
Abstract
People with Parkinson’s disease (PD) frequently report difficulty with tasks involving manual dexterity such as buttoning clothing, handwriting, tying shoelaces, and typing on a keyboard (Nijkrake et al., 2009). This impairment is traditionally ascribed as a consequence of bradykinesia, defined as slowness of movement. Bradykinesia is typically assessed through clinical assessment of repetitive movements, including repetitive finger movements. However, little is known regarding how repetitive finger movement performance affects fine-motor dexterity tasks in people with PD.
Research has shown that impairments in simple repetitive finger movements emerge at high movement rates (>2 Hz, or 120 movements/min; Freeman et al., 1993; Nakamura et al., 1978; Stegemöller et al., 2009, 2010; Yahalom et al., 2004). The performance of dexterity tasks involving manipulative serial hand movements is also frequency dependent based on the sensory control process required (Kunesch et al., 1989). Dexterity tasks that involve focal sensory control are performed slower (<2 Hz), whereas dexterity tasks that involve preattentive sensory processes are performed faster (Kunesch et al., 1989). Thus, the purpose of this study was to examine the relationship between the performance of fine-motor dexterity tasks and high-rate repetitive finger movement in people with PD.
Both buttoning and Purdue pegboard tasks have been used to examine fine-motor dexterity in people with PD (Foki et al., 2016; Proud & Morris, 2010; Smiley-Oyen et al., 2006; Tan et al., 2003). However, few studies have examined the relationship between repetitive finger movement performance and performance on the Purdue pegboard test in people with PD. Müller and colleagues (2000) found a significant correlation between finger tapping as fast as possible and insertion of pegs in the Purdue pegboard. More recently, Růžička and colleagues (2016) demonstrated a significant correlation between clinical ratings of finger tapping using the Unified Parkinson’s Disease Rating Scale (UPDRS; Goetz et al., 2008) and performance on the Purdue pegboard test. However, the movement rate of the tapping tasks in these studies was not controlled, and specific kinematic elements of movement amplitude and movement rate were not explored. In contrast to findings on the Purdue pegboard test, Foki and colleagues (2016) showed that clinical measures of bradykinesia were not significant predictors of buttoning. It remains unknown whether high-rate repetitive finger movement performance is related to buttoning in people with PD.
To compare the relationship between performance on the Purdue pegboard test and buttoning with repetitive finger movement performance, we had participants with PD complete an acoustically cued repetitive finger movement task at incremental rates from 1 to 3 Hz, a timed buttoning task, and a timed Purdue pegboard assembly task. Because impairments in repetitive finger movements occur at high rates, when people with PD are instructed to tap “as big and fast as possible” during clinical assessment, two movement strategies emerge. They tap either big and slow or fast and small (Espay et al., 2011). Thus, controlling for movement rate and analyzing changes in movement rate and movement amplitude independently help control for individual differences.
Moreover, we posited that the buttoning and Purdue pegboard tasks require different sensory control processing and would be performed at different movement rates. The buttoning task may involve preattentive sensory processes and may be performed at rates greater than 2 Hz. The Purdue pegboard assembly task may involve focal sensory control and may be performed at rates lower than 2 Hz (Kunesch et al., 1989). Thus, given that repetitive finger movement is significantly impaired at high movement rates (>2 Hz; Stegemöller et al., 2009, 2010), we hypothesized that buttoning performance would be significantly correlated with repetitive finger movement performance at tone rates above 2 Hz and that performance on the Purdue pegboard test would significantly correlate with repetitive finger movement performance at tone rates below 2 Hz.
Method
Participants
Data were collected from 46 participants diagnosed with idiopathic PD. Participants had a mean age of 70 ± 9 yr, 24% were male, and 41% were right handed. Participants had a mean disease duration of 8 ± 6 yr, and 23% reported that the right side was the most affected side. Table 1 shows individual participant characteristics. There were no exclusion criteria for this study because the aim was to recruit a diverse population of people with PD. Participants were tested while on antiparkinson medication. All participants gave written informed consent before inclusion in the study, and the Iowa State University institutional review board approved the procedures.
Participant Characteristics
Note. F = female; L = left; M = male; R = right.
Procedure
Repetitive Finger Movement Task.
Participants used the most affected side for the repetitive finger movement task as determined from participant report. Participants were seated comfortably in a chair with elbow flexed at 90° and forearm of the most affected side supported in an arm brace with palm facing downward. Movement was restricted to the index finger by securing the remaining fingers and thumb. Participants completed three trials of an unconstrained index finger flexion–extension (finger tap) movement in synchrony with acoustic tones (50 ms, 500 Hz, 80 dB) presented at a starting rate of 1 Hz with a gradual increase to 3 Hz in increments of 0.25 Hz. Fifteen tones at each rate were presented. Each trial lasted approximately 90 s for a total of 135 finger taps. Three trials were collected. Participants were allowed a practice trial and rest between trials as needed. This task had been used in previous research, and results revealed that medication did not significantly improve movement performance and that peripheral fatigue was not a contributing factor to impaired performance (Stegemöller et al., 2009, 2010, 2013, 2016).
Finger movement was measured with a goniometer and collected using a data acquisition board (Micro 1401, Cambridge Electronic Design, Cambridge, England) and software (Spike2, Cambridge Electronic Design, Cambridge, England). Signals were digitized at a sampling rate of 100 Hz.
Purdue Pegboard Task.
Participants completed three trials of an assembly task on the Purdue pegboard. Using both hands interchangeably, participants assembled four pieces in the following order: pin, washer, collar, washer. This procedure was demonstrated and participants were allowed to practice before data collection began. Participants were allotted 1 min to complete as many bilateral assemblies as possible. Each piece assembled (pin, washer, or collar) yielded a score of 1, with a complete assembly yielding a score of 4.
Buttoning.
For the buttoning task, participants wore a vest with three medium-sized buttons (1.2 cm). Participants started from a neutral position (a hook-and-loop button closure at the top of the vest) and buttoned down the vest as fast as possible using both hands. At the closure of the last button, both hands were placed facing downward on the thighs to signal the stop time. Total time from the neutral start position to hand placement on the thighs was recorded. Participants completed three trials.
Data Analysis
For the repetitive finger tapping task, movement rate was calculated on the basis of the time between each peak displacement (i.e., amplitude). The tone rate was then subtracted from the movement rate to obtain the movement rate difference (MRΔ; Stegemöller et al., 2016). Peak-to-peak amplitude was calculated for each movement, averaged across movements at each tone rate, and normalized to data at 1 Hz. As a measure of variability, the coefficient of variation (CV) was also determined for movement rate by dividing the standard deviation by the mean for each tone rate. MRΔ, peak-to-peak amplitude, and movement rate CV were each averaged for three conditions: (1) across all tone rates (1–3 Hz), (2) tone rates <2 Hz, and (3) tone rates ≥2 Hz.
Statistical Analysis
To evaluate performance on the repetitive finger movement task, a repeated-measures analysis of variance was completed to compare the effect of tone rate on each outcome measure (MRΔ, CV, and amplitude). Post hoc comparisons were completed using paired t tests with Bonferroni correction (eight comparisons, p < .006). Spearman correlations were completed between the fine-motor dexterity outcome measures (buttoning time and number of assemblies) and between the repetitive movement outcome measures (MRΔ, peak-to-peak amplitude, and movement rate CV) to determine whether there was any shared variance between variables. To address the stated hypothesis, partial correlations were completed comparing number of assemblies completed on the Purdue pegboard with MRΔ, peak-to-peak amplitude, and movement rate CV across each averaged condition (all tone rates, tone rate <2 Hz, tone rate ≥2 Hz) while controlling for buttoning time. Partial correlations were also completed for buttoning time with MRΔ, peak-to-peak amplitude, and movement rate CV across each averaged condition while controlling for assembly number.
Results
The mean and standard error for MRΔ, CV, and normalized amplitude from the repetitive movement task are shown in Figure 1. Individual participant data are shown in supplemental material (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). For MRΔ, a value of 0 would indicate that the participant was tapping at the same rate as the intended tone rate. A value >0 indicates that the participant was tapping faster than the intended tone rate, whereas a value <0 would indicate that the participant was tapping more slowly.
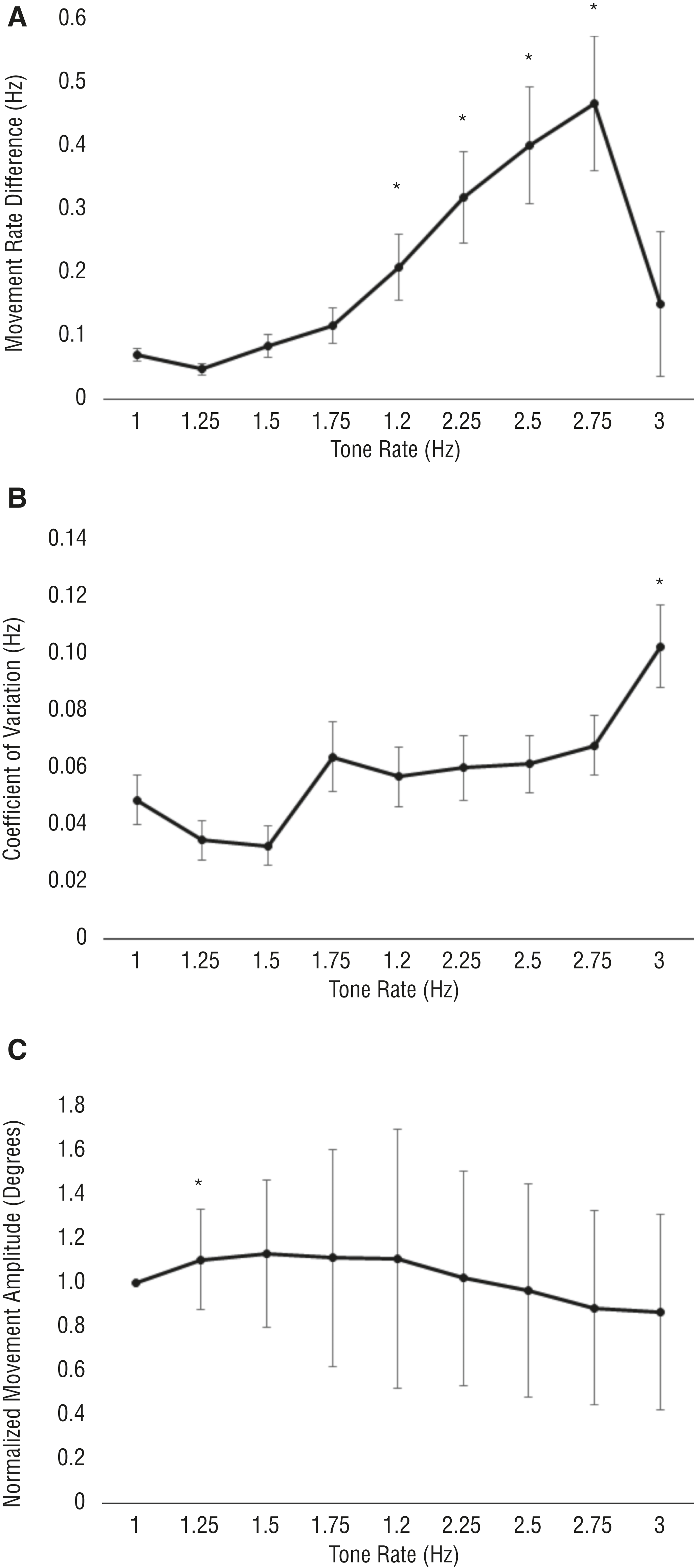
Means and standard errors for movement rate difference (A), coefficient of variation (B), and normalized amplitude (C) across all tone rates for the repetitive finger movement task.
The greater change in mean and standard error for MRΔ occurred around 2 Hz and above. In addition, the increase in CV occurred at ≥1.75 Hz. For normalized amplitude, a value of 1 indicates that the participant was maintaining the same movement amplitude as at the start of the task with the tone rate of 1 Hz. A value >1 indicates that movement amplitude increased, whereas a value <1 indicates that movement amplitude decreased. The mean for amplitude began to drop at 2 Hz and above, and the standard error remained relatively large.
Results revealed a significant effect of tone rate for MRΔ, F(1, 8) = 9.17, p < .001; CV, F(1, 8) = 5.55, p < .001; and normalized amplitude, F(1, 8) = 6.59, p < .001. When comparing MRΔ at 1.0 Hz to the remaining tone rates, post hoc analysis revealed significant differences at 2.0 Hz, 2.25 Hz, 2.5 Hz, and 2.75 Hz, t(45) < −2.86, p < .006. For CV, the only significant difference revealed was at the tone rate of 3 Hz, t(45) = −3.65, p = .001. Post hoc analysis for normalized amplitude revealed a significant difference at 1.25 Hz, t(45) = −3.22, p = .002. These results are in keeping with previous research using this task (Stegemöller et al., 2009, 2010, 2013, 2016).
A significant negative relationship was found between performance on the Purdue pegboard task and buttoning (r = −.62, p < .001). There were no significant associations between the repetitive movement outcome measures (r < −.20, p > .19). Partial correlations between the Purdue pegboard task (controlling for buttoning), buttoning (controlling for the Purdue pegboard task), and the repetitive movement task are shown in Table 2. There were no significant relationships between Purdue pegboard performance and any of the repetitive movement outcome measures. For buttoning performance, significant positive correlations were found for MRΔ and MRΔ CV such that participants who moved faster than the intended tone and with great variability took longer to complete the buttoning task. No significant relationships were revealed between buttoning time and normalized amplitude.
Partial Correlations Between Repetitive Finger Movement Performance and Performance on Fine-Motor Dexterity Tasks
Note. CV = coefficient of variation; Hz = Hertz; MRΔ = movement rate difference.
Significant relationship between variables.
Discussion
The results of this study show that impairments in movement rate across all rates are related to increased difficulty in buttoning. There was no relationship between Purdue pegboard performance and repetitive finger tapping. Given that most neurologists assess disease severity and progression by assessment of repetitive movements, such as finger tapping, and not necessarily functional fine-motor tasks, these results provide insight to help occupational therapy practitioners interpret and determine the impact of Parkinson’s disease on functional fine-motor movement tasks.
Previous research demonstrated a relationship between timed insertion of pegs on the Purdue pegboard and finger tapping (Müller et al., 2000). The results of this study did not reveal a relationship between repetitive finger movement performance and Purdue pegboard performance. The Purdue pegboard task in this study was an assembly task rather than a timed peg insertion task. Thus, additional cognitive components, such as remembering the order of the assembly, may have slowed performance and contributed to the lack of relationship between repetitive finger movement rate and Purdue pegboard task performance. Moreover, the lack of relationship between movement rate and assembly task performance further suggests that bradykinesia may not be correlated with finger dexterity tasks. Indeed, research examining the relationship with other dexterity tasks, such as coin rotation, has shown no correlation with clinical measures of finger bradykinesia (Lee et al., 2010).
In contrast, the results of the current study revealed a relationship between buttoning and movement rate, but not movement amplitude. Previous research demonstrated no relationship between buttoning and clinical assessment of repetitive finger movement (Foki et al., 2016). The clinical assessment of repetitive finger movement is used to assess bradykinesia and does not evaluate movement amplitude and movement rate separately. Previous research using the same repetitive finger movement task as in this study demonstrated that movement rate and amplitude were differentially affected by deep brain stimulation (Stegemöller et al., 2013). Moreover, research has shown that repetitive finger movement performance (i.e., movement rate and amplitude) at high tone rates was not improved with dopaminergic medication (Stegemöller et al., 2009) and was equally present on both sides (Stegemöller et al., 2016). Given that research has demonstrated that bradykinesia is improved with dopaminergic medication and more evident on the most affected side, impairments in repetitive finger movement rate may represent other dysfunctions associated with PD, such as festination (hastening) or hesitation. Festination or hesitation may better explain the relationship between buttoning and repetitive finger movement performance.
Both limb kinetic apraxia (i.e., loss of ability to make precise, independent but coordinated finger movement) and higher order sensory dysfunction have been suggested as contributors to impairments in finger dexterity in people with PD, rather than bradykinesia (Foki et al., 2016; Gebhardt et al., 2008; Hill et al., 2010; Lee et al., 2010). Although performance on the Purdue pegboard and buttoning tasks was highly related in this study, suggesting that a common mechanism may contribute to impairments in both, separate analysis of movement rate and movement amplitude may suggest that separate underlying mechanisms may contribute to impairment in these tasks. For a task that requires greater precision and reliance on sensory information, such as the assembly task on the Purdue pegboard, higher order sensory dysfunction may be a primary contributor to impairments in this task. Impairments in tactile discrimination may lead to changes in the scaling of the motor output that are not evident in the repetitive finger movement task.
In contrast, for tasks that are faster and more automatic, such as buttoning, limb kinetic apraxia may be a primary contributor. Festination and hesitations present during repetitive finger movement may also be a contributing factor to limb kinetic apraxia. Thus, limb kinetic apraxia may explain the relationship between buttoning and movement rate. However, movement kinematics were not collected during the Purdue pegboard and buttoning tasks in this study. Further research is needed to determine whether differing mechanisms indeed contribute to the varying results of fine-motor dexterity studies with people with PD.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Repetitive finger movements are often used during the clinical assessment of PD. People with PD use different strategies to perform repetitive finger movements; they may tap either big and slow or fast and small.
Differences in repetitive movement performance strategy may provide information regarding impairments in fine-motor dexterity tasks. People who move fast and small, demonstrating difficulty in controlling movement rate, may have greater difficulty in fast fine-motor dexterity tasks such as buttoning.
Understanding differences in performance during assessment may aid practitioners in developing a more effective treatment plan.
Continued research is needed to determine the relationship between repetitive finger movement performance and additional fine-motor dexterity tasks, such as using eating utensils and handwriting.
Limitations
The lack of exclusion criteria may have increased the variance in performance across participants, decreasing the overall relationship between tasks. Indeed, the correlation between movement rate and buttoning, though significant, was small. Participants were tested on the most affected side for the finger tapping task, whereas both the buttoning and Purdue pegboard tasks involved both hands. Although previous research has shown that performance on the repetitive movement task in this study does not differ between sides (Stegemöller et al., 2016), it is unknown whether differences between sides influenced buttoning and Purdue pegboard performance in this study.
Participants were tested on medication. Although medication state does not affect the impairment of repetitive finger movement at rates near to and above 2 Hz (Stegemöller et al., 2009), the effects of medication may have contributed to better motor performance on the buttoning and Purdue pegboard tasks, reducing the significance of associations. Clinical data on participants, such as the UPDRS score, were lacking; correlation of motor performance on the fine-motor tasks with scores on the motor section of the UPDRS would be beneficial in clarifying the relationship between subjective and quantitative assessment of motor function in people with PD.
Conclusion
This pilot study demonstrated that changes in movement rate and movement amplitude during the performance of repetitive finger movement tasks have differential relationships to performance of fine-motor dexterity tasks in people with PD. Differing motor control mechanisms may contribute to impaired fine-motor dexterity. Further detailed examination of movement kinematics may provide more information and aid in the treatment of people with PD.
Supplemental Material
Supplementary material for Repetitive Finger Movement and Dexterity Tasks in People With Parkinson’s Disease
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.028738.pdf for Repetitive Finger Movement and Dexterity Tasks in People With Parkinson’s Disease by Jennifer C. Uzochukwu and Elizabeth L. Stegemöller in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.