adherence to, and Satisfaction With Video Game Versus Traditional Self-Training of the Upper Extremity in People With Chronic Stroke: A Pilot Randomized Controlled Trial
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.026799.pdf for Feasibility of, Adherence to, and Satisfaction With Video Game Versus Traditional Self-Training of the Upper Extremity in People With Chronic Stroke: A Pilot Randomized Controlled Trial by Anat Yacoby, Gabi Zeilig, Harold Weingarden, Ronit Weiss and Debbie Rand in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors thank all the participants. This work was performed in partial fulfillment of the requirements for a Master of Occupational Therapy degree by Anat Yacoby and Ronit Weiss, Sackler Faculty of Medicine, Tel Aviv University, Israel. Debbie Rand was funded by the European Community’s Seventh Framework Program (FP7/2007–2013) under Grant Agreement 277023, Virtual Reality Intervention for Stroke Rehabilitation. This study was registered with ![]() (NCT02393170).
(NCT02393170).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.