
Abstract
Despite many health benefits of physical activity for people with spinal cord injury (SCI; Cragg et al., 2012; Ginis et al., 2011), people with SCI are extremely inactive. Only 13%–16% report consistent physical activity (Fernhall et al., 2008; Washburn & Hedrick, 1997), whereas the majority report no physical activity (Perrier & Martin Ginis, 2016; Tasiemski et al., 2000). Numerous barriers to increasing physical activity in people with SCI exist, such as mobility limitations and a lack of accessible physical activities (Vissers et al., 2008). Thus, incorporating physical activity into a person’s everyday life should be a main strategy for occupational therapy practitioners to increase overall physical activity in people with SCI. However, to intervene with this population, an understanding of physical activity levels in daily life and how people function in their environment is needed.
Physical activity in daily life is commonly measured objectively by accelerometers. Although this method is valid and reliable in ambulatory people with or without neurological conditions (Dijkstra et al., 2008; Hendelman et al., 2000; Motl et al., 2006; van Someren, 1997; Weikert et al., 2010), less is known about measurement properties of accelerometers in people with SCI. In the SCI literature, researchers have examined the validity of accelerometry methods to detect wheelchair movement (Sonenblum et al., 2012), predict energy expenditure (Hiremath & Ding, 2011; Hiremath et al., 2013; Nightingale et al., 2014; Tanhoffer et al., 2012), or discriminate between different types of ambulation (such as self-propelled wheeling vs. being pushed; Kooijmans et al., 2014). Although these types of studies provide crucial information about mobility-related physical activity, the focus is generally on wheelchair usage and is limited in terms of other types of physical activity.
Some accelerometers allow for simultaneous measurement of physical activity as well as symptoms and behaviors that occur in real time. This type of technology offers the potential for insights about how people function within their daily context and into immediate barriers to engaging in physical activity. Two such monitors currently available are the Actiwatch Score (Philips Respironics, Bend, OR) and PRO-Diary (CamNTech, Cambridge, England). These wrist-worn monitors can be programmed to alert participants to enter self-report responses about pain, fatigue, social context, and other factors that are relevant to physical activity engagement. Actiwatch Score allows for responses to be entered on a numerical rating scale and has demonstrated good criterion validity and reliability for measuring physical activity in independent ambulatory participants (Gironda et al., 2007; Kop et al., 2005; Murphy et al., 2008). PRO-Diary offers more options for gathering self-report data, including free text, Likert scales, and branching logic.
In a focus group conducted by Kratz (2004), people with SCI were able to more easily enter responses into PRO-Diary compared with Actiwatch Score. However, little is known about the reliability and validity of PRO-Diary. One study showed that PRO-Diary corresponded to a gold-standard accelerometer in measuring sedentary to vigorous activity in independent ambulatory participants (Hickey et al., 2016). No studies to date have examined how either Actiwatch Score or PRO-Diary performs in measuring everyday activity in people who use a manual wheelchair.
In this study, we examined the reliability and construct validity of Actiwatch Score and PRO-Diary in people with SCI (who were manual wheelchair users) or without SCI in laboratory tasks designed to simulate a range of everyday physical activities. The first aim was to examine the interunit reliability, or agreement, of Actiwatch Score and PRO-Diary within each group across tasks. We expected high interunit reliability in both groups across all tasks. The second aim was to examine the construct validity of Actiwatch Score and PRO-Diary within each group by examining sensitivity of the monitors to different activity levels across tasks. We expected that both monitors would be sensitive to activity-level differences between tasks. Because ambulation is more dependent on upper extremity mobility for those in a wheelchair compared with those who ambulate by walking, it was hypothesized that both monitors would show significantly higher physical activity counts for the two ambulation tasks, but not other tasks, in the SCI group compared with the non-SCI group.
Method
This research was approved by the University of Michigan’s (UM’s) Human Subject Review Board. Volunteers with SCI were recruited through existing participant registries and were sex and age matched (within 2 yr) to participants without SCI, who were recruited through a UM-sponsored research participant website.
Eligibility screening was done by phone. Inclusion criteria were ages 18–65 yr and English speaking. Those without SCI had to ambulate independently without an assistive device. For participants with SCI, additional inclusion criteria were ≥1 yr since injury and use of self-propelled manual wheelchair. Exclusion criteria were medical condition that interferes with typical physical activity or ability to complete study tasks, including limb amputation, acute injury or illness, severe arthritis, or other orthopedic condition; uncontrolled cardiovascular or metabolic disease; and any injury or condition that affects upper extremity strength or dexterity.
Participants who met eligibility criteria were scheduled for a lab visit. After providing written consent, participants completed a demographic questionnaire and self-reported height and weight (because of lack of a wheelchair-accessible scale). Waist circumference (in centimeters) was measured by the research assistant.
Instruments
Actiwatch Score.
Actiwatch Score is an accelerometer that has a cantilevered rectangular piezoelectric bimorph plate and measures seismic mass sensitive to movement in all directions. This type of sensor integrates the degree and speed of motion and produces an electrical current that varies in magnitude. Increases in degree and speed of motion produce an increase in voltage, and these raw data were processed by onboard software into activity counts. The monitors were programmed to record data in 15-s epochs for maximum sensitivity. Data were calculated to yield average activity counts per minute. Each Actiwatch Score was randomly selected from a pool of monitors (N = 35).
PRO-Diary.
PRO-Diary has an integrated triaxial microelectromechanical systems accelerometer. Raw acceleration measurements were processed with onboard software to generate activity counts; the maximum sampling frequency is 50 Hz subjected to bandwidth filtering (3–11 Hz) with a range between 0.01 and 8 g. PRO-Diary was programmed to record data in 15-s epochs to be consistent with the maximum sensitivity setting of Actiwatch Score. Data were calculated to yield average activity counts per minute. Each PRO-Diary was randomly selected from a pool of monitors (N = 12).
Testing Protocol
The protocol involved a 90-min lab visit. Data were collected by one of three trained research assistants. The same laptop was used to initialize and download data from the two monitors to ensure time synchronization. A solid plastic unit on which the two monitors were mounted was secured to the dorsal aspect of the nondominant wrist above the ulnar process with a hook-and-loop wristband.
Participants completed a series of tasks, described in Table 1. Participants were instructed to perform each activity at a self-selected pace, similar to the pace in which usual activities at home are performed, with the exception of brisk walking–wheeling. At the start and end of each activity and rest period, the participant pushed the Actiwatch Score button as an event marker to delineate the tasks for data processing. Start and end times were also recorded by the research assistant. Participation in the study ended after the testing protocol was completed.
Series of Tasks in Testing Protocol
Data Analysis
Bland–Altman plots, a widely used tool to compare two similar measurement methods, were used to measure agreement (Bland & Altman, 1986). Bland–Altman plots graphically display mean differences between two methods, and lines that represent confidence intervals are superimposed; scaling differences are reflected in bias lines depicted on the graphs (Giavarina, 2015). The data for video watching and Internet browsing were natural log-transformed before conducting t tests and Bland–Altman plots to correct for substantially nonnormal distributions. Intraclass correlation coefficients (ICCs) with an absolute agreement definition and a two-way random effect model were also used to examine interunit agreement within each task for the groups.
To test construct validity, we first examined whether Actiwatch Score and PRO-Diary were sensitive to detecting changes in physical activity, as indicated by average activity counts per minute, from one task to the next. Raw mean differences (subsequent task activity count − previous task activity count) and percentage difference (from the previous activity count) were calculated. We then conducted paired t tests to compare average activity counts per minute from one task to another for each monitor within each group. Good construct validity was indicated when the monitors were able to detect notable differences in physical activity between tasks. Between SCI and non-SCI groups, we examined whether the monitors would detect different physical activity levels by task using independent sample t tests. Construct validity was supported if the monitors showed notable differences on tasks expected to be different between groups (i.e., the walking–wheeling tasks). We conducted statistical analyses using IBM SPSS Statistics (Version 22; IBM Corp., Armonk, NY).
Results
Thirty-eight participants (19 with SCI and 19 without SCI) participated in the study. The participants had a mean age of 49 yr, and one-third were female; the group was predominantly White and, on average, overweight. The groups were similar except that participants without SCI tended to hold more advanced educational degrees. In the SCI group, about half had complete injuries, and the majority had injuries that occurred ≥7 yr ago.
Interunit Reliability (Agreement)
Bland–Altman plots (Figure 1) showed agreement between Actiwatch Score and PRO-Diary in each task. Agreement between monitors was acceptable for almost all tasks, indicated by data points mostly clustered around the bias line, with few points scattered beyond the limits of agreement. The brisk walking–wheeling task had the most data points outside the limits of agreement. Relatedly, both walking–wheeling tasks showed evidence of systematic error as a result of increasing differences between the monitors as physical activity level increased. ICC values depicted in Table 2 ranged from .78 to .97, indicating a high level of agreement between monitors for all tasks within each group. The ICCs were high when we combined the two groups together and compared across the tasks (all ICCs > .90).
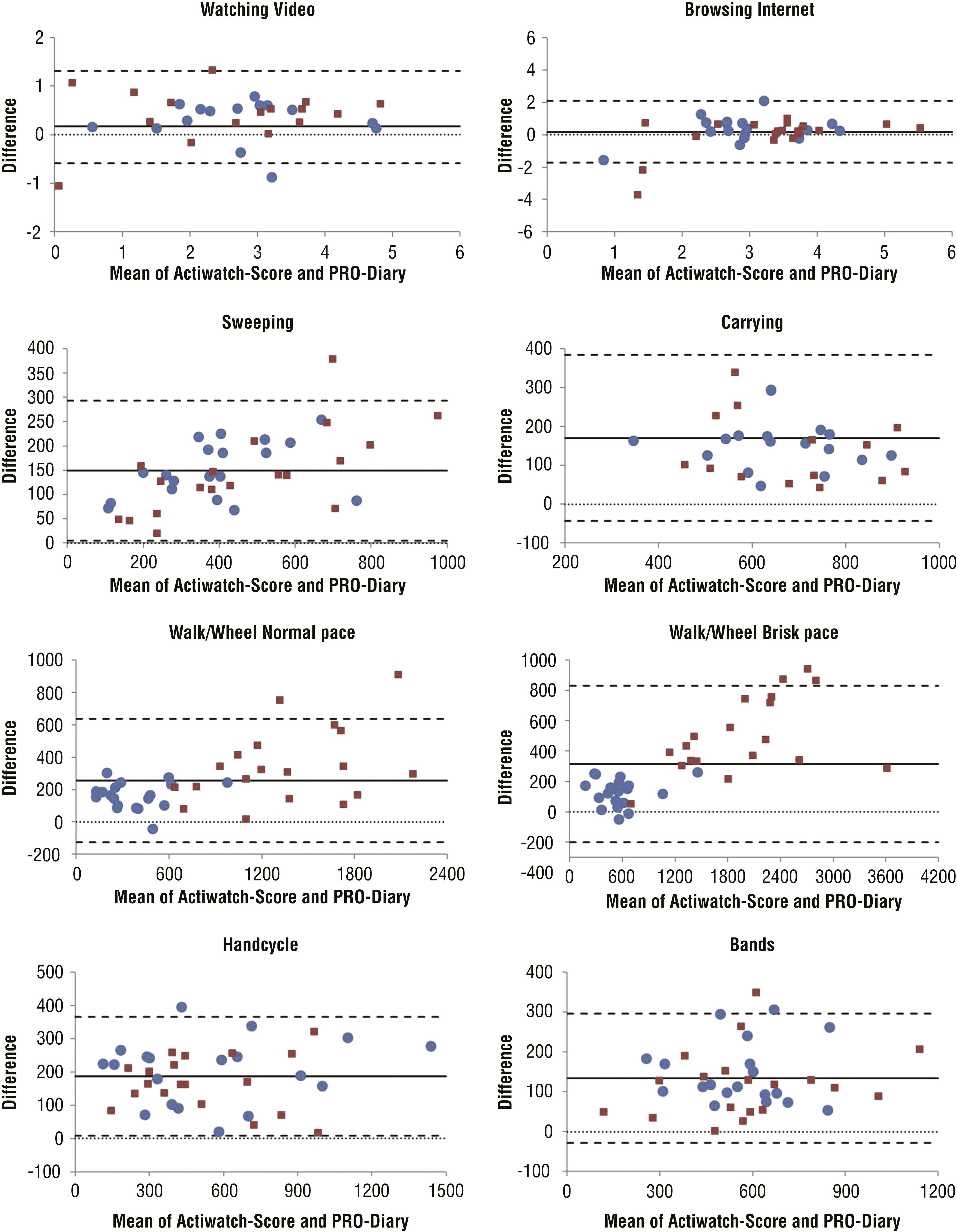
Bland–Altman plots depicting the degree of agreement between Actiwatch Score and PRO-Diary across tasks (SCI: n = 19, red squares; non-SCI: n = 19, blue circles).
Interunit Reliability Estimates for Each Subgroup and Comparison of Physical Activity Levels From One Task to the Next
Note. Physical activity levels were measured by average activity counts per minute generated by Actiwatch Score and PRO-Diary within each group. The p values are for paired t tests comparing within-unit mean differences from one task to the next. diff = difference; ICC = intraclass correlation coefficient (absolute agreement); raw difference = subsequent task activity count − previous task activity count; SCI = spinal cord injury.
For all ICCs, p < .001.
Construct Validity
Mean activity counts per minute across all tasks for each monitor by group are depicted in Figure 2. Means are shown with standard deviations, raw mean differences, percentage mean differences, and p values for paired t tests in Table 2. Results indicate that both monitors measured changes in physical activity from one lab task to the next in both groups, with a few exceptions. Neither monitor detected differences in physical activity level between the two upper extremity exercises (handcycling and therabands) for either group. Additionally, whereas neither monitor detected notable differences in physical activity between the two sedentary tasks for those without an SCI, both monitors showed statistically significant differences in activity (between 93% and 125% change) from video watching to Internet browsing for those with SCI. Similarly, both monitors showed a significant decrease in activity from brisk walking–wheeling to handcycling in the SCI group only, which was due to high activity counts for brisk wheeling in the SCI group.
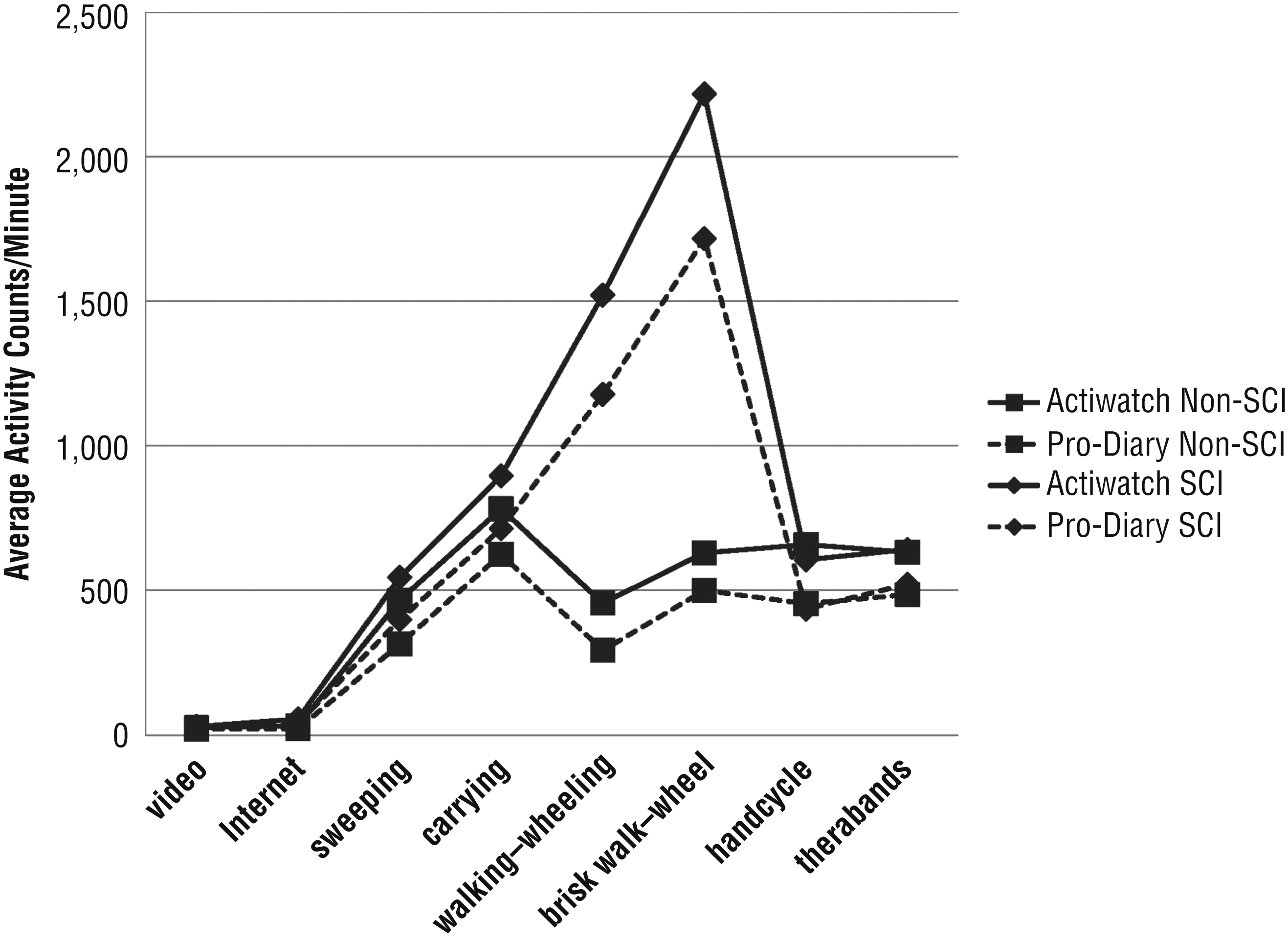
Comparison of mean average activity counts per minute of Actiwatch Score and PRO-Diary across all tasks by group (SCI = 19; non-SCI = 19).
A similar pattern of group differences in activity across the tasks is shown in Figure 2. Only walking–wheeling tasks showed marked differences in activity counts between groups. As expected, participants with SCI had significantly more activity counts per minute compared with those without SCI during ambulatory activities only for both monitors. For walking–wheeling normally, mean activity counts per minute were 3.3 times higher for Actiwatch Score, t(37) = −8.36, p = .0001, and 4 times higher for PRO-Diary, t(37) = −8.16, p = .0001, for those with SCI compared with those without SCI. For walking–wheeling briskly, mean activity counts per minute were 3.5 times higher for Actiwatch Score, t(37) = −8.31, p = .0001, and 3.4 times higher for PRO-Diary, t(37) = −7.38, p = .0001, for those with (compared with without) SCI. Group comparisons of physical activity levels for all other lab tasks were nonsignificant (all ps < .11).
Discussion
This is the first study to compare two wrist-worn accelerometers with self-report capabilities in those with SCI who are manual wheelchair users and those without SCI during laboratory tasks meant to simulate everyday physical activities. The results show that Actiwatch Score and PRO-Diary were highly consistent with each other across lab tasks, demonstrating high interunit reliability as hypothesized. Although Actiwatch Score yielded more activity counts per minute compared with PRO-Diary, this result appears to be a matter of scaling, and activity count patterns of each monitor were highly consistent. Moreover, Actiwatch Score and PRO-Diary demonstrated good construct validity in that they measured significantly different activity counts across tasks for both groups and yielded more activity counts for wheelchair ambulation compared with walking.
Our data suggest that exercises such as therabands and handcycling may be difficult to identify as “exercise” and may appear similar to everyday household tasks in terms of physical activity level as measured by these monitors. On the basis of our findings, it appears necessary to log exercises in addition to the accelerometer to adequately distinguish these exercises in research studies. In contrast, any type of ambulatory task, including wheeling at a comfortable pace, registered high levels of physical activity with wrist-worn accelerometers. Because accelerometers are most sensitive at the site where they are placed (Gironda et al., 2007; Rosenberger et al., 2013; Routen et al., 2012), high activity counts during wheeling from a wrist-worn accelerometer may not be a good representation of physical activity intensity. Additional work is needed to examine energy expenditure to determine activity intensity cutpoints for wrist-worn accelerometers, and this study shows that future researchers will need to separate SCI and non-SCI groups.
Irrespective of our current ability to measure energy expenditure, type, and intensity of physical activity using Actiwatch Score or PRO-Diary, this study suggests practical uses for these monitors, including the ability to characterize participants as relatively more or less active to others in a sample. This capability comes with the caveat that people who ambulate independently should not be compared with those who use a wheelchair (or possibly any type of assistive device). These monitors can also be used to examine within-person changes in activity to identify high activity bouts or to examine momentary associations between physical activity and symptom experience (Murphy et al., 2006, 2007, 2008, 2012). This study imparts some confidence that these monitors detect differences even at low levels of physical activity; this finding is important for those who are not interested just in exercise but in more functional aspects of physical activity that imply engagement in everyday activities (e.g., ADLs).
Implications for Occupational Therapy Practice
To develop occupational therapy interventions that enable people to increase physical activity in their daily life, one should understand each person’s individual level of activity and other self-reported factors that influence activity in real time. This study has the following implications for using these accelerometers as tools to inform research and practice:
Both wrist-worn accelerometers are able to detect differences in physical activities for people with and without SCI, although the scaling is different so they cannot be directly compared.
Before any technology can be confidently used, it must be proven reliable and valid in the population of interest. In populations in which physical impairment is common, accessibility, feasibility, and durability of such technologies are imperative.
Occupational therapy researchers who gather this type of physical activity and self-report data should use the best available technology for their population or risk frustrating respondents and experiencing problems with missing data.
Study Limitations
We did not compare Actiwatch Score or PRO-Diary with a criterion of either physical movement or calorie expenditure. Although this study showed that the monitors were discriminated between different tasks, future studies could examine the energy expenditure during performance of these tasks. All participants underwent the protocol of tasks in the same order, and fatigue may have affected performance on the tasks later in the protocol. Although this choice was designed with the understanding that all participants would be subject to the same bias if it existed, it may be important to vary task order in future studies. Despite limitations, this work provides fundamental information that will inform future research design choices and contributes to a field that has little information about the reliability and validity of these monitors in people with physical disabilities.
Conclusion
This study supports the construct validity of the Actiwatch Score and PRO-Diary to measure everyday activities in people with SCI. Comparison of people with and without SCI showed that the monitors performed similarly except for ambulation tasks of walking versus wheeling tasks. Although additional studies are needed, this study provides support for the use of either of these monitors to assess physical activity in daily life and offers the additional capability of assessing symptoms and other contextual factors in real time.
Footnotes
Acknowledgments
Susan L. Murphy and Anna L. Kratz contributed equally to this work. Financial support was obtained through the pilot grant program of Michigan’s Institute of Clinical and Health Research sponsored by National Center for Advancing Translational Sciences Grant UL1TR002240. Anna L. Kratz was supported by National Institute of Arthritis and Musculoskeletal and Skin Diseases Grant 1K01AR064275.