
Abstract
Chronic pain can have a significant impact on physical, cognitive, and psychological function (Aegler & Satink, 2009). Approximately 100 million adults in the United States have chronic pain, at a cost of $560–$635 billion annually for lost productivity and pain-related medical expenses (Institute of Medicine, 2011). Chronic pain is defined as pain that has not resolved within the expected time frame of 3 mo and that is not responsive to routine pain intervention (Tunks et al., 2008). Pacing is an intervention strategy commonly used by occupational therapy practitioners as a component of multidisciplinary pain management services (Nielson et al., 2013). The absence of a single accepted definition of pacing has resulted in the use of various definitions in the literature (Antcliff et al., 2015). For example, pacing is often used interchangeably with activity pacing (Nielson et al., 2014), adaptive pacing (White et al., 2011), and operant-based activity pacing (Andrews et al., 2016).
For people with chronic pain, pacing is a learned skill that involves preplanning (Sternbach, 1978) in an effort to balance over- and underactive tendencies and improve level of function (Gill & Brown, 2009). Pacing can facilitate the reintroduction of activity and increase activity (Kos et al., 2015). Encompassed in pacing is pacing up, which involves people gradually increasing the duration of occupational participation over time. Pacing as a learned strategy differs from pacing as an instinctive response because rather than taking rest breaks as a reaction to increasing pain severity, a preplanned intervention is used to increase functional tolerances over time (Andrews et al., 2012).
There is a paucity of evidence (Antcliff et al., 2015) and a lack of agreement regarding the effectiveness of pacing as a pain management strategy for people with chronic pain (Gill & Brown, 2009). In a review of the evidence, the effectiveness of pacing as an intervention for people with chronic pain was unable to be verified (Gill & Brown, 2009). Nielson et al. (2013) reported that the effectiveness of pacing had not been evaluated as a stand-alone intervention because it was often included within larger intervention programs. In contrast to the clinical intention of pacing, its use has been associated with lower levels of physical functioning in people with rheumatoid arthritis (Cuperus et al., 2012) and greater levels of pain and disability reported by those with chronic pain (Andrews et al., 2012).
Although two literature reviews on pacing (Gill & Brown, 2009; Andrews et al., 2012) have been undertaken, the first of these reviews (Gill & Brown, 2009) used a structured review of the literature, which by design may not have located all relevant literature. The second review (Andrews et al., 2012) included studies that reported on correlation coefficients between at least one measure of pacing behavior and patient functioning. This review therefore included studies in which pacing was not investigated as a learned intervention and reported on associations between pacing and outcomes rather than causations. The limitations of these reviews and the lack of clarity regarding the effectiveness of pacing as a learned intervention for adults with chronic pain justify the need to undertake a systematic review of the literature.
Method
We conducted a systematic review to evaluate the evidence regarding the effectiveness of pacing. The research question for this systematic review was “How effective is pacing as a learned strategy for adults with chronic pain?” The reporting format for the systematic review was based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Shamseer et al., 2015).
Inclusion and Exclusion Criteria
Inclusion criteria for this systematic review required published peer-reviewed articles to be written in English (conference abstracts and qualitative studies were excluded) and adult participants age 18 yr or older with chronic pain and receiving outpatient services. In addition, participants using pacing as a strategy had to be the focus of the intervention study, and the definition of pacing had to be consistent with the activity pacing criteria of Murphy and colleagues (2010; i.e., individuals planning ahead and dividing tasks into multiple time blocks, tasks interspersed with rest breaks, and individuals aiming not to exacerbate their symptoms). Studies using variations of the term pacing, such as activity pacing or adaptive pacing, were included if the definition used was consistent with the definition outlined in the eligibility criteria of this article. For the purpose of this review, we use pacing. Study outcomes had to reflect the domains of participation, activity, and impairment according to the International Classification of Functioning, Disability and Health (ICF; World Health Organization [WHO], 2001). Classifying outcomes within the ICF domains enabled categorization and comparison of the type of outcomes in the literature.
Information Sources and Search Strategy
Six databases were searched in March 2016: CENTRAL, OTseeker, PEDro, CINAHL, MEDLINE, and Embase. Combinations of the following key words and MeSH terms were used as search terms: pacing, paced, activity pacing, and pain. Database-specific operators, truncations, and wildcards were used to refine the search strategies.
Study Selection and Data Extraction
Two authors (LG and CM) reviewed the titles and abstracts of articles for eligibility. When eligibility could not be determined with this review, a full-text review was conducted. Two authors (LG and CM) checked references and citations in included studies using the abstract and citation database SCOPUS to retrieve additional relevant studies. Any disagreements between LG and CM concerning the eligibility of a study were resolved with discussion with the third author (CB).
Two authors (LG and CM) independently extracted data from each study using a data extraction form. This process began with extracting data regarding inclusion and exclusion criteria. If a study was deemed ineligible, it was excluded from the systematic review (Figure 1). Extracted outcome data were aligned with the ICF domains, specifically participation, activity, and impairment (WHO, 2001).
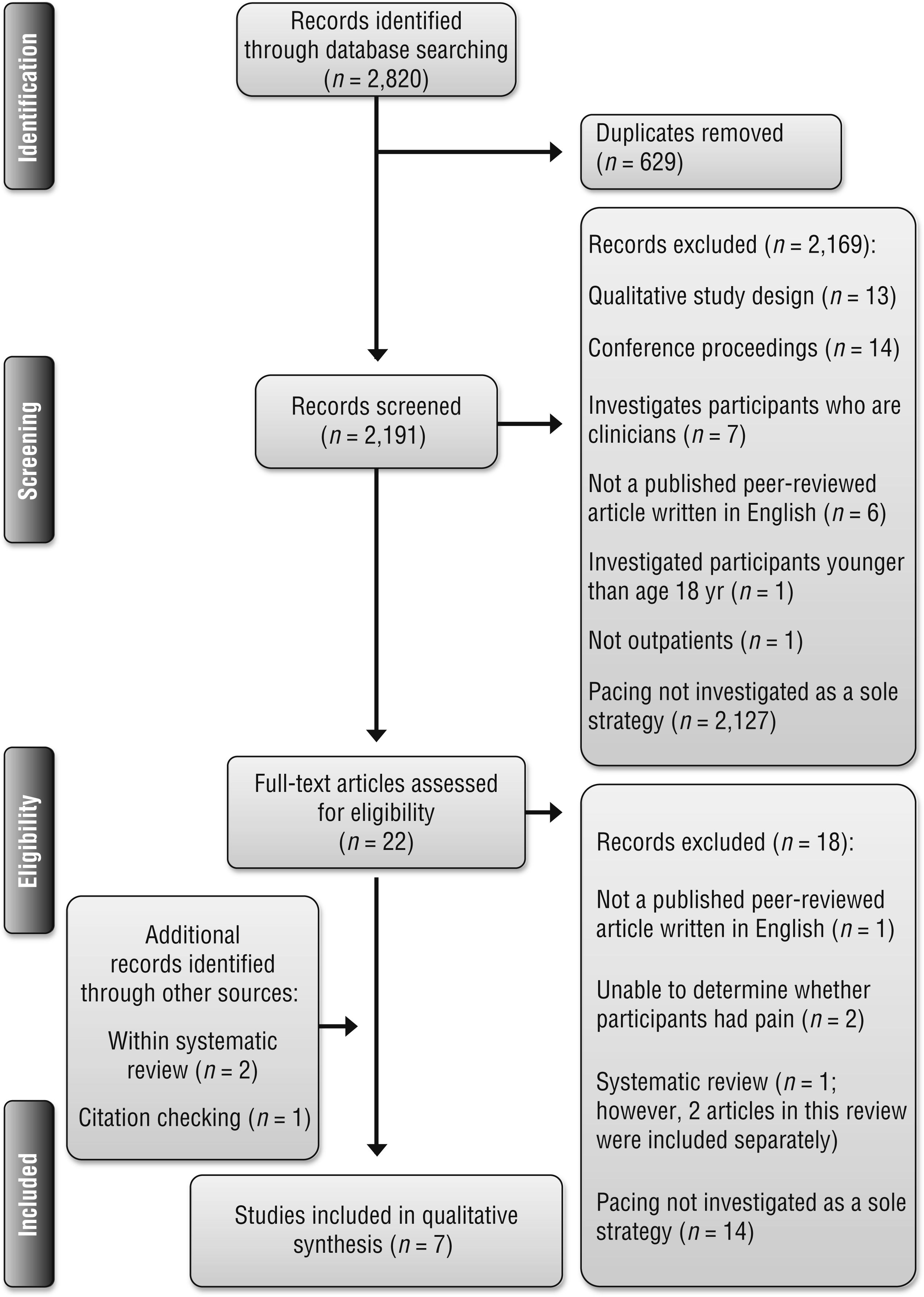
Flow diagram of articles identified, screened, eligible for, and included in the systematic review.
Risk of Bias in Individual Studies
Two authors (LG and CM) used the Cochrane Collaboration’s tool for assessing risk of bias (Higgins & Green, 2011) and the McMaster University Critical Review Form for Quantitative Studies (Law et al., 1998) to determine the methodological quality of each study. Any disagreements between these two authors were resolved through discussion, and if required, the third author (CB) was consulted to assist in achieving consensus.
The Cochrane Collaboration’s tool for assessing risk of bias assesses six specific domains. The tool involves two parts. In the first part, the assessor describes what has happened in each domain (Higgins & Green, 2011). In the second part, the assessor makes a judgment regarding the risk of bias as being low, unclear, or high risk (Higgins & Green, 2011).
The McMaster University Critical Review Form for Quantitative Studies checklist (Law et al., 1998) enables the appraisal of both randomized and nonrandomized study designs within eight domains of methodological quality. Guerin et al.’s (2013) rating scale was used to determine methodological quality, with 1 = yes and 0 = no or not addressed. Scores could range from 0 to a maximum total of 14. In addition, items that were rated not applicable were deducted from the overall score (Guerin et al., 2013). The checklist scores were calculated to provide a rating in which the higher the percentage was, the higher the overall methodological quality.
Data Synthesis
A wide range of clinical outcomes were reported across the included studies, which investigated different populations. Because of the heterogeneity of data presented, a meta-analysis could not be conducted. Therefore, a narrative review was deemed most appropriate and was undertaken. We analyzed the included studies for similarities in outcomes within the relevant outcome categories of impairment, activity, and participation. The strength of evidence within themes was determined using U.S. Preventive Services Task Force (2012) ratings:
• Strong evidence—consistent results from at least 2 well-conducted randomized controlled trials (RCTs)
• Moderate evidence—at least 1 RCT or at least 2 studies providing lower levels of evidence, with inconsistencies in findings across well-designed individual studies
• Limited evidence—too few research studies, often with flaws, to make specific recommendations
• Mixed evidence—inconsistent or conflicting findings throughout studies.
Results
Of the 2,820 articles that were located and screened, 7 met the inclusion criteria and were included in data synthesis (see Figure 1). Characteristics of the 7 studies are described in an evidence table (Supplemental Table 1; available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). All eligible studies used an RCT study design, which is Level 1 within the hierarchy of evidence grading (Guyatt et al., 1995). Three of the eligible studies (Murphy et al., 2010, 2012; Schepens et al., 2012) reported on different outcomes from the same trial, which was a pilot study. The eligible studies investigated a range of populations, including people with fibromyalgia, chronic fatigue syndrome, and osteoarthritis. The sample sizes of the included studies varied from 30 to 640, with a total of 1,007 participants across the 7 studies. The samples generally had more female than male participants.
The period of intervention varied from a single 30-min session (Meeus et al., 2010) to 10 sessions provided over a 36-wk time frame (Bourke et al., 2014). In 2 studies (Meeus et al., 2010; Van Oosterwijck et al., 2013), pacing was provided to the control group as an intervention. Three of the studies included two different pacing intervention approaches: a general pacing intervention and a tailored pacing intervention (Murphy et al., 2010, 2012; Schepens et al., 2012). The pacing approach used differed, with some interventions focusing on symptom management (Meeus et al., 2010; Murphy et al., 2010, 2012; Schepens et al., 2012) and others providing education on pacing up to facilitate an increase in activity (Bourke et al., 2014; Van Oosterwijck et al., 2013). All interventions were provided verbally by therapists, and some also included the provision of written information (Murphy et al., 2010, 2012; Schepens et al., 2012; Van Oosterwijck et al., 2013) and individualized reports that detailed the relationship between the participant’s activity level and symptoms (Murphy et al., 2010, 2012; Schepens et al., 2012). None of the interventions used an occupation-based approach in which pacing was implemented practically within an occupation under the guidance of a therapist.
Risk of Bias Within Studies
The Cochrane Collaboration’s tool for assessing risk of bias (Higgins & Green, 2011) was used for each study (Table 1). Most studies demonstrated methodological strengths in their random sequence generation, allocation concealment, blinding of outcome assessment, reporting of short-term outcome measurement data, and quality of reporting. There was difficulty determining risk of bias regarding the blinding of participants and personnel. Methodological strength was compromised in the studies that did not report long-term outcome measurement data (Bourke et al., 2014; Murphy et al., 2010, 2012).
Risk of Bias of the Studies Included in the Systematic Review
Note. Categories for risk of bias: + = low risk of bias; ? = unclear risk of bias; – = high risk of bias. N/A = not applicable.
Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), by J. P. T. Higgins and S. Green (Eds.), 2011, London: Cochrane Collaboration. Retrieved from http://handbook-5-1.cochrane.org. Copyright © 2011 by The Cochrane Collaboration.
A summary of the methodological quality domain scores of included studies is presented in Table 2. Completion of the McMaster University Critical Review Form for Quantitative Studies checklist (Law et al., 1998) indicated that the quality of the included studies varied from 43% (Bourke et al., 2014) to 100% (Meeus et al., 2010), with higher percentages meaning higher quality.
Methodological Quality Domain Scores of Studies Included in the Systematic Review
Note. Scores for methodological quality domains: 1 = yes, 0 = no or not addressed. N/A = not applicable.
1 = Was the study purpose stated clearly? 2 = Was the relevant background literature reviewed? 3 = design, (not scored); 4a = Was the sample described in detail? 4b = Was the sample size justified? 5a = Were the outcome measures reliable? 5b = Were the outcome measures valid? 6a = Intervention was described in detail? 6b = Contamination was avoided? 6c = Cointervention was avoided? 7a = Results were reported in terms of statistical significance? 7b = Were the analysis method(s) appropriate? 7c = Clinical importance was reported? 7d = Dropouts were reported? 8 = Conclusion was appropriate, given the study methods and results.
All of the included studies stated the study purpose, reviewed relevant literature, reported results in terms of statistical significance, and described the clinical significance of their results. Except for Bourke et al. (2014), all studies had methodological strength in their detailed description of the sample and the intervention. The data analysis methods were appropriate, and dropouts were reported in all eligible studies except Schepens et al. (2012). The conclusions made by study authors were appropriate given the study methods and results, except for Bourke et al. (2014), who drew conclusions that were not based on the study purpose or results.
There was variation among the included studies in how quality indicators were addressed including justification of sample sizes, whether reliability and validity outcomes were reported, and whether transparency was established regarding avoidance of contamination and co-intervention.
Synthesis of Results
The qualitative synthesis resulted in three main themes, reflecting the ICF impairment, activity, and participation domains (WHO, 2001). These themes describe the primary outcomes associated with the use of pacing as a learned strategy for adults with chronic pain.
Impairment.
The majority of the outcomes investigated across the 7 studies were categorized within the domain of impairment. The findings of this systematic review indicate that there is strong evidence that pacing as a learned strategy does not significantly reduce pain (Murphy et al., 2010, 2016; Van Oosterwijck et al., 2013). Reduction of pain was investigated across two different populations—people with osteoarthritis and people with fibromyalgia—using two different outcome measures: the Western Ontario and McMaster Universities Osteoarthritis Index and the Medical Outcomes Short Form 36 Health Survey, Dutch translation. There is moderate evidence to indicate that pacing does not significantly reduce muscle pain or joint pain in a population with chronic fatigue (Bourke et al., 2014) or reduce endogenous pain inhibitory mechanisms in a population with fibromyalgia (Van Oosterwijck et al., 2013). There is strong evidence that pacing does not increase pain thresholds for people with chronic fatigue or fibromyalgia (Meeus et al., 2010; Van Oosterwijck et al., 2013).
There is strong evidence that pacing as a learned strategy does not significantly alter adaptive and maladaptive psychological traits, including transforming, distraction, reducing demands, retreating, worrying, resting, helplessness, magnification, ruminating, and kinesiophobia for those with chronic fatigue and fibromyalgia (Meeus et al., 2010; Van Oosterwijck et al., 2013). There was also moderate evidence that pacing did not influence the mental health of participants or overall catastrophic thoughts about pain or hypervigilance for pain (Van Oosterwijck et al., 2013).
There was mixed evidence regarding effectiveness of pacing and fatigue severity. Murphy et al. (2010) reported a moderate effect size between intervention groups when comparing a tailored pacing intervention with a general pacing intervention. In comparison, Murphy et al. (2016) found no significant changes between pacing intervention groups and a usual-care group for the outcome of fatigue. Murphy et al. (2010), however, reported a large effect size and significant difference between groups regarding fatigue interference in favor of the tailored intervention group. Moderately strong evidence also supports tailored pacing interventions to significantly reduce joint stiffness in people with osteoarthritis (Schepens et al., 2012).
Activity.
Evidence was scarce within the domain of activity. There was moderate evidence for pacing as a tailored intervention to significantly reduce variability in physical activity compared with a general pacing intervention in a population with osteoarthritis (Murphy et al., 2010). Pacing as a learned strategy did not influence the outcomes of average activity level, physical disability, or physical functioning in participants with osteoarthritis (Murphy et al., 2012, 2016) or fibromyalgia (Van Oosterwijck et al., 2013).
Participation.
There was a limited use of outcomes categorized in the domain of participation and few high-quality results. Pacing as a learned strategy does not significantly reduce people’s role limitations as a result of physical pain or emotional problems or improve social functioning for those with fibromyalgia (Van Oosterwijck et al., 2013).
Discussion
This systematic review found moderate to strong evidence that pacing, as a learned strategy for adults with chronic pain, does not reduce pain severity or improve psychological health. Moderate levels of supporting evidence indicate that pacing could assist with reducing joint stiffness and variability in activity levels, although whether pacing can influence the impact of fatigue is undetermined. Because only 7 articles were eligible for this review, and given the heterogeneity of the populations investigated and the outcomes selected, the ability to synthesize evidence was limited. Consistent with conclusions by Gill and Brown (2009), Nielson et al. (2013), and Andrews et al. (2012), there is a paucity of literature investigating the effectiveness of pacing as a pain management strategy.
A majority of the outcome measures used in the eligible studies were categorized in the domain of impairment. Outcomes that could be categorized in the domains of activity and participation were scarce. This was an unexpected finding given that a primary purpose of pacing is to improve a person’s ability to participate in daily activities and occupations while managing pain. Pacing is proposed to be of value to people who have adopted maladaptive ways to manage their pain, such as underactive or overactive approaches; therefore, it would be useful to understand the impact that pacing can have in the domains of activity and participation. These findings indicate that there is a lack of understanding about the impact of pacing on a person’s satisfaction with participation in occupations and ability to fulfill life roles and sense of identity.
The definition of pacing varied among studies, creating the question of whether the results consistently capture the true intention of pacing. A key component of pacing is the notion of pacing up to increase activity tolerances over time; however, not all studies incorporated this component into their intervention design (i.e., Meeus et al., 2010; Murphy et al., 2010, 2012; Schepens et al., 2012). The variability in the definition of pacing has also been reported in previous literature (Andrews et al., 2012; Antcliff et al., 2015; Birkholtz et al., 2004).
The eligible studies had various chronic pain target populations, including people with fibromyalgia, osteoarthritis, and chronic fatigue syndrome. Chronic pain exists in a range of other conditions, such as chronic musculoskeletal pain, back pain, cancer, and complex regional pain syndrome. Therefore, the generalizability of the findings of this review to other populations with chronic pain is limited. The variability within the populations also reduced the combined strength of the evidence.
Most of the interventions in the included studies could be used in usual practice except for the intervention design used by Bourke et al. (2014). This intervention was provided across 32 wk, which may be too long for multidisciplinary pain management services, which often provide shorter term rehabilitation options.
All included studies provided the pacing intervention from an educational perspective, with no studies using a practical or occupation-based approach in which the pacing strategy was embedded into activities or occupations under the guidance of a therapist. The lack of occupation-based elements in the pacing intervention is a key limitation of the intervention designs of these studies because clinical practice often involves both educational and practical components. Pacing education that is focused on a client’s daily occupations and routines could be more effective than a focus on performance skills or physical capacity (Andrews et al., 2016). In addition, the use of occupation-based interventions is perceived to be a powerful treatment approach that facilitates participation and independence within meaningful occupations (Colaianni & Provident, 2010; Jack & Estes, 2010).
No detrimental effects were reported for the implementation of pacing. In contrast, a recent systematic review by Andrews et al. (2012) found a positive correlation between pacing and decreased function and increased pain. Andrews et al. included studies that did not investigate pacing as a learned strategy; therefore, the results may have captured how people naturally pace and how naturally pacing might contribute to a decline in functional ability.
Implications for Occupational Therapy Practice
The findings from this study have the following implications for occupational therapy practice:
The current evidence supports the use of pacing as a tailored intervention for adults with chronic pain to reduce the interference of fatigue, reduce joint stiffness, and decrease variability in physical activity.
The current evidence does not support the use of pacing as a learned strategy to reduce pain or influence psychological traits.
The evidence is not sufficient to determine whether pacing can improve a person’s average activity level, participation in life roles, participation in social functioning, or reduction in fatigue severity.
Occupational therapy practitioners are recommended to use their clinical experience and narrative clinical reasoning when advising on appropriate intervention options with their clients and customizing pacing interventions to the client.
Implications for Occupational Therapy Research
Future RCTs, using validated and reliable outcome measures, are needed to increase the potential to conduct a meta-analysis of results. Researchers should ensure they justify their sample size to improve the quality of their study design. Additional research should consider investigating pacing among populations with other types of chronic pain conditions, such as musculoskeletal chronic pain and complex regional pain syndrome, to improve the generalizability of study results.
Future studies should investigate different intervention conditions, such as the length and frequency of intervention sessions or whether the intervention should be tailored, to determine the optimal methods to use to provide a pacing intervention. In addition, studies should ensure that the design of the pacing intervention could be realistically replicated in clinical practice settings to improve the generalizability of results. Given that the use of occupation is core and unique to occupational therapy, future intervention designs incorporating an occupation-based therapy approach are needed. Additional research is required to investigate the effectiveness of pacing as a learned strategy in the activity and participation outcome domains in determining the impact that pacing can have on a person’s ability to participate in daily occupations and life roles.
Implications for Occupational Therapy Education
Educators should ensure that the essential elements comprising the concept of pacing, including preplanning, alternating activity, rest before symptom exacerbation, and pacing up, are included in the curriculum content. Educators are recommended to provide options of different methods for delivering a pacing intervention, for example, the length and frequency of sessions and a customized or general strategy. In addition, occupational therapy practitioners require enhanced clinical reasoning skills to enable decision making about how and when a pacing intervention is appropriate when working with people with chronic pain.
Limitations
Limitations of this systematic review include the narrow breadth of researchers investigating this topic in the field: Murphy was an author of 4 of the 7 studies included; Lyden, of 3 studies; and Smith, Van Oosterwijck, and Meeus, of 2 studies. The limited range of study geographical locations (4 of the 7 studies were conducted in the United States, 2 in Belgium, and 1 in the United Kingdom) reduces the generalizability of this review’s results. Small sample sizes were used with no justification in studies by Murphy et al. (2010, 2012), Schepens et al. (2012), and Bourke et al. (2014). Small sample sizes can yield unreliable results and may not be representative of the population of interest (Carandang et al., 2016), limiting the reliability of the findings and conclusions made in this review. The heterogeneity of variables across the 7 studies, including participant pain type, intervention design, and definition of pacing used, limits the strength of the accumulated results. In addition, the heterogeneity of outcome measures and outcomes prevented us from conducting a meta-analysis.
Conclusion
Current research provides evidence that the use of pacing as a learned strategy for people with chronic pain does not influence pain severity or psychological traits; however, it can assist in reducing the interference of fatigue and joint stiffness and decreasing physical activity variability. Future research is needed to investigate pacing as a learned strategy in the ICF (WHO, 2001) domains of activity and participation to better understand its impact on a client’s day-to-day life. Future research is also needed to clarify whether pacing is better delivered as a customized strategy or a generic strategy.
Supplemental Material
Supplementary material for Effectiveness of Pacing as a Learned Strategy for People With Chronic Pain: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.028555.pdf for Effectiveness of Pacing as a Learned Strategy for People With Chronic Pain: A Systematic Review by Lauren Guy, Carol McKinstry and Chris Bruce in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Western Health for providing support to undertake this review. This research received no specific grant support from any funding agency in the public, commercial, or not-for-profit sectors. The authors declare no conflict of interest. The systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO; No. CRD42016049629).
*
Indicates studies that were included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.