
Abstract
Autism spectrum disorder (ASD), a diagnosis estimated to affect 1 in 68 children in the United States, affects social communication and results in repetitive and restrictive behaviors (American Psychiatric Association, 2013; Christensen et al., 2016). Core and associated characteristics of ASD affect occupational performance in many areas for both children and families. Social communication (i.e., sharing, positive affect, conversation, receptive language) is particularly challenging for children with ASD (Bauminger et al., 2008). As a result of these deficits, children with ASD often have difficulty forming peer relationships (Lasgaard et al., 2010). Difficulties with social participation and friendships are further complicated by the differences in play observed in children with ASD.
Play is an essential occupation of childhood from which children develop language, self-regulation, and problem-solving skills (Lifter et al., 2011). Parents have reported that children with ASD engage in more repetitive behaviors and less play than typically developing peers (Honey et al., 2007). From an early age, children with ASD are extremely preoccupied with objects and use them in unusual ways (Williams, 2003). In addition, children with ASD explore sensory aspects of objects past the age of typically developing children (Williams, 2003) and spend less time engaged in pretend play than both typical peers and children with other developmental disorders (Rutherford & Rogers, 2003).
Performance of self-care and daily living tasks are essential to child independence but are often delayed in children with ASD compared with age-matched peers (Bal et al., 2015; Jasmin et al., 2009). Examples of skills that are particularly difficult to master include toileting, dressing, personal hygiene, and eating. Research suggests that parents of children with ASD who have increased caregiving responsibilities experience higher subjective stress and lower family quality of life (Hoefman et al., 2014; Khanna et al., 2011). Delayed self-care and daily living skills affect not only child outcomes but also caregiver well-being.
Early and intensive intervention addressing the previously mentioned concerns results in the best outcomes for children with ASD (Lord & McGee, 2001; Orinstein et al., 2014). Intervention services based on a variety of theoretical frameworks are delivered in many settings, including clinics, schools, and the home (Boyd et al., 2010; Warren et al., 2011). These services are often expensive, are not covered by insurance, or have transportation barriers (Chiri & Warfield, 2012; Croen et al., 2006). Given the barriers to accessing early intervention services provided by trained therapists, effective and evidence-based alternatives are essential; parents are optimally situated to support their children in these early years. Compared with therapist-led interventions, parent-led interventions are less expensive, increase generalization of learning across environments, and are associated with improved skill maintenance over time; however, they may be considered more time intensive for parents (Brookman-Frazee et al., 2009).
Parent-mediated interventions engage parents in the role of therapist to implement interventions with their children (Oono et al., 2013). Implementation of parent-mediated interventions consists of three steps: identifying potential interventions; teaching parents how to implement the intervention; and continuing collaboration between parents and practitioners, with practitioners providing feedback to parents (Boyd et al., 2010). Training specifics vary on the basis of outcomes targeted by the intervention. Research has primarily focused on parent-mediated interventions for young children with ASD that target social interaction (e.g., Kasari et al., 2015).
To better understand the efficacy of parent-mediated interventions supporting this population, Oono et al. (2013) completed a systematic review of the literature. The review included randomized controlled trials (RCTs) of parent-mediated early interventions conducted in the United States, the United Kingdom, Australia, Canada, Thailand, and China with children ages 1–7 yr. Results of the review were mixed, with moderate evidence supporting improvements in aspects of parent–child interaction and autism symptom severity but insufficient evidence supporting improvements in behavior, language, and social communication (Oono et al., 2013). After completion of a meta-analysis on a subset of the studies (n = 11), Oono et al. found a statistically significant improvement in parent–child interactions, including shared attention, and reduction in autism symptom severity.
Generalizability of the results of the study completed by Oono et al. (2013) is limited for several reasons. First, Oono et al. did not limit their review to traditional parent-mediated interventions but rather included a range of interventions that involved parents, such as group parent education. In addition, the review included studies conducted outside the United States. Parenting children with developmental disabilities is heavily culturally influenced (Marquis & Baker, 2014), so the generalizability of the results of this review to the United States may be limited. Finally, most studies included in the review primarily focused on social interaction. Although this skill is important, an essential need exists to better understand the potential of traditional parent-mediated intervention to improve a wider variety of skills that affect a child’s occupational performance and participation.
The purpose of this systematic review is to evaluate the evidence for the effectiveness of parent-mediated interventions on the occupational performance of children with ASD. As parent-mediated interventions increase, research evaluating their effectiveness with a broader range of outcomes is essential. In addition, by studying clearly defined interventions (e.g., traditional parent-mediated intervention vs. group parent training), we increase the likelihood of matching specific interventions with targeted outcomes to optimize participation for children with ASD and their families.
Method
We conducted a systematic search of the literature through March 2017 using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009) guidelines to find articles evaluating the effectiveness of parent-mediated interventions on occupational performance of children with ASD. Three databases were systematically searched, including MEDLINE–PubMed, CINAHL Plus (including ERIC, PsycARTICLES, PsycINFO, SocINDEX, Social Sciences), and OTseeker, for relevant articles published since September 2005 in addition to relevant reference lists. Variations of keywords related to parenting, intervention, and autism spectrum disorder were used to search all three databases, including relevant filters for humans, English language, and age. For example, the MEDLINE–PubMed search included the following keywords: (“parent” OR “coach*” OR “mediat*” OR “caregive*”) AND (“intervention” OR “treatment” OR “therapy”) AND (“autis*” OR “autism spectrum disorder” OR “pervasive developmental disorder” OR “Asperger” OR “ASD”). This search also had the following filters: “humans”; “English language”; and “child: 1–18 yr,” “preschool child: 2–5 yr,” “child: 6–12 yr,” and “adolescent: 13–18 yr.”
The inclusion criteria were that the study must include an intervention that met the definition of parent-mediated intervention and the child (age 18 yr or younger) must have a diagnosis of ASD. Parent-mediated interventions required the existence of a parent–child–interventionist triad. Key intervention components included modeling of strategies, parent coaching, provision of feedback, and individualization of the intervention strategies. Studies that included only parent education and training, participants with co-occurring diagnoses, or children at risk for ASD or a provisional diagnosis were excluded, as were studies published before September 2005. We excluded studies conducted outside of the United States because of predicted cultural influences on parenting practices and occupational outcomes (Marquis & Baker, 2014).
After duplicates were removed, articles were first screened by title, then abstract, and finally full-text review by two independent reviewers. Discrepancies that required further attention were reviewed by a third and fourth research team member and discussed as needed. Research team members included three graduate students and a university faculty member. Levels of evidence were assigned on the basis of American Occupational Therapy Association (AOTA) guidelines; articles at Level III or higher were included for analysis (AOTA, 2017). If studies contained multiple designs, results were only reported for designs meeting the criterion Level III or higher. Figure 1, a flow diagram, shows the process used to identify and select studies for review.
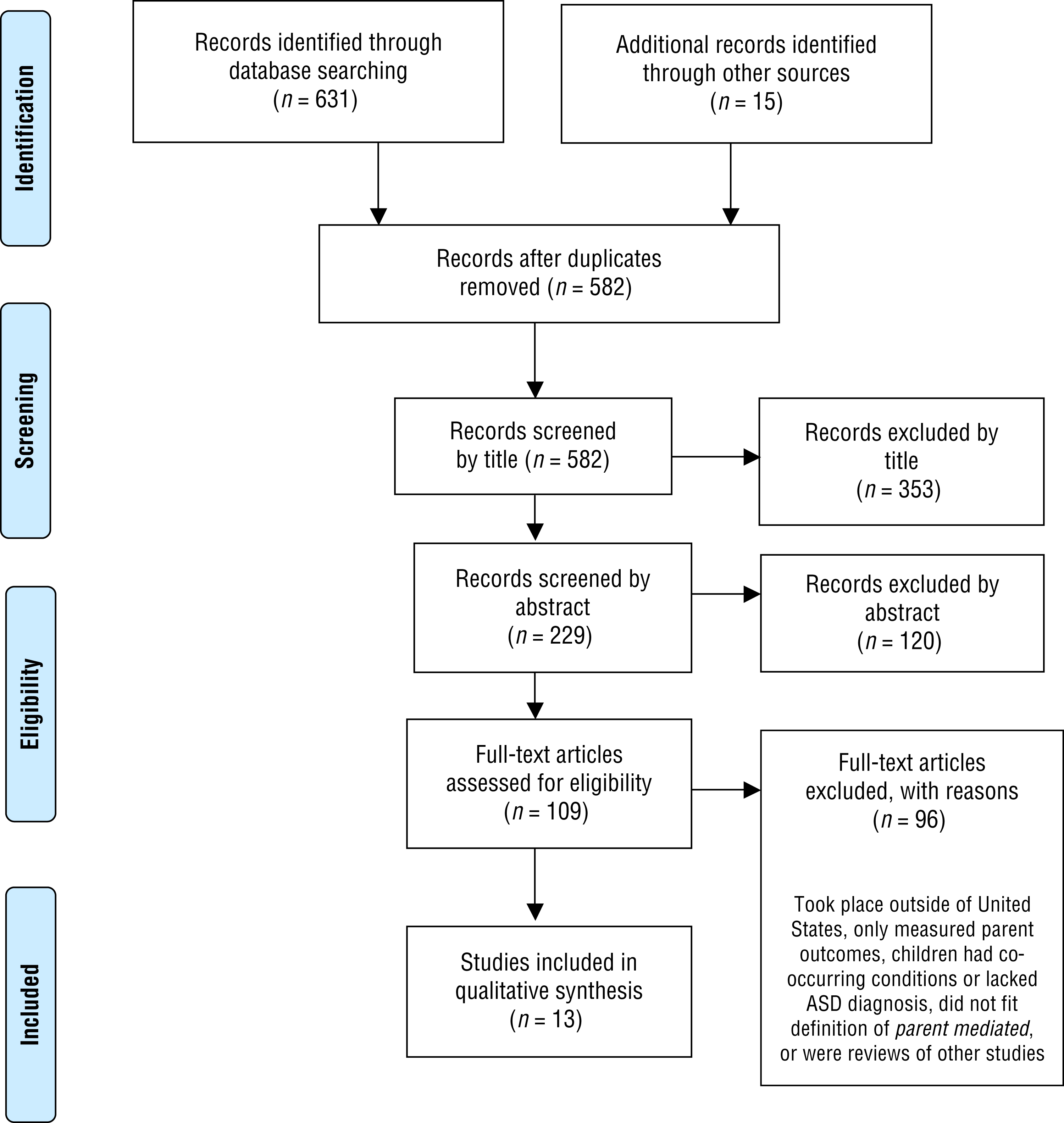
Flow diagram for inclusion and exclusion process of peer-reviewed studies.
Results
The systematic review search identified 582 unique articles. After screening title and abstracts, 109 articles remained for full-text review, and 13 met the inclusion and exclusion criteria. Twelve articles were evidence Level I, and 1 article was evidence Level III. Only 2 of the studies identified by Oono et al. (2013) for their systematic review also met the inclusion criteria for this systematic review (Kasari et al., 2010; Silva et al., 2011). The remaining articles were excluded because interventions either did not meet our definition of parent-mediated intervention or occurred outside of the United States.
Studies included in this review were organized by outcome area, including communication, behavior, play, adaptive functioning, and autism symptom severity. Categories were not mutually exclusive; therefore, articles that addressed several outcome areas were included in multiple categories. Categories were each assigned a strength of evidence ranging from insufficient to strong as outlined by AOTA (2017) in its guidelines for systematic reviews and on the basis of U.S. Preventive Services Task Force (2016) recommendations. For example, strong evidence includes consistent results from a minimum of 2 high-quality RCTs, and moderate evidence includes evidence from a minimum of 1 well-conducted RCT or at least 2 other lower level studies. For further information on strength of evidence, refer to AOTA (2017).
Interventions occurred in a wide variety of settings and differed in administration protocol. A total of 835 participants were included across studies. Studies occurred in the home (n = 4), clinic or laboratory (n = 6), or via telehealth (n = 1), or they used a combination of service delivery methods (n = 2). Studies varied in intensity and length, with durations ranging from 7 wk to 12 mo. Studies chosen for inclusion are summarized in Supplemental Table 1, placed at the end of this article. Although 12 studies were RCTs, many did not adequately describe the process of randomization or allocation, resulting in unclear or high risk of selection bias. None of the articles included blinding of the participants or the interventionists administering the interventions. In addition, 4 studies relied completely on patient-reported outcomes. Further examination of the risk of bias for the studies can be found in Table 1.
Risk-of-Bias Analysis for Intervention Studies Included in the Review of Parent-Mediated Interventions for Children With Autism Spectrum Disorder
Note. Categories for risk of bias are as follows: + = low risk of bias; ? = unclear risk of bias; − = high risk of bias. N/A = not applicable because of study design. Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), by J. P. T. Higgins and S. Green (Eds.), 2011, London: Cochrane Collaboration. Retrieved from http://handbook-5-1.cochrane.org. Copyright © 2011 by The Cochrane Collaboration.
Communication
Eleven studies reported an outcome related to various aspects of communication, including language, nonverbal communication, joint attention and engagement, and initiation and response to interaction. Several measures, including standardized assessments, parent report, and video coding, were used to evaluate child progress.
Language.
Seven studies measured language outcomes (including receptive, expressive, and spontaneous use). Moderate evidence from 3 Level I studies (RCTs) indicates that parent-mediated interventions improve communication as measured by the Vineland Adaptive Behavior Scales, Second Edition (VABS–II; Sparrow et al., 2005). Two of these studies showed improvement in the treatment group compared with the control group, whereas 1 found no difference between groups. Wetherby et al. (2014) compared the effects of an individual parent-mediated Social Communication, Emotional Regulation, and Transactional Supports (SCERTS; Prizant et al., 2006) intervention with those of a group SCERTS intervention. Considerable improvements were found in the Communication domain of the VABS–II among children in the parent-mediated intervention versus the comparison group. Schertz et al. (2013) examined the effects of a Joint Attention Mediated Learning (JAML; Schertz et al.; 2013) intervention conducted in the home. Compared with the control group, children who received the JAML intervention displayed significant increases in VABS–II Communication scores. In the final study, Ingersoll et al. (2016) compared the parent-mediated Improving Mood—Promoting Access to Collaborative Treatment (ImPACT; Schreibman et al., 2015) telehealth intervention with a similar intervention without therapist feedback. Improvements in the Communication domain of the VABS–II were observed in both groups, with no notable difference between groups.
Related to receptive language, mixed evidence from 4 Level I studies (RCTs) indicates that parent-mediated interventions may be beneficial. In 2 studies, children in parent-mediated groups displayed increased receptive language scores compared with the control group, although various measures were used (Schertz et al., 2013; Wetherby et al., 2014). However, the remaining studies, which used different types of primary interventions, found that children in both the intervention and the control groups displayed similar increases in receptive language measures (Kasari et al., 2015; Welterlin et al., 2012). One RCT used the Joint Attention, Symbolic Play, Engagement, and Regulation (JASPER) model (Kasari et al., 2015), and the other assessed the home Treatment and Education of Autistic and Related Communication-Handicapped Children (TEACCH; Mesibov et al., 2005) program (Welterlin et al., 2012).
Moderate evidence from 5 Level I studies (RCTs) suggests that that parent-mediated interventions improve expressive language, although not necessarily more effectively than other forms of intervention. Three studies found improvements in expressive language as measured by the Mullen Scales of Early Learning (MSEL; Mullen, 1995), Scales of Independent Behavior—Revised (SIB–R; Bruininks et al., 1996), or Reynell Developmental Language Scale (Reynell & Curwen, 1977) but no notable differences between groups (Kasari et al., 2015; Welterlin et al., 2012; Wetherby et al., 2014). An RCT exploring the effectiveness of the parent-mediated Play and Language for Autistic Youngsters (PLAY) Project Home Consultation model (Solomon et al., 2007) compared with usual community services found that both groups improved on the Words Produced and Words and Sentences subdomains of the MacArthur Communicative Development Inventory (Fenson et al., 2007) with no notable differences between groups (Solomon et al., 2014). Ingersoll et al. (2016) found a similar pattern of improvement on the Words and Sentences subdomain.
Insufficient evidence from 2 Level I studies (RCTs) indicates that parent-mediated interventions may not effectively improve child spontaneous language. Venker et al. (2012) compared the effectiveness of an adapted More Than Words program (Sussman, 1999) with delayed treatment. They found that more children in the intervention group increased spontaneous communication, with no notable differences between groups. Ingersoll et al. (2016) found considerable gains in spontaneous language in both the therapist-assisted and self-directed groups, with no notable difference between groups at posttreatment or follow-up.
Nonverbal Communication.
Moderate evidence from 4 Level I studies (RCTs) suggests that that parent-mediated interventions may improve nonverbal communication, although not more effectively than other interventions. Two studies found improvements in gestures, although neither found a notable difference between groups (Ingersoll et al., 2016; Solomon et al., 2014). Wetherby et al. (2014) found no notable differences between groups on MSEL measures of nonverbal skills. The remaining study found no notable difference in video-coded measures of spontaneous nonverbal communication between the intervention and delayed treatment groups (Venker et al., 2012).
Joint Attention and Engagement.
Mixed evidence from 4 Level I studies (RCTs) indicates that parent-mediated interventions may increase child initiation of and responsiveness to joint attention. Three RCTs found that parent-mediated interventions had no considerable impact on initiation of joint attention compared with a comparison intervention or control group (Kasari et al., 2010, 2015; Schertz et al., 2013). One RCT found that both a caregiver education intervention and a parent-mediated intervention increased initiation of joint attention, which remained at 3-mo follow-up, and the parent-mediated group experienced a faster rate of increase (Kasari et al., 2014). Two RCTs reported an increase in child responsiveness to joint attention after parent-mediated interventions (Kasari et al., 2010; Schertz et al., 2013). The increase remained at 4- and 8-wk (Schertz et al., 2013) and 1-yr (Kasari et al., 2010) follow-ups.
Strong evidence from 4 Level I studies (RCTs) suggests that parent-mediated interventions improve child joint engagement. Kasari et al. (2010) found that children who received JASPER parent-mediated intervention participated in significantly more joint engagement and less object-focused play than the waitlist group, but the difference was not maintained at 1-yr follow-up. In 2 separate follow-up studies, the same research group found that children in the JASPER parent-mediated group had significantly greater improvements in joint engagement duration, which were maintained at 3-mo (Kasari et al., 2014) and 6-mo (Kasari et al., 2015) follow-ups. Shire et al. (2015) also followed the JASPER protocol and found that the mean time spent jointly engaged increased throughout their study period, decreased at 3-mo follow-up, but still remained higher than baseline.
Initiation and Response to Interaction.
Moderate evidence from 2 Level I studies (RCTs) indicates that parent-mediated interventions increase child initiation and response to interaction. Solomon et al. (2014) found that parent-mediated intervention in addition to usual community services significantly increased child attention and initiation compared with usual community services alone. Venker et al. (2012) found that children significantly increased prompted communication acts compared with the control group.
Behavior
Moderate evidence from 2 studies (Levels I and III) supports the use of parent-mediated interventions to decrease behavioral challenges for children with ASD. An intervention that used a parent-mediated approach, compared with parent education, found decreases in irritability and noncompliant behaviors (Bearss et al., 2013). After a behaviorally based play therapy intervention, Zlomke et al. (2017) reported a decrease in frequency of disruptive behaviors, hyperactivity, aggression, and atypical behaviors as well as an increase in child compliance.
Play
Moderate evidence from 3 Level I studies (RCTs) shows improvements in play skills; however, the evidence is mixed regarding increases in functional or symbolic play. In 3 studies using different samples, Kasari et al. (2010, 2014, 2015) focused on functional and symbolic play skills. The first study (Kasari et al., 2010) found that neither group increased in symbolic play. The parent-mediated JASPER group showed an increase in functional play compared with the waitlist control group, which was maintained at 1-yr follow-up. Another study comparing caregiver-mediated JASPER and caregiver education interventions found that neither group showed an increase in functional play, but the caregiver-mediated group showed increases in symbolic play types (Kasari et al., 2014). Finally, Kasari et al. (2015) found that the JASPER parent-mediated intervention group showed an increase in types of functional play and highest play level achieved, compared with a caregiver education group, and that gains were not maintained at 1-yr follow-up.
Adaptive Functioning
Two studies (Levels I and III) provide moderate evidence for improvements in outcomes related to attributes of adaptive functioning for children with ASD (e.g., daily living skills, overall adaptability, functional communication, and independent functioning). Comparing an individual parent-mediated intervention with a group SCERTS intervention, Wetherby et al. (2014) found considerable improvements in daily living skills and overall adaptive behavior. Zlomke et al. (2017) used a behaviorally based play therapy intervention and did not find considerable changes in adaptive behavior. However, caregivers reported increases in prosocial adaptive behaviors such as social skills and functional communication.
Autism Spectrum Disorder Symptoms: Behaviors, Socialization, Sensory Processing, and Self-Regulation
Moderate evidence provided by 3 Level I studies (RCTs) indicates that parent-mediated interventions may improve ASD symptoms, although 1 study showed worsening repetitive behaviors. By comparing the PLAY Project Home Consultation model with community services, Solomon et al. (2014) found that children in the intervention group were more than twice as likely to experience improvement in autism diagnostic classification, as measured by the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000). Parents in both groups reported fewer ASD symptoms over time, with no notable differences between groups. Comparing an individual parent-mediated intervention with a group SCERTS intervention, Wetherby et al. (2014) found that social affect improved, as measured by the ADOS. However, Wetherby et al. reported that restricted and repetitive behaviors worsened in both groups. In 1 study, Silva et al. (2011) used parent-implemented Qigong massage, which resulted in improved ASD behaviors, as measured by the Autism Behavior Checklist (Krug et al., 1993), and decreased autism composite scores on the Pervasive Developmental Disorders Behavior Inventory (Cohen & Sudhalter, 2005), compared with the waitlist control group.
Five Level I studies (RCTs) addressed social communication skills, with 3 finding improvement over comparison groups; therefore, moderate evidence exists for the use of parent-mediated interventions to address these skills. Three studies found that the group receiving parent-mediated interventions showed considerable improvements in measures of socialization, social and language abilities, and social–emotional functioning compared with the comparison group (Ingersoll et al., 2016; Silva et al., 2011; Solomon et al., 2014). Gains were maintained at 3-mo follow-up for one group (Ingersoll et al., 2016). An RCT assessing a SCERTS intervention found that the parent-mediated group’s socialization scores remained stable over the intervention period, whereas the comparison group’s scores significantly decreased (Wetherby et al., 2014). The parent-mediated group also had greater improvements on the social composite of the Communication and Symbolic Behavior Scales (Wetherby & Prizant, 2002) compared with group who received the comparison intervention (Wetherby et al., 2014). An RCT assessing the home TEACCH program found that both the intervention and waitlist control participants improved on the Social Interaction domain of the SIB–R, with no notable differences between groups (Welterlin et al., 2012).
Insufficient evidence from 1 Level I study (RCT) showed improvements in sensory symptoms and self-regulation after a parent-mediated intervention (Silva et al., 2011). After a Qigong home intervention program, children showed improved scores on sensory and approach–withdrawal compared with the control group (Silva et al., 2011). Children in the intervention group also improved on sensory and self-regulation impairment.
Discussion
In this systematic review, we identified communication, behavior, play, adaptive functioning, and autism symptoms as outcomes that may be positively influenced by parent-mediated interventions. Despite relatively strong levels of evidence, outcomes were difficult to compare because of variability in measurements and types of interventions. Six studies used follow-up measures, and 5 studies determined that improvements remained, suggesting parent-mediated interventions can have lasting effects.
All studies included children with ASD who were younger than 8 yr old, with no studies exploring the impact of parent-mediated interventions for older children or adolescents. Parents can play an important role in facilitating occupational performance in older children with ASD in the home environment, particularly related to activities of daily living. Resources and evidence-based interventions are lacking to support people with ASD as they age (Gerhardt & Lainer, 2011). In addition, independence in daily living skills continues to be a barrier for children with ASD as they age into adulthood, and parent-mediated interventions could improve occupational performance for these older children (Smith, Maenner, & Seltzer, 2012).
Parent-mediated interventions have been well-established as effective interventions for improving autism symptoms and social communication outcomes in children with ASD (Oono et al., 2013). Our review supports this finding, with multiple well-designed RCTs providing strong evidence for positive outcomes related to communication and autism symptoms. However, other functional outcomes, such as behavior, play, and adaptive functioning, have emerging evidence supporting gains for children with ASD after parent-mediated interventions; this finding is a new, considerable contribution to the literature.
Although the evidence levels of the studies supporting these findings are high, generalizability is limited because of the small number of studies assessing these areas of occupational performance. For example, all studies addressing play outcomes were conducted by the same research group, and outcome measurement occasionally did not occur in the child’s natural environment or with an interventionist versus parent or peer. In addition, key features and difficulties of ASD, such as feeding, self-care skills, sleep, and sensory sensitivities, were not a focus of any of the parent-mediated interventions. It is essential to assess a variety of outcomes (e.g., play, feeding) in the natural context of family daily routines to better determine long-term effectiveness of these interventions.
Occupational roles of children include feeding, independence in self-care, school and social participation, play, and sleep (AOTA, 2014). Many outcomes in this review, although not always overtly occupational in nature, relate to basic skills, which are the building blocks for occupational roles and influence successful occupational engagement. For example, a decrease in autism symptom severity, coupled with improvements in communication skills, may enable a child to form relationships with peers and participate throughout the school day. Parent-mediated interventions can address these essential skills and enable age-appropriate participation in the child’s environment.
Emerging studies from the occupational therapy literature and other research groups support parent-led intervention methods that did not meet the definition of parent-mediated used for this review or that focused on children with diagnoses other than ASD (e.g., Baranek et al., 2015; Dunn et al., 2012). Some of these studies have found improvements in occupational performance areas such as feeding (Johnson et al., 2015), sleep (Johnson et al., 2013), and transitioning to adulthood (Smith, Greenberg, & Mailick, 2012). Future research should begin to compare traditional parent-mediated interventions with alternative interventions that include caregivers to identify the most efficient and effective intervention for families.
Although this review focused on child outcomes, multiple studies also explored the impact of these interventions on parent outcomes. Several studies found that parents in the intervention groups experienced decreased stress (Ingersoll et al., 2016; Silva et al., 2011; Solomon et al., 2014; Welterlin et al., 2012). This finding is particularly meaningful because parents of children with ASD may have high parental stress and lower parental self-efficacy and well-being (Karst & Van Hecke, 2012). Another study found improved parent self-efficacy and positive perception of their children (Ingersoll et al., 2016). Improving a caregiver’s state of well-being and decreasing stress may lead to better overall family functioning and outcomes for children. Parent-mediated interventions have potential benefits for the child, parent, and family.
As the need for intervention in rural communities has expanded and access to technology has increased, a growing number of health services are being provided over the Internet through telehealth models (Baggett et al., 2010). Ingersoll et al. (2016) described a successful parent-mediated intervention delivered via a telehealth model. Several other studies have provided further emerging evidence for parent-mediated interventions via telehealth, although they did not meet criteria based on level of evidence for this review (e.g., Baharav & Reiser, 2010; Meadan et al., 2014). Both of these studies used Skype and found improvements in children’s communication skills. This emerging delivery model may increase access to services, decrease barriers to care, and allow occupational therapy practitioners to serve more families through parent-mediated interventions.
Limitations and Future Directions
Although many of the studies were deemed to have high levels of evidence and relatively strong design, limitations exist that should be considered when interpreting results. Although certain types of bias such as blinding of participants or interventionists are challenging, future studies, particularly RCTs, should consider aspects of the study design such as randomization and including objective outcomes to reduce study bias. In addition, because of the variety in methods, outcome measures, and study lengths and locations, it is challenging to draw conclusions regarding the most effective type of parent-mediated intervention, location, or length. Many studies compared parent-mediated interventions with parent education interventions, finding similar improvements in outcomes. More research is needed to determine what characteristics of parent-mediated interventions are essential to address specific outcomes and to achieve sustained gains for children with ASD and their families. Finally, future research should also explore evidence for parent-mediated interventions for older children and adolescents as well as a broader range of outcomes across all age groups.
Implications for Occupational Therapy Practice
Because of the high prevalence of ASD among children, parent-mediated interventions may serve as an evidence-based, family-centered approach to address needs in an environmentally valid context. Occupational therapy practitioners are particularly well suited to support this type of intervention because of their focus on occupational performance across the lifespan. The evidence discussed in this review has the following implications for occupational therapy practice:
On the basis of the moderate to strong evidence for parent-mediated interventions for areas of communication, ASD symptoms, behavior, play, and adaptive functioning, occupational therapy practitioners should consider implementing traditional parent-mediated interventions to support families with children with ASD.
Occupational therapy practitioners can effectively collaborate with parents to implement intervention strategies that can be provided more frequently and intensively in a natural environment through daily routines.
Occupational therapy practitioners can guide parents to facilitate child skill development while adapting interventions to the child’s changing needs to improve occupational performance.
Although discrete skills or behaviors are often the focus of parent-mediated interventions, occupational therapy practitioners are well suited to expand those improvements into occupational participation and improve engagement in daily activities for children with ASD.
Conclusion
Parent-mediated interventions are effective in improving many outcomes for children with ASD. Our findings align with existing research showing considerable improvements in communication and autism symptoms. This review also identified limited but growing evidence supporting several emerging areas of focus for parent-mediated interventions (adaptive functioning, play, and behavior). Occupational therapy practitioners can use the evidence synthesized in this review to effectively collaborate with parents while expanding on traditional occupational therapy approaches to best support children with ASD in improved occupational performance.
Supplemental Material
Supplementary material for Parent-Mediated Interventions for Children With Autism Spectrum Disorder: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.030015.pdf for Parent-Mediated Interventions for Children With Autism Spectrum Disorder: A Systematic Review by Colleen E. Althoff, Caitlin P. Dammann, Sarah J. Hope and Karla K. Ausderau in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.