
Abstract
Concussion, a form of mild traumatic brain injury, is one of the most commonly reported injuries among youth (McCrory et al., 2013). Although most young people recover quickly, a substantial subset (30%–58.5%) report symptoms that persist at 1 mo, and a reported 11%–14% continue to report symptoms beyond 3 mo (Barlow et al., 2010; Zemek et al., 2016).
Standard care after concussion involves rest; education; gradual, symptom-limited return to activities; and a bottom-up approach to treatment of discrete symptoms (e.g., analgesics for headache; Zemek et al., 2014). Youth who are slower to recover are at risk of developing secondary issues (e.g., depression, anxiety, deconditioning) if activities are curtailed for extended periods while awaiting symptom resolution (DiFazio et al., 2016).
We hypothesize that for youth whose symptoms persist for many months, a focus on discrete symptom management and on what they cannot do may have a detrimental effect on their engagement in occupations that are meaningful and important to them (e.g., school and sports). Currently, no evidence-based guidelines for treatment address occupational concerns for youth who are slower to recover from concussion. We postulated that a top-down rehabilitation approach with metacognitive strategy training as the core of the intervention might be effective.
A growing body of literature supports the use of metacognitive strategy training to improve participation in meaningful activity and achievement of self-selected occupation-based goals (Dawson et al., 2017). Metacognitive strategy training approaches foster functional change by promoting self-awareness, self-monitoring, performance adjustment, and generalization and transfer to other tasks and contexts in everyday life (Cicerone et al., 2011).
The Cognitive Orientation to daily Occupational Performance (CO–OP) Approach™ (Dawson et al., 2017; Polatajko & Mandich, 2004) is a metacognitive intervention that has been successfully used to effect clinically significant change in occupation-based performance and satisfaction among adults and youth with mild to moderate traumatic brain injury (Dawson et al., 2009, 2013; Missiuna et al., 2010). Dawson et al. (2009) described how they adapted the approach to suit the needs of adults with brain injury (e.g., increased number of sessions), and Missiuna et al. (2010) used the original approach with youth with brain injury. In practice, clinicians teach clients to use a global strategy (Goal–Plan–Do–Check), by using a process of “guided discovery” to work toward client-chosen activities. Given the long-term occupational concerns among youth with persistent postconcussion symptoms and the lack of evidence-based interventions for these youth, we hypothesized that the CO–OP Approach would facilitate this population’s return to meaningful occupation.
The purpose of this pilot study was to determine the feasibility and effects of the CO–OP Approach for youth with persistent postconcussion symptoms. Our primary objectives were to (1) refine the intervention for this population; (2) collect pilot data regarding effects on performance and satisfaction of self-identified occupation-based goals, self-reported symptoms, and mood; (3) investigate whether the intervention generalizes to other daily activities; and (4) determine whether study procedures are feasible and acceptable to participants and their families.
Method
This study was approved by the research ethics boards of Holland Bloorview Kids Rehabilitation Hospital and Baycrest. All participants (youth and parents) provided informed, written consent.
Design
A prospective case-series design was used. This design is optimal when seeking to establish the feasibility and effects of an intervention in a real-world context (Portney & Watkins, 2009).
Sample
Youth and their parents were recruited from the community and a hospital-based clinic for youth with persistent postconcussion symptoms. Eligibility criteria were as follows: (1) concussion diagnosed by a physician, (2) presence of at least one postconcussion symptom for ≥3 mo, (3) challenges with usual daily activities secondary to postconcussive symptoms, (4) ability to identify four or more occupation-based goals, (5) age 12–18 yr, and (5) no concurrent serious medical or psychiatric diagnoses. We considered parents as study participants because they supported their child’s participation with the study intervention and provided their opinion of the intervention in postintervention interviews.
Measures
Study measures were administered at baseline, immediately postintervention, and at 3-mo follow-up. Participant interviews were conducted immediately postintervention.
Activity Performance (Trained and Untrained Occupation-Based Goals).
The Canadian Occupational Performance Measure (COPM; Law et al., 2014) was used to establish intervention goals and to measure changes in performance of and satisfaction with trained and untrained occupation-based goals. The COPM has been shown to be a valid and reliable measure of change. A change score of 2 points is considered clinically significant (McColl et al., 2006). During a semistructured interview, clients are asked to identify a minimum of five occupational performance issues (OPIs). The client’s five most important OPIs are identified by using a ranking scale ranging from 1 (not important at all) to 10 (extremely important) and then ranked according to performance and satisfaction with performance on 10-point scales (performance score ranging from 1 = not able to do it to 10 = able to do it extremely well; satisfaction score ranging from 1 = not at all satisfied to 10 = extremely satisfied).
Postconcussion Symptoms.
The 22-item Post-Concussion Symptom Inventory (PCSI; adolescent version; Sady et al., 2014) measures the presence and severity of concussion symptoms on a scale ranging from 1 (not a problem) to 6 (severe problem). The PCSI has moderate to good interrater reliability (rs = .4–.5), test–retest reliability (rs = .62–.84), and internal consistency (rs = .72–.93). Higher scores indicate the presence of more or worse symptoms.
Mood.
The Beck Youth Inventories–Second Edition for Children and Adolescents (BYI–II; Beck et al., 2005) provide insight into youths’ negative thoughts about their self, life, and future and feelings of sadness, worry, guilt, anger, disruptive behaviors, and self-worth. The Depression, Anxiety, and Anger Inventories were administered. Higher scores are associated with negative affect. Psychometric properties are strong, with high internal consistency (Cronbach’s αs = .91–.96) and test–retest reliability (rs = .83–.93).
Interview.
Postintervention, youth and their parents participated in individual semistructured interviews to determine whether study procedures were feasible and acceptable. A study-specific interview guide, consisting of open-ended questions (9 questions for youth; 7 questions for parents; e.g., “Tell me what you liked/did not like about the intervention”), was developed by the research team.
Feasibility was determined on the basis of the following criteria: (1) Assessments and reassessments could be completed in <2 hr, including time for symptom-related rest breaks; (2) all 10 intervention sessions could be completed within 9 wk; (3) all study procedures were acceptable to participants, as determined on the basis of positive reviews in their postintervention interview; and (4) positive changes were observed on outcome measures.
Intervention
We used an adapted CO–OP Approach (e.g., we did not use a puppet to teach participants the strategy, and we did not ask participants to complete an activity log before the first meeting) and a modified intervention schedule of ten 30- to 60-min sessions over a 7-wk period (two sessions/week for 4 wk and then one session/week for 3 wk). We posited that providing multiple sessions initially would “kick-start” the intervention, and then frequency of sessions could be reduced as participants became more independent. All sessions took place in participants’ home or in the community rather than in an institutional or clinic setting as in the original CO–OP Approach. Sessions were delivered by an experienced occupational therapist (AWH) trained in CO–OP.
Over the course of the sessions, youth were guided to learn and practice the metacognitive Goal–Plan–Do–Check strategy applied to three trained goals. The therapist used guided discovery, an iterative technique to facilitate problem solving by participants to develop plans to achieve their goals and evaluate their progress. Rather than directly telling participants what to do or how to approach a task, the therapist asked questions to facilitate participants’ development of their own approach (e.g., “How do you think you could do this so your symptoms don’t get worse?”; Dawson et al., 2017). Each session began with a review of (1) the global strategy (Goal–Plan–Do–Check), (2) progress made toward individual goals, and (3) review of the strategies used. Progress toward goals was evaluated at each session through discussion with participants and therapist feedback during observation of actual task performance. The intervention was explained to parents at the initial session. Beyond this, participants were given the opportunity to determine the extent of parental involvement (e.g., attendance at all, some, or no sessions).
Procedure
Preintervention, postintervention, and 3-mo follow-up assessments took place in the research institution of Holland Bloorview Kids Rehabilitation Hospital (Toronto). A trained research assistant (MP) administered all assessments except the initial COPM. The occupational therapist (AWH) administered the initial COPM and set five occupation-based goals collaboratively with participants. Trained and untrained goals were determined as follows: Participants identified one goal they wanted to work on (trained goal). Two other trained goals were then chosen randomly from among the remaining four goals. These three trained goals became the focus of the intervention. Participants were advised in the first intervention session that they could work on their remaining two (untrained) goals independently but that these would not be addressed during sessions. During the intervention, participants worked toward their three trained goals using the metacognitive strategy. Symptoms were explicitly addressed only in the initial session when participants were instructed to try to make their plans so that their symptoms did not get worse. Participants were also instructed to alert the occupational therapist in the event that their symptoms became significantly worse at any point during the study period.
Analyses
Descriptive analyses were used to characterize findings. Treatment was considered clinically significant if a 2-point improvement was found in COPM Performance and Satisfaction scores on trained and untrained goals at posttest. Maintenance of effects and generalization were considered to be demonstrated if improvements in trained and untrained goals were maintained at 3-mo follow-up. Improvements in mood and symptoms were characterized by positive changes in scores from pre- to postintervention on the BYI–II and PCSI, respectively. Acceptability of study procedures and intervention was demonstrated by positive commentary from participants in postintervention interviews and consistent attendance at intervention appointments.
Results
Participants were three female youth (P1, P2, and P3; ages 16, 15, and 17 yr, respectively) who were 11, 10, and 13 mo postconcussion, respectively, and were experiencing postconcussion symptoms at study enrollment. All had previously participated in multiple treatments for symptoms (e.g., physical therapy, chiropractic, cranial–sacral therapy, osteopathy, massage) and reported that they continued to have difficulty engaging in everyday activities. All participants attended all scheduled appointments for assessment and intervention within our targeted time period (≤9 wk). Although all parents attended the first session to learn about the intervention, all 3 participants preferred that their parents not be actively involved in each session. In one instance, a parent did provide support to a participant (P2) when it was specifically part of a plan (e.g., “Ask my mom to remind me to pack my lunch”).
Activity Performance
Participant goals and COPM scores are displayed in Table 1. Clinically significant changes (change of at least 2 points) in performance and satisfaction ratings on trained and untrained goals were reported for all participants postintervention. Average change scores are displayed in Figure 1. All participants maintained positive changes in performance at 3-mo follow-up. P1 had one trained goal that was sport-specific. Because the sport was not in season at the 3-mo follow-up, she was not performing the activity, which resulted in a score of 1 (not performing at all). Clinically significant changes were seen in satisfaction with both trained and untrained goals in all participants from baseline to postintervention. Participant-identified strategies to work toward goals included use of external devices (e.g., scheduling, using phone apps, using sticky notes, conducting Internet searches for information) and verbal self-talk (e.g., talking themselves through an exercise-based activity).
Performance and Satisfaction Ratings on Self-Identified Goals (COPM)
Note.
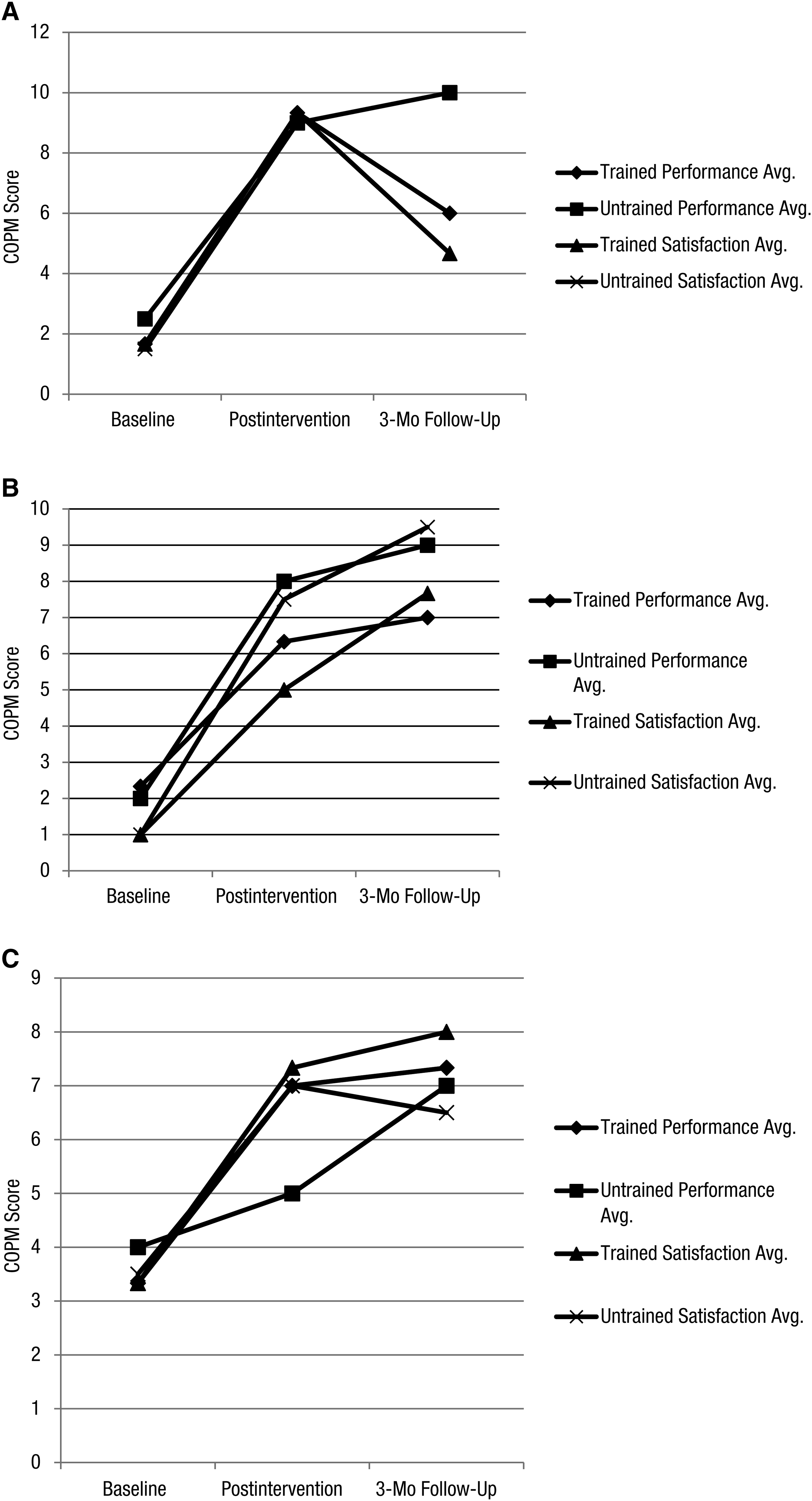
Average changes in performance and satisfaction on trained and untrained goals (determined with the COPM) for (A) Participant 1, (B) Participant 2, and (C) Participant 3.
Symptoms
All 3 participants showed decreases in postconcussion symptoms on both PCSI Total score and the Cognitive and Emotion domains from pre- to postintervention (Figure 2). P3 had a more variable distribution of symptom reporting across the three time points; she also reported that the postintervention and 3-mo follow-up assessments coincided with her high school exam periods.
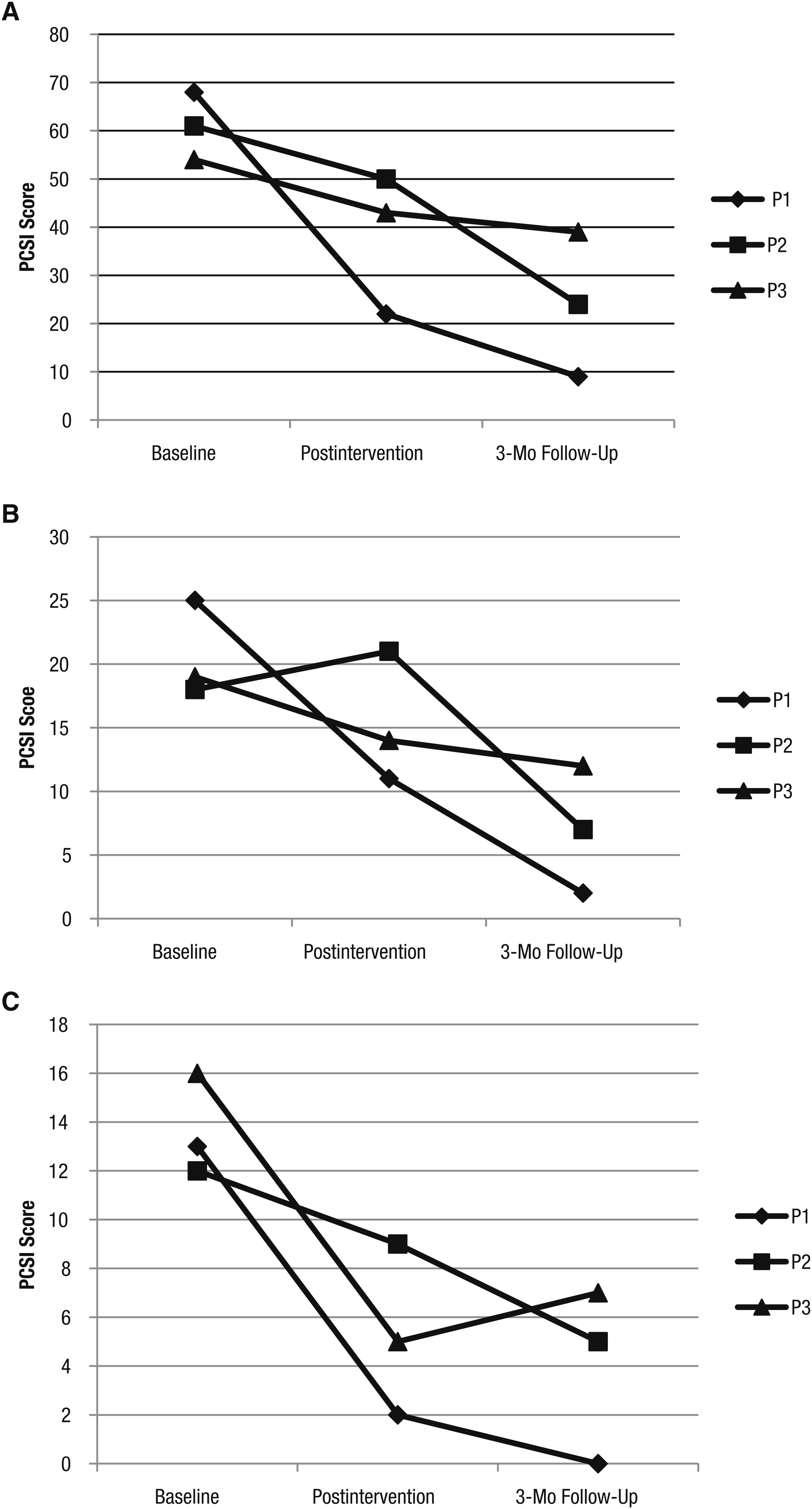
PCSI (A) total, (B) cognitive domain, and (C) emotional domain scores.
Mood
Findings regarding mood varied across the 3 participants (Figure 3). P1 displayed similar trends across the Anxiety, Anger, and Depression Inventories, with sharp decreases in score from baseline to postintervention (indicating improvements) and then small increases (indicating worsening) from postintervention to 3 mo-follow-up, but her scores still improved from baseline. P2 demonstrated few changes across time on all three inventories. P3 showed decreases (improvement) from baseline to postintervention across all inventories, but these scores returned to baseline at the 3-mo follow-up.
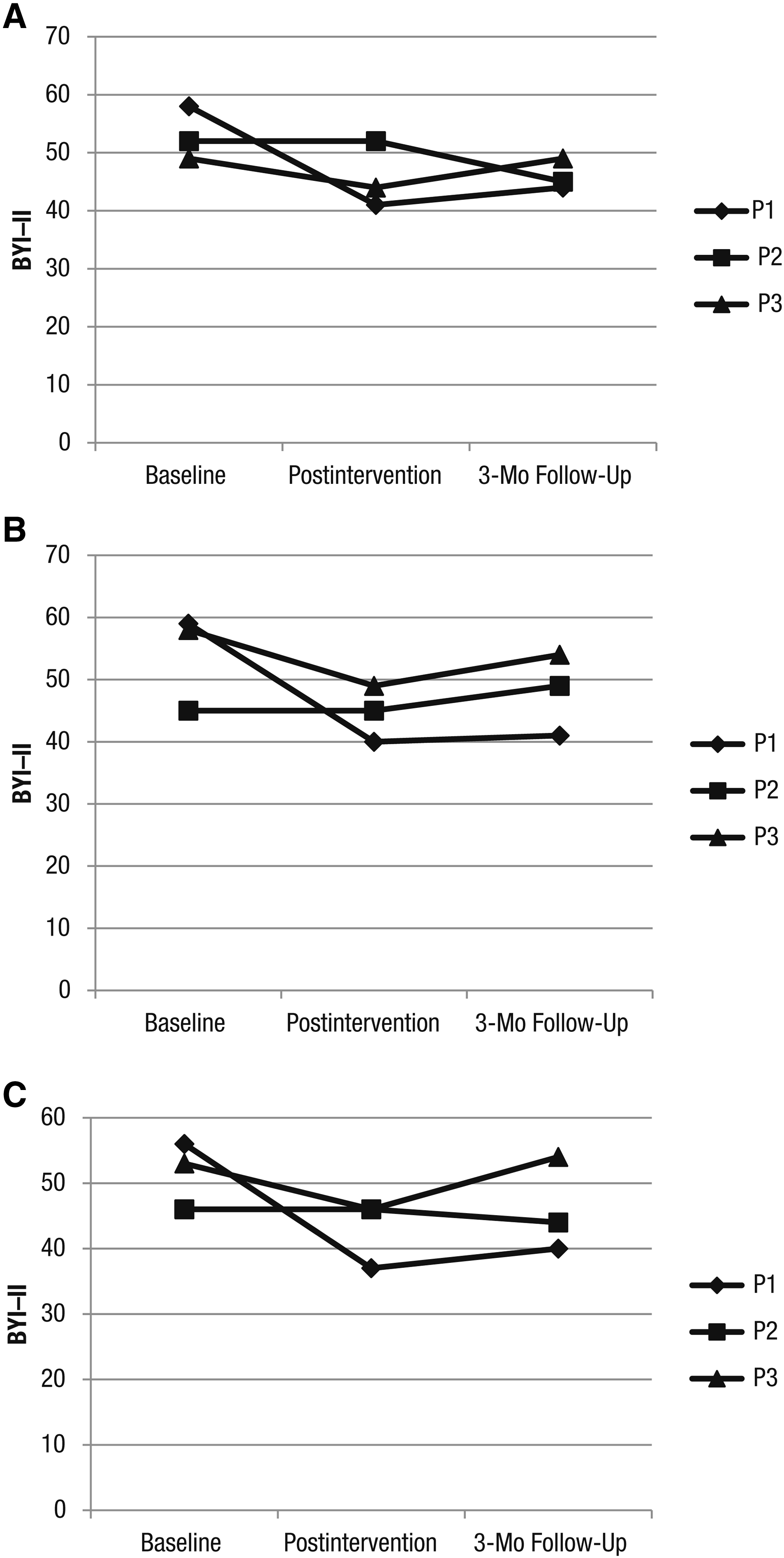
Changes in BYI–II (t scores): (A) Anxiety Inventory, (B) Depression Inventory, and (C) Anger Inventory.
Participants’ Experience
Postintervention interviews ranged from 20 to 55 min. All participants and their parents reported that the study procedures and intervention were acceptable. The parents of 2 participants indicated that they would have liked a longer intervention period. They felt their child was “finally beginning” to reintegrate into school and activity and that additional support for several months would have helped to maintain their child’s progress. All 3 participants and their parents stated that they would highly recommend this type of intervention to others.
Discussion
This study is to our knowledge the first to use a top-down occupational rather than a bottom-up symptom-based approach to sport-related concussion management in youth. Our findings from this preliminary work suggest that the CO–OP Approach may make a positive contribution to recovery. All participants made clinically significant positive changes in activity performance and satisfaction on both trained and untrained goals, and these changes were maintained at 3-mo follow-up, indicating that intervention effects may be both transferable and generalizable. Participants identified goals related to school (e.g., completing homework), sport (e.g., participating in fitness activities), leisure (e.g., reading), and health and wellness (e.g., using a sleep routine). Decreases in cognitive (e.g., difficulty remembering, concentrating) and emotional (e.g., nervousness, feeling more emotional) symptoms, for which very few evidence-based treatments are available for youth, were also observed. All assessment and intervention procedures were feasible and acceptable to all study participants.
The intervention focused on working toward achievement of self-identified, meaningful, occupation-based goals in participants’ home or community environment. The approach provided a safe opportunity for doing rather than focusing on activity restrictions (i.e., what they could not do). Before the study, participants and their parents were focused on limiting activities, resting, receiving treatments for discrete symptoms (e.g., headaches), and waiting for symptoms to resolve before resuming activities. That is, they were focused on what they could or should not do. The focus on doing in this study is supported by emerging research in the concussion literature that activity-based approaches such as exercise are effective means of rehabilitation for youth postconcussion (Gagnon et al., 2009; Kurowski et al., 2016). These active approaches to postconcussion rehabilitation are consistent with the most recent expert-based consensus concussion management guidelines (McCrory et al., 2017) that promote an initial period of rest followed by gradual resumption of activity.
All participants experienced a reduction in symptoms postintervention and at follow-up. Reductions were seen in cognitive (e.g., difficulty remembering, getting confused with tasks) and emotional (e.g., sadness, nervousness) symptoms for which treatment options are currently limited. Although emerging evidence has suggested that cognitive–behavioral therapy might be effective for some youth postconcussion (McCarty et al., 2016), our findings offer another possible treatment option to target cognitive and emotional symptoms. The intervention may reduce the perception of cognitive and emotional symptoms by focusing on independent behavioral self-regulation and positively influencing participants’ self-confidence. Enabling participants to identify and “do” plans and to create new plans when previous plans were unsuccessful gave participants performance feedback, independence, and control over how to reengage in activities. The “check” of how plans worked enabled participants to make a direct link between their activities and exacerbation of symptoms (i.e., “My plan to do my homework immediately after school didn’t work because I had a headache after school; my new plan will be to rest after school and then do homework”). That participants demonstrated clinically significant changes on both trained and untrained goals suggests preliminary evidence of generalization; that is, participants used the approach to reengage in other meaningful activities in their lives that may also have contributed to enhanced self-confidence.
The use of a metacognitive strategy during concussion recovery may have important implications for return to school. As our participants’ goals show (e.g., P1’s goal to complete physics homework, P3’s goal to complete assignments on time), metacognitive strategies may enable youth to balance the cognitive workload associated with school-based activity with their tolerance of postconcussion symptoms. This outcome may be highly relevant for gradual return to school postconcussion, especially given findings that cognitive rest is not necessarily associated with symptom reduction (Gibson et al., 2013).
Findings from youth and parent interviews regarding their experiences with the intervention were very favorable. Surprisingly, there were no study appointment cancellations; this is unusual in pediatric rehabilitation where the multiple demands on families can affect consistent participation. We believe that the focus on occupation, use of client-identified goals, and provision of intervention in the clients’ own environment where working toward these goals was most meaningful and convenient to families contributed to this positive experience.
Study Limitations and Future Directions
Although the initial results of this study are promising, it was nonetheless carried out with only 3 participants, all of whom were female. More rigorous study, including larger samples with both male and female participants and control participants, is needed. Neuropsychological testing would be beneficial to understand the cognitive profile of youth who may benefit from a metacognitive strategy training approach. Because effects were not consistently maintained at 3-mo follow-up, future research should address how to maintain postintervention improvements over the long term, possibly through a longer intervention period or booster sessions.
Implications for Occupational Therapy Practice
The CO–OP Approach may be a treatment option for youth with persistent postconcussion symptoms. It enables youth to focus on what they can do postconcussion, not on what they cannot do. This study has the following implications for occupational therapy practice:
The iterative process of guided discovery, which involves asking, not telling, may facilitate reengagement in meaningful activity.
The intervention session schedule supports that more frequent sessions initially (e.g. twice-weekly sessions for the first 4 wk) followed by a gradual reduction in sessions may be helpful for youth postconcussion.
This approach may be useful for youth who are returning to school postconcussion or who have been out of school or sport for prolonged periods because the intervention may reduce the perception of cognitive and emotional symptoms by focusing on independent behavioral self-regulation and positively influencing participants’ self-confidence.
Conclusion
The adapted CO–OP Approach to rehabilitation for youth with persistent symptoms after concussion is feasible and may make a positive contribution to activity resumption, symptom reduction, and mood. More rigorous study is warranted.