
Abstract
By 2050, 13.8 million Americans will be living with dementia, most being cared for by family members (Alzheimer’s Association, 2016). A key clinical feature of dementia is neuropsychiatric behaviors such as agitation, aggression, and rejection of care. The behavioral and psychological symptoms of dementia (BPSD) affect most persons with dementia, occur throughout the disease process, and are associated with nursing home placement, hospitalization, decreased quality of life, and increased morbidity and mortality (Gitlin et al., 2012; Miyamoto et al., 2010). In addition, for caregivers, the presence of BPSD is associated with caregiver burden (Matsumoto et al., 2007), increased depression and stress, and decreased quality of life (Gitlin et al., 2012).
Although psychotropic medications are often used to manage BPSD, they have shown only modest benefit along with increased risk for adverse outcomes. Leading medical organizations and expert groups recommend nonpharmacological approaches as first-line treatment (Gitlin et al., 2012). One promising nonpharmacological approach is use of activity tailored to the person’s interests, abilities, and physical and social environment. New Ways for Better Days: Tailoring Activities for Persons With Dementia and Their Caregivers (TAP) is an evidence-based program drawing on occupational therapy principles including activity analysis and simplification, person-centered care, problem solving, and person–environment–occupation fit (Gitlin et al., 2016; Piersol & Jensen, 2017).
In this article, we illustrate the importance of occupational therapists in dementia care by presenting a case report describing the TAP protocol, the clinical reasoning processes used, and outcomes of activity engagement related to BPSD. We asked these research questions: Does TAP increase caregiver confidence in using activities? Does activity use increase engagement over time for persons with dementia?
Method
This case report is drawn from a randomized clinical trial testing the efficacy of TAP compared with attention control to reduce BPSD (Gitlin et al., 2016). The study was approved by the Johns Hopkins Medicine institutional review board.
TAP Program
TAP draws on a person–environment–occupation framework. It addresses BPSD by providing structured activities of intrinsic interest that are tailored to the preserved capabilities of persons with dementia and that realign environmental expectations with capacity. This approach departs from traditional medical care and rehabilitation, which focus on cure or remediation. In TAP, occupational therapists evaluate persons with dementia, caregivers, and living environments; develop activity prescriptions tailored to the person’s capacities; and teach caregivers to implement the prescriptions. Caregivers learn to manage their situational distress; optimize function; and prevent, reduce, or manage BPSD that may be a consequence of person–environment mismatches and inappropriate expectations (Gitlin et al., 2016). The approach assumes that reducing BPSD results in better quality of life for caregivers and persons with dementia.
As described elsewhere (Gitlin et al., 2009, 2016), TAP involves up to eight home sessions occurring within 3 mo. Sessions unfold in three phases. In Phase 1, assessment (Sessions 1–2), the occupational therapist uses standardized assessments (listed in Table 1) to evaluate the person with dementia, caregiver, and environment. On the basis of findings, the therapist collaborates with the caregiver (and person with dementia when possible) to identify three activities of interest that are then tailored to the capabilities and context of the person with dementia (Figure 1). Caregivers are educated about disease processes and BPSD and learn simple stress reduction techniques to manage their upset.
Assessments Administered in the Case Study
Note. ADLs = activities of daily living; BPSD = behavioral and psychological symptoms of dementia; IADLs = instrumental activities of daily living; TAP = New Ways for Better Days: Tailoring Activities for Persons With Dementia and Their Caregivers.

Simplified Decision Matrix for Tailored Activity Selection.
In Phase 2, implementation (Sessions 3–6), the occupational therapist reviews assessment results with the caregiver and provides three activity prescriptions, which describe the activity, goal, person’s abilities, and implementation steps. The therapist then demonstrates for the caregiver how to set up and implement the activities, after which the caregiver practices strategies. On the basis of skilled observation, the therapist modifies the prescriptions as necessary. The caregiver continues to practice activity prescriptions with the person with dementia between sessions.
In Phase 3, generalization (Sessions 7–8), the occupational therapist helps the caregiver identify ways to simplify the activities as the disease progresses. The therapist also helps the caregiver brainstorm ways to generalize activity strategies to other care challenges (e.g., bathing), such as by simplifying communications and modifying the environment.
Measures
In addition to the standardized assessments used in Phase 1 (see Table 1), several investigator-designed forms are used to measure how the caregiver and person with dementia accept and use activities.
Delivery Assessment Form.
The Delivery Assessment Form is a brief form completed at the conclusion of each session. The occupational therapist records dose and intensity and reflections on the session, including the acceptance and enactment of activities provided and engagement level of the person with dementia.
Confidence Rating Form.
On the Confidence Rating Form, the caregiver rates his or her level of confidence and willingness to do each of the activities. Rated on a scale of 0 (not at all confident/not at all willing) to 10 (extremely confident/extremely willing), these two items are completed after each activity is introduced and again at the final session.
Activity Record.
The Activity Record is completed in the session after an activity is introduced and is used to assess the frequency of activity use by the caregiver and the reaction of the person with dementia.
Caregiver Readiness.
Readiness to implement TAP strategies is based on the Transtheoretical Model’s stages of change (precontemplation, contemplation, preparation, and action/maintenance; Prochaska & DiClemente, 1983). It is scored on a 4-point scale on the basis of the occupational therapist’s observations and interactions with the caregiver during the first two sessions. Readiness is again scored at the final session.
Environmental Assessment Form.
The environment (room or area of room) in which each activity will take place is assessed for both ease of performance and safety. The occupational therapist uses a yes–no checklist to examine eight areas of the environment for each activity (layout, flooring, lighting, work area, seating, appliances, manual tools, and other, such as temperature and presence of others). If any issues are found, the occupational therapist notes whether a change to the environment or activity is necessary.
Case Description
Sara, a single African-American woman in her 60s, cares for her father, Lee, age 92, who has severe dementia and mobility limitations (pseudonyms are used to preserve confidentiality). Sara, though not living with Lee, identifies as his primary caregiver. Multiple other family members live with and care for Lee. Sara has a full-time demanding job and was overwhelmed by her multiple responsibilities.
Phase 1: Assessment
Lee’s BPSD included irritability, agitation, and verbal aggression (yelling and being argumentative). Lee’s Allen Cognitive Level of 3.4 indicated that he was able to use his hands and arms to grasp and release objects, engage in familiar repetitive actions, and follow simple verbal instructions (Allen et al., 2007; Earhart, 2006). A score of 2 min and 31 s on the Timed Up and Go indicated that Lee had poor mobility and was at high fall risk. Lee was moderately to completely dependent in activities of daily living. Observation of social behavior (Peavy et al., 1996) showed that Lee was socially appropriate (e.g., good eye contact, shakes hand), although he often yelled inappropriately or turned his back on others. He enjoyed being with family and was cooperative when effectively engaged. Lee was previously a deacon and enjoyed listening to sermons and gospel music. Other interests included baseball, spending time with his great-grandson, and petting and watching animals.
Sara used some positive management strategies, including diverting Lee’s attention when he became upset and putting needed items in his sight. However, she also used negative communication techniques, including raising her voice, criticizing, and threatening him with negative consequences (e.g., turning off the space heater) if Lee did not comply with her demands. Also, she would attempt to reason with him, telling him he was wrong and arguing with him. For example, he frequently asked to go to work and meet with friends. Sara would typically yell, informing him that he had not worked for more than 30 yr and that he no longer had work buddies.
Sara believed that her father had more capacity than he did and that his yelling was purposeful and intended to annoy her. She had previously tried activities but did not find them helpful or engaging. The home environment was noisy and cluttered, the television was constantly blaring, and family members’ comings and goings appeared chaotic.
Given Sara’s fundamental misunderstanding of dementia and BPSD, belief that nothing would help, and lack of understanding about Lee’s need for appropriate social engagement and activity, the occupational therapist rated her stage of readiness to implement activity strategies as precontemplation, indicating that Sara was not ready to implement TAP strategies, was unaware of the need for change, and did not understand that a problem existed. Sara expressed being overwhelmed, not knowing what to do, and having poor quality of life.
Phase 2: Implementation
With Sara’s input on Lee’s activity interests and prior roles, the occupational therapist identified three activities to implement: listening to gospel music, watching animal shows, and tossing a ball with family members. For each activity, the therapist developed an activity prescription that matched activity demands with Lee’s current abilities (cognitive, physical, social). The activity prescription included suggested time of day and frequency of activity use, Lee’s abilities, and strategies for setting up the environment, simplifying the activity, and communicating effectively to enhance Lee’s participation. Stress reduction strategies were included for Sara to take care of herself.
For each activity, the environment was set up to optimize Lee’s engagement. One strategy to limit auditory commotion was to have Lee use earbuds to listen to music. The animal show activity was implemented in a less cluttered room to minimize distractions. The ball toss activity, however, was conducted in a common area to include other family members, which enhanced enjoyment for Lee and his family.
Lee enjoyed the activities and engaged with each. At the completion of the eight sessions of the intervention, Sara reported improved confidence in her ability and willingness to use activities (Table 2). Her initial confidence with the ball toss activity was 5 of 10 (moderately confident). By Session 8, she rated her confidence as 8. The occupational therapist in turn rated Sara as having “a little” understanding of strategies during the first session and as having “moderate” understanding by Session 8. Sara’s use of effective communication techniques improved, along with her readiness to implement strategies from rejecting suggestions (precontemplation) to embracing new care strategies (contemplation). Sara reported being more patient with her father and feeling less stressed.
Assessment Results Showing the Impact of the TAP Program on the Caregiver in the Case Study
Note. TAP = New Ways for Better Days: Tailoring Activities for Persons With Dementia and Their Caregivers.
Rated on a 5-point scale: 0 = not at all, 1 = a little, 2 = moderately, 3 = very much, and 4 = extremely.
Changes were also observed in Lee. During Sessions 1 and 2, the occupational therapist estimated moderate engagement because he spent about 50% of the time actively engaged. During each activity introduced, Lee’s engagement level increased to extremely engaged (about 100% of time; Figure 2). Sara reported that her father did not yell when listening to gospel music; rather, he moved his head to the music and listened to it for an hour. This freed her to do things around the home or rest. Sara reported using the activities almost daily.
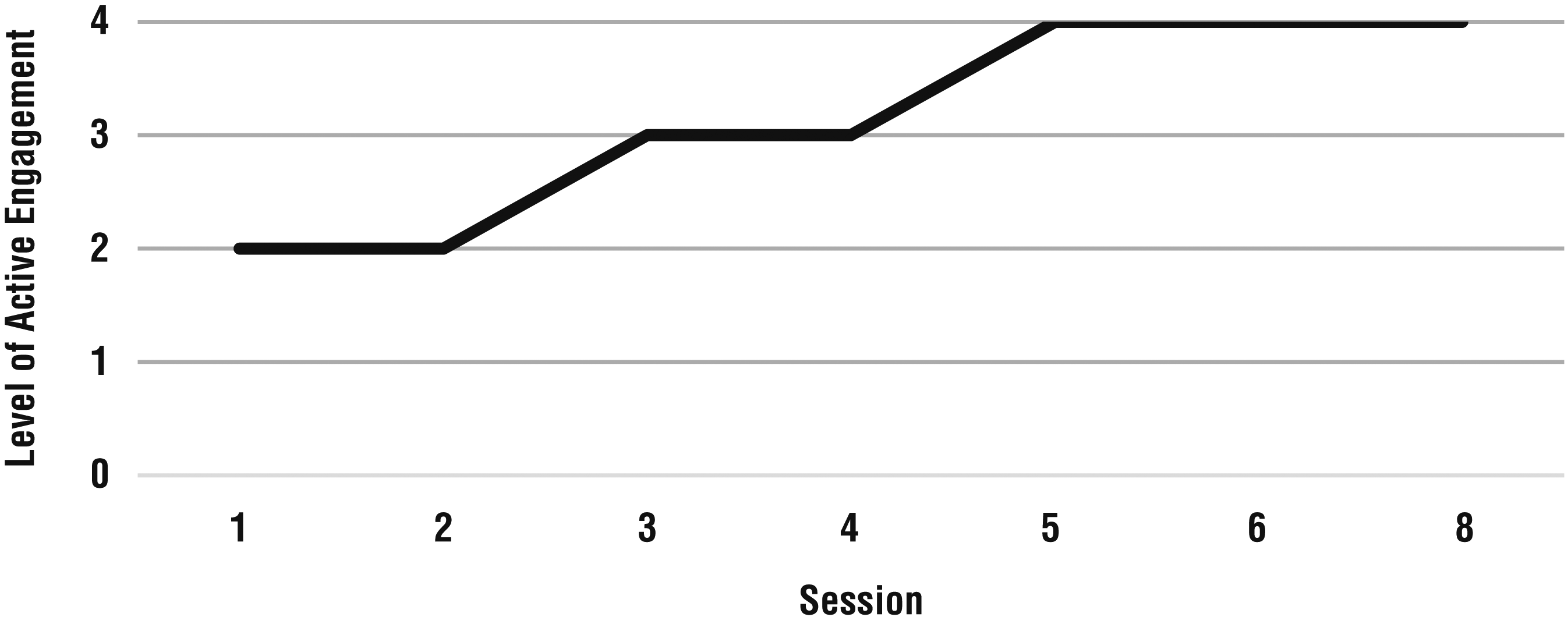
Lee’s level of active engagement during participation in the TAP program, as observed by the occupational therapist.
Phase 3: Generalization
During the final two sessions, the occupational therapist helped Sara identify ways to simplify the three activities as Lee declined and to apply strategies learned for activity implementation to other daily care challenges. During this process, the therapist used brainstorming to engage Sara and support her independent generation of strategies. The goal of this phase was for Sara to be able to problem solve and generate strategies independently, preparing her for being on her own after the intervention.
During brainstorming, the occupational therapist offered simplification strategies for the first two activities. For the third activity, listening to music, Sara was able to independently identify strategies to simplify the activity, such as using a different CD with a slower melody or spending less time in the activity. A care challenge Sara described was Lee’s difficulty feeding himself and not following her directions. Together, the therapist and Sara identified strategies from the activity prescriptions that could address this challenge. These included simplifying the activity using finger foods on a white plate placed on a dark placemat and using one-step directions, such as “Dad, eat your chicken nuggets.”
Discussion
This case report illustrates how occupational therapists work with families using the TAP protocol to help them manage BPSD by tailoring activities. Achieving the just-right fit among person, caregiver, environment, and activity or occupation requires complex clinical reasoning—most prominently, interactive and conditional reasoning.
Interactive reasoning focuses on understanding the client as a person, including his or her preferences, interests, and motivations, and applying that understanding to treatment approaches (Fleming, 1991). Interactive reasoning was reflected in the occupational therapist’s recognition of Sara’s distress, her misunderstandings of BPSD, and the family dynamics. The therapist did not minimize Sara’s distress and showed empathy. The therapist provided education at an appropriate level for Sara to understand, teaching Sara that her father’s behaviors were not intentional but rather a disease symptom.
The occupational therapist worked with Sara to identify activities that would be of interest to Lee yet appropriate for Sara to implement. The therapist demonstrated each activity, modeled effective communication, and asked Sara to reflect on what worked and what did not, valuing and respecting Sara’s input. On the basis of assessment findings and continuous reflection on the care environment, the therapist worked to reduce Sara’s caregiver stress and improve her knowledge, use of communication and simplification strategies, and ability to use activities in daily care routines. The therapist did this through demonstration and explanation and by including Sara in problem solving, brainstorming, and strategy generation.
Conditional reasoning focuses on envisioning future contexts for the client and applies experience with similar situations and clients to refine treatment to match current and future contexts (Fleming, 1991). The occupational therapist used conditional reasoning when guiding the selection and implementation of activities. The therapist learned that Sara was stressed and unsuccessfully using activities. Sara’s negative communication was a critical observation combined with her being overwhelmed and needing immediate strategies to manage her own upset.
The therapist demonstrated how and why tailoring activities to Lee’s interests and current abilities was possible and effective. The therapist made ongoing observations of the environment, noting various visual and auditory distractions for Lee. Strategies such as using earbuds and incorporating family members in activities were offered to offset the negative impact of environmental press and promote engagement. At the conclusion of TAP, Sara reported that Lee displayed reduced behavioral disturbances, particularly yelling and repetitive questioning.
Implications for Occupational Therapy Practice
Results of this case report suggest the following implications for occupational therapy practice in dementia care:
A person–environment–occupation framework that considers the preserved capacities of the person with dementia, the caregiver’s level of readiness to implement strategies, and environmental factors offers a structure from which to design and tailor activities for persons with dementia.
Standardized assessments of persons with dementia, caregivers, and environments and a decision tree in which interests, abilities, caregiver readiness to implement strategies, and environmental features are considered provide the basis for designing activities that tap into preserved capacities and promote meaningful engagement.
Occupational therapists serve as consultants in TAP, guiding caregivers and persons with dementia through the use of meaningful activities to manage BPSD.
Activity is a therapeutic modality through which caregivers learn how to effectively interact with persons with dementia and realign their own expectations with the person’s capacity.
Conclusion
This case report underscores the importance of a structured protocol for tailoring activities and training caregivers in their use and describes some of the challenges. Occupational therapists are uniquely qualified to systematically assess the cognitive functioning of persons with dementia, caregivers, and home environments and to integrate this information to derive and implement activities tailored to the person’s capacities and context to achieve a just-right fit, thus reducing BPSD (Fraker et al., 2014). TAP can be implemented in conjunction with other occupational therapy interventions or dementia care programs, or it can be delivered as a stand-alone consultation service.