
Abstract
Improving health conditions and work performance among employees is a global objective in occupational health (World Health Organization, 2007). Occupational health has been defined as a field aimed at maintaining and promoting the physical, mental, and social well-being of workers in all areas (Kopias, 2001). Conflict is a risk factor for occupational health and is being studied around the world (e.g., Arenas et al., 2015). Conflict is recognized as one cause of stress and burnout, and these problems are also global issues (e.g., Salvagioni et al., 2017). Conflict is defined as an interactive process manifested in incompatibility, disagreement, and dissonance within or between social interactions (Baron, 1990; Rahim, 2015). The conflict involves belief; therefore, in areas such as philosophy and health care, this problem is called belief conflict (e.g., Husserl, 1970; Kyougoku et al., 2015; Saijo, 2005; Takeda, 2004).
In recent years, belief conflict and occupational dysfunction have attracted attention as occupational health-related problems in Japan (Kyougoku et al., 2015; Teraoka & Kyougoku, 2015c). Belief conflict arises in the course of teamwork, and occupational therapy practitioners therefore encounter this problem because they work in teams (Kohiyama & Kyougoku, 2016). Occupational dysfunction is a health problem experienced by Japanese workers, and its prevalence is particularly high among health care workers (Teraoka & Kyougoku, 2015c). Both belief conflict and occupational dysfunction have been linked to job stress, depression, and burnout (Kyougoku et al., 2015; Teraoka & Kyougoku, 2015a).
In other words, belief conflict and occupational dysfunction are associated with various outcomes that are globally recognized as serious issues in occupational health. Therefore, preventive occupational therapy should attempt to improve both belief conflict and occupational dysfunction (Teraoka & Kyougoku, 2014).
Review of Belief Conflict
Belief is a view of the world constructed through the interaction of the person and the environment (Kyougoku, 2011). Belief conflict is a fundamental confrontation caused by situations that challenge or bring individuals’ beliefs into question (Kyougoku, 2011). This phenomenon was first proposed through an examination of Husserl’s phenomenology (Takeda, 2004), a philosophy that clarifies the conditions under which a belief is established (Husserl, 1970). In Japan, Husserl’s phenomenology was later incorporated into a philosophical movement called “structural constructivism” (Saijo, 2005).
The aim of structural constructivism was to dissolve belief conflict in the human sciences (Saijo, 2005).The dissolution approach for belief conflict (DAB), which was based on structural constructivism, aimed to decrease belief conflict in the health care field (Kyougoku, 2011). In DAB, belief conflict arises when an individual’s thoughts, emotions, or actions are not approved by another person or a group (Kyougoku, 2011). DAB has been applied in various fields such as interprofessional practice and education, medical care, nursing, physical therapy, occupational therapy, and artificial intelligence (Kyougoku, 2012, 2014; Matsuda & Kyougoku, 2015). Belief conflict negatively affects teamwork, shared decision making, therapeutic relationships, and occupation-based practice and leads to job stress and burnout (Kohiyama & Kyougoku, 2016; Kono & Kyougoku, 2015; Kyougoku, 2012; Kyougoku & Teraoka, 2015; Kyougoku et al., 2015; Simizu, 2013, 2015; Yonemoto & Kyougoku, 2015).
Review of Occupational Dysfunction
Occupational dysfunction was originally proposed as a concept in the Model of Human Occupation (MOHO) and was later adopted in the occupational sciences (Kielhofner, 1995, 1997; Wilcock, 1998). In MOHO, occupational dysfunction occurs when a person has difficulty choosing, interpreting, performing, or experiencing his or her occupations, which includes work, play, daily life, and rest (Kielhofner, 1995). Occupational dysfunction becomes a problem when occupations fail to provide health and well-being or cannot meet the needs of the interaction between the person and environment (Kielhofner, 1995, 1997).
Subclassification of this field began when the concept was transferred from MOHO to occupational science (Kielhofner, 1997; Molineux, 2004; Wilcock, 1998). For example, Molineux (2004) classified occupational dysfunction into five categories (occupational deprivation, occupational disruption, occupational alienation, occupational imbalance, and performance deficits), whereas Wilcock (1998) divided it into three categories (occupational imbalance, occupational deprivation, and occupational alienation). Therefore, because no unified view regarding the classification of occupational dysfunction exists, our research group conducted a concept analysis to further elucidate its structure (Teraoka & Kyougoku, 2014).
Confirmatory factor analysis revealed a four-factor structure of occupational dysfunction consisting of occupational imbalance, occupational deprivation, occupational alienation, and occupational marginalization (Teraoka & Kyougoku, 2015a, 2015b). In addition, we developed a new theory of occupational therapy called Occupation-Based Practice 2.0 (OBP 2.0), which divides occupational dysfunction into four categories (Teraoka & Kyougoku, 2014). OBP 2.0 was developed theoretically by drawing on a variety of literature related to occupational therapy (e.g., Kielhofner, 1995; Kyougoku, 2011; Wilcock, 1998). OBP 2.0 addresses both belief conflict and occupational dysfunction, facilitating the relationship between clients and their families, and it plays a role in improving occupational dysfunction (Tanaka et al., 2016).
In OBP 2.0, occupation is defined as a human experience (Teraoka & Kyougoku, 2014). Moreover, occupational dysfunction is a state in which an occupation cannot be appropriately engaged in or enabled (Teraoka & Kyougoku, 2014). Occupational imbalance is a state in which the meaning, time, and type of balance regarding occupation is biased. Occupational deprivation is a state in which occupation cannot be enabled or engaged in appropriately because of external factors. Occupational alienation is a state in which meaning cannot be felt in occupation. Finally, occupational marginalization is a state in which occupation cannot be enabled or engaged in appropriately because of the gap between people’s choices about occupations and social expectations. Like belief conflict, occupational dysfunction may negatively affect occupational participation and health-related quality of life and lead to stress, depression, and burnout in health care workers (Teraoka, 2015; Teraoka & Kyougoku, 2015a, 2015b).
Research Objective
As described earlier, belief conflict and occupational dysfunction should be considered as health issues among health care workers. However, to our knowledge, no studies have examined the relationship between belief conflict and occupational dysfunction. Therefore, the purpose of this research was to examine this relationship.
Method
Ethical Approval
This research was approved by the Kibi International University Research Ethics Review Committee (No. 13–01).
Research Design
This study followed a cross-sectional study design and used a questionnaire. To improve the accuracy of the answers, we first explained the concepts of belief conflict and occupational dysfunction to participants. In addition, participants read a briefing paper on both concepts to deepen their understanding.
Participants
Participants were recruited via nonrandom sampling in Japan. Inclusion criteria required participants to be practitioners employed in hospitals, including doctors, nurses, and occupational therapists.
Measures
Participant Profile.
Basic information was obtained from participants, including age, gender, license, years of clinical experience, work time, commute time, marital status, smoking habits, and alcohol consumption habits.
Assessment of Belief Conflict in Relationship–14.
We measured belief conflict using the Assessment of Belief Conflict in Relationship–14 (ABCR–14), which is based on the DAB (Kyougoku et al., 2015). The ABCR–14 contains 14 items across three factors, with a 7-point response scale ranging from 1 (disagree) to 7 (agree; Kyougoku et al., 2015). The three factors include belief conflict within the same health care profession, belief conflict between health care workers and staff in other professions, and belief conflict between the client and health care professional. When the total score of the ABCR–14 is high, it is interpreted as belief conflict. However, because the cutoff value of the ABCR–14 is unknown, no criterion for interpretation currently exists.
Classification and Assessment of Occupational Dysfunction.
We measured occupational dysfunction using the Classification and Assessment of Occupational Dysfunction (CAOD), which is based on the OBP 2.0 (Teraoka & Kyougoku, 2015b). The CAOD contains 16 items across four factors with a 7-point response scale ranging from 1 (disagree) to 7 (agree; Teraoka & Kyougoku, 2015b, 2015c). The four factors include occupational imbalance, occupational deprivation, occupational alienation, and occupational marginalization. The cutoff value of ≥52 points indicates a higher risk for occupational dysfunction. The cutoff value of CAOD has been obtained on the basis of the Japanese version of the Center for Epidemiologic Studies Depression Scale (Radloff, 1977).
Data Analysis
Statistical Software.
In this study, we conducted analyses using Stan (Version 2.11; NumFOCUS, Austin, TX) and DPpackage (Version 1.1-7.4; Jara et al., 2011) in R (Version 3.3.1; R Foundation, Vienna, Austria). Stan software is used for Bayesian statistical modeling through the Hamiltonian Monte Carlo method (Kruschke, 2014), and DPpackage software is used for Bayesian nonparametric and semiparametric modeling in R (Jara et al., 2011). Stan was used for descriptive statistics, estimation of differences, correlation analysis, and estimation of odds ratios. DPpackage was used to estimate the cutoff value.
Bayesian Analysis.
In this study, Bayesian statistics modeling was used to calculate descriptive statistics, estimate differences, analyze correlations, determine the cutoff value, and estimate odds ratios. Bayesian statistics modeling shows the result by expected a posteriori (EAP) and 95% credible interval, which is the estimated value of the posterior distribution. EAP is the mean of the posterior distribution. The 95% credible interval is an interval estimation of a posterior distribution. Moreover, the 95% credible interval can be interpreted as having a significant difference when zero is not included. A concept similar to the 95% credible interval is the 95% confidence interval, which means that if 100 different samples of the same population were taken and a 95% confidence interval was computed for each sample, then approximately 95 of the 100 confidence intervals would contain the true mean value (Kruschke, 2014). Conventional statistics refer to 95% confidence intervals, but Bayesian analysis refers to 95% credible intervals (Kruschke, 2014).
In this study, we used Bayesian description statistics to estimate total results and results separated by gender; we also examined Bayesian differences by gender. Bayesian correlation analysis was used to determine the correlation between the sum of ABCR–14 plus CAOD and factor scores. The following values were used to understand the size of the correlations: r = 0–.20, decorrelation; .20–.40, small correlation; .40–.60, moderate correlation; .60–.80, large correlation; and .80–1.00, very large correlation (Tomita, 2006). We calculated the predictive accuracy of the ABCR–14 using the CAOD diagnosis of occupational dysfunction as the external criterion assessment of belief conflict, on the basis of the Bayesian semiparametric model. A receiver operating characteristic (ROC) curve was used to determine the cutoff value. The accuracy of the ROC curve was judged by the area under the curve (AUC). The following values were used to interpret the accuracy of the AUC: .5–.7, low accuracy; .7–.9, moderate accuracy; and .9–1.0, high accuracy (Streiner & Cairney, 2007).
Generally, for disorders such as depression, a physician’s diagnosis is used as an external criterion for determining the cutoff value of the assessment scale. However, no diagnostic criterion for belief conflict exists, so expert judgment cannot be used as an external standard. Therefore, in this study, we adopted CAOD, which measures occupational dysfunction that is expected to be related to belief conflict as an external standard. We predicted that the hypothesis indicating that participants with occupational dysfunction would experience belief conflict would hold. Participants with values greater than the ABCR–14 cutoff value were categorized as the “belief conflict group with occupational dysfunction” (high-belief-conflict group), and those with values less than the ABCR–14 cutoff value were categorized as the “belief conflict group without occupational dysfunction” (low-belief-conflict group). Moreover, we investigated how many odds ratios of occupational dysfunction and demographic variables would increase if belief conflict was present.
The predictor variable was ABCR–14, and the response variables were CAOD gender, age, clinical experience, work time, commute time, smoking, and drinking. The cutoff value of the CAOD was used to indicate the presence of occupational dysfunction. We estimated medians for the following variables: age, clinical experience, work time, and commute time. These variables were also used for the creation of dummy variables. In the prediction model, we also estimated the correct probability of the hypothesis that the odds ratio would exceed 1. Half-Cauchy distribution (which is less likely to influence posterior distribution, and its use has been recommended; Gelman, 2006; Gelman et al., 2016) was used as the prior distribution. Repeating the simulation numerous times will lead to similar results. The appropriateness of the posterior distribution was judged when the Rhat value was ≤1.05. Therefore, a posterior distribution was generated as a predictive distribution that approximated a true distribution. In this study, we generated four Markov chains, repeated all simulations 10,000 times, and discarded half.
Results
Bayesian statistical modeling revealed that Rhat values were ≤1.05 for all possible comparisons. In other words, the posterior distribution generation was properly conducted for Cauchy distribution.
Demographic Characteristics
A total of 890 practitioners participated in the study (449 women, 441 men; Table 1). A difference in posterior probability distribution was present between men and women in age, ABCR–14 scores (excluding one factor), and CAOD scores.
Demographic Characteristics
Note. ABCR–14 = Assessment of Belief Conflict in Relationship–14; BC-F1 = belief conflict within the same health care profession; BC-F2 = belief conflict between health care workers and staff in other professions; BC-F3 = belief conflict between the client and health care professional; BTGD = Bayesian testing of gender difference; CAOD = Classification and Assessment of Occupational Dysfunction; CI = credible interval; EAP = expected a posteriori; M = mean; OD-F1 = occupational imbalance; OD-F2 = occupational deprivation; OD-F3 = occupational alienation; OD-F4 = occupational marginalization; SD = standard deviation.
Bayesian Estimation of Correlation
Correlations between ABCR–14 and CAOD factors were moderate to strong (Table 2).
Correlations
Note. ABCR–14 = Assessment of Belief Conflict in Relationship–14; BC = ABCR–14 total score; BC-F1 = belief conflict within the same health care profession; BC-F2 = belief conflict between health care workers and staff in other professions; BC-F3 = belief conflict between the client and health care professional; CAOD = Classification and Assessment of Occupational Dysfunction; CI = credible interval; EAP = expected a posteriori; OD = CAOD total score; OD-F1 = occupational imbalance; OD-F2 = occupational deprivation; OD-F3 = occupational alienation; OD-F4 = occupational marginalization.
Bayesian Estimation of the Cutoff Value
The cutoff value for the ABCR–14 was 58 points (sensitivity = .80, specificity = .76, AUC = .87; Figure 1). The AUC value of .87 can be interpreted as moderate accuracy. In other words, participants with a total score on the ABCR–14 of ≥58 were placed into the high-belief-conflict group, indicating an increased risk of experiencing occupational dysfunction.
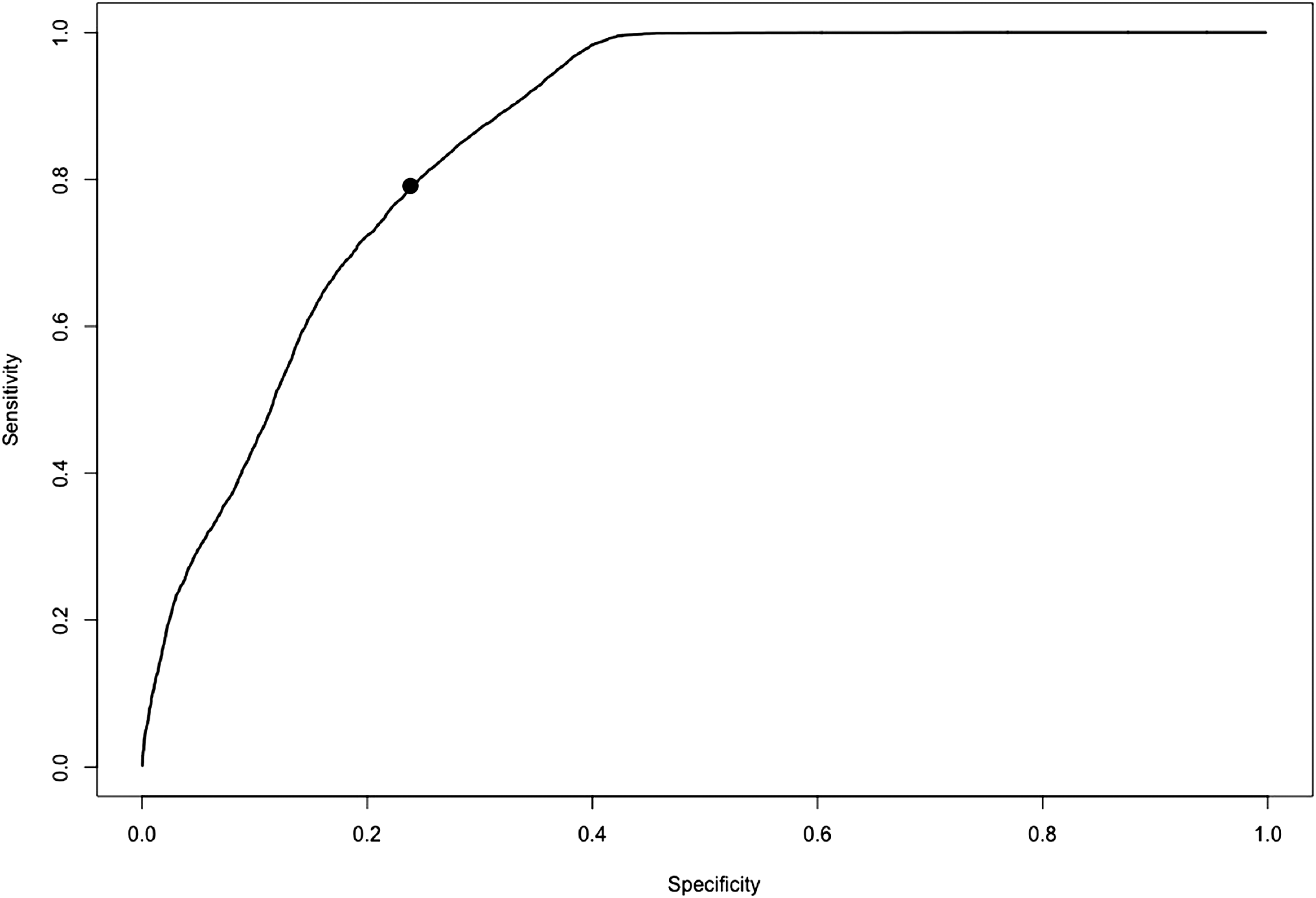
Receiver operating characteristic curve.
Bayesian Estimation of the Odds Ratio
Odds ratios are displayed in Table 3. Occupational dysfunction variables all had a high odds ratio, and the hypothesis showed 100% correct probability.
Odds Ratios
Note. CI = credible interval; EAP = expected a posteriori; OR ≥ 1 = probability that the odds ratio is ≥1.
Discussion
This study had five main findings. First, belief conflict and occupational dysfunction showed a moderate to strong positive correlation. In previous research, the ABCR–14 was used to measure problems in teamwork in health care fields (Kyougoku et al., 2015), and occupational dysfunction was previously found to be a problem among health care workers (Teraoka & Kyougoku, 2015c). The findings of this study indicate that issues related to teamwork and health are interrelated.
Second, the cutoff value of the ABCR–14 was estimated to be 58 points or higher when it was based on the CAOD. In other words, a participant who has an ABCR–14 total score of 58 or higher could be classified as being in the high-belief-conflict group. Occupational dysfunction is a health issue that leads to job stress and depression (Teraoka & Kyougoku, 2015c). Therefore, researchers and practitioners need to pay attention to the relationships and health of high-belief-conflict groups.
Third, gender differences were found in the relationship between the ABCR–14 and CAOD. Gender differences were hardly observed in other profiles, but men scored highly in the ABCR–14 and CAOD (except for one factor in the ABCR–14). Moreover, the odds ratios for the high-belief-conflict group and the occupational dysfunction group were greater among women. Although previous studies have not found a gender difference, the results of this study suggest this possibility (Kyougoku et al., 2015; Teraoka & Kyougoku, 2015c).
Fourth, all men’s scores had odds ratios exceeding 1. On the basis of this finding, we think that men in the high-belief-conflict group need to take measures against aging, long work hours, long commuting time, and the consequences of drinking and smoking as well as occupational dysfunction. In particular, drinking and smoking contribute to an increase in lifestyle diseases and cancer, so it may be necessary to investigate the relationship between high-belief-conflict groups and these behaviors in the future.
Finally, Bayesian analysis might promote preventive occupational therapy studies. For example, the conventional odds ratio represents the response rate to the presence or absence of exposure only. In contrast, the odds ratio in Bayesian analysis estimates the probability that the odds ratio exceeds 1 in addition to the response rate. Because the results obtained by Bayesian analysis are intuitive and easily understood, this analytical approach will be useful for research in preventive occupational therapy.
Limitations and Future Studies
Because this study was cross-sectional, a strict causal relationship could not be determined. Longitudinal studies are needed in the future to investigate effects over time.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
This study provides evidence that belief conflict and occupational dysfunction show a more than moderate correlation. Moreover, compared with women, considerably more men had these problems.
In this study, the odds ratios for occupational dysfunction were high in the high-belief-conflict group, especially among women, showing that women are at increased risk.
Conclusion
Belief conflict and occupational dysfunction are global problems. Therefore, in this study, we examined the relationship between belief conflict and occupational dysfunction. Results indicated that belief conflict and occupational dysfunction were moderately to strongly positively associated. Belief conflict and occupational dysfunction showed a strong correlation in men. Moreover, it was found that more clinical experience, long working time, long commuting time, drinking, and smoking tended to be problematic among men in the high-belief-conflict group.