
Abstract
The chronic, progressive, and unpredictable nature of multiple sclerosis (MS) affects all areas of life, from activities of daily living and social activities to leisure and work (Karhula et al., 2013; Lexell et al., 2014). MS causes various impairments at the body function level, such as fatigue, bladder dysfunction, and sensory and motor symptoms (Holper et al., 2010). In everyday life, these impairments have both a physical impact, such as problems using different means of transport, and a psychological impact, such as worries related to the disease (Johansson et al., 2007). Although assessment of the severity of MS is based mainly on physical impairments (Lublin et al., 2014), perceived quality of life is affected more by other factors such as level of social support, living area, depression, level of education, employment, fatigue, and religiosity (Yamout et al., 2013).
Cognitive retraining and cognitive–behavioral therapy for emotional regulation and physical exercise are examples of interventions that have shown positive effects at the body function level (Yu & Mathiowetz, 2014b). There is also evidence that people with MS benefit from individualized, goal-directed, occupational therapy–related interventions that target functional performance and aim to promote participation in everyday life (Yu & Mathiowetz, 2014a).
In choosing the occupational therapy approach that best promotes participation in everyday life, occupational therapists first need to better understand the factors that predict participation in people with MS. With this information, interventions can be targeted and planned to enable people with MS to take up occupations they currently perceive as challenging. In addition, better understanding of the factors promoting participation can assist occupational therapists in choosing measures that support clinical practice. The purpose of this study was to contribute to knowledge on the factors that support participation in everyday life for people with MS.
Definitions
Definitions of participation differ, as do the measures of participation based on them (Eyssen et al., 2011). In this article, we define participation in terms of autonomy. Thus, participation is actualized when a person is able to control his or her life, even when the ability to perform the actions in question is lacking (Perenboom & Chorus, 2003). In chronic and progressive conditions such as MS, it is essential to evaluate participation in relation to autonomy. The Impact on Participation and Autonomy (IPA) measure was developed in line with this assumption and is recommended to be used in conjunction with other measures when evaluating both the need for and the outcome of rehabilitation (Cardol et al., 1999).
Thus far, studies focusing on the predictors of participation and autonomy in people with MS have been few. One such study found a relationship between appraisal, defined as the evaluation of a situation and the ability to deal with the situation, and participation and autonomy (van den Akker et al., 2016). Another study, conducted with a small sample of people with MS, reported that disease severity measured by the Expanded Disability Status Scale (EDSS) and generic quality of life measured by the EuroQol–5D visual analog scale correlated with participation and autonomy (Kwiatkowski et al., 2014).
Because MS affects many life areas, it is important to know how participation and autonomy are associated with the perceived impact of the disease on everyday life. For example, a previous study showed that disease severity and generic quality of life may affect participation (Kwiatkowski et al., 2014). This is an important topic that merits further study. Moreover, it is not known whether participation and autonomy are influenced by gender. Therefore, the aim of our study was to investigate how perceived quality of life and impact of the disease on the individual, the severity of the disease, and gender predict participation and autonomy in people with MS. We hypothesized that participation and autonomy would be predicted by perceived quality of life, the physical and psychological impacts of the disease, the severity of the disease, and gender.
Method
Study Design and Procedure
A cross-sectional survey design with convenience sampling was used. Data were collected in two phases from people with MS during their rehabilitation period. The first data set was collected as part of a larger evaluation study conducted in 2011. The data were gathered from people with MS who participated in a 2-yr multiprofessional group-based outpatient rehabilitation project implemented by the Finnish Neuro Society and evaluated by the Social Insurance Institution of Finland and the GeroCenter Foundation for Aging Research and Development. Rehabilitation professionals from the Finnish Neuro Society recruited participants from three areas of Finland: Helsinki, Kuopio, and Turku (Salminen et al., 2014). To obtain a larger sample, the second data set was collected in 2012–2013 during an inpatient rehabilitation period of 1–3 wk at Masku Neurological Rehabilitation Center.
All potential participants were informed about the study by rehabilitation professionals. Those who agreed to participate provided written informed consent and completed questionnaires. The study was approved by the ethics committees of the Social Insurance Institution of Finland (Data Set 1) and the Hospital District of Southwest Finland (Data Set 2).
Participants
People with MS were recruited with predefined inclusion and exclusion criteria. The inclusion criteria were age 18–65 yr, confirmed diagnosis of MS, and ability to complete questionnaires independently or with the help of an assistant. A total of 194 people with MS participated in the study (Karhula et al., 2017). Most participants were women (72%), and mean (M) participant age was 50 yr (standard deviation [SD] = 9). Participants had high disease severity ratings on the EDSS (M = 5.8, SD = 2) and a median disease duration of 14 yr. Most (83%) were on a disability pension, and one-third (33%) lived alone.
Measures
Participation and Autonomy.
The IPA (Cardol et al., 1999) comprises 32 items in five domains: (1) Autonomy Indoors, (2) Family Role, (3) Autonomy Outdoors, (4) Social Relationships, and (5) Work and Education. A standardized mean score is calculated for each domain. Higher scores indicate lower perceived participation and autonomy. The Finnish version of the IPA (Kanelisto & Salminen, 2011) has proved to be a valid and reliable measure (Karhula et al., 2017).
Quality of Life.
The World Health Organization Quality of Life–Brief measure (WHOQOL–BREF; WHOQOL Group, 1998) comprises 26 items that assess the following domains: Physical Health, Psychological, Social Relationships, and Environment. Domain scores are calculated by multiplying the mean of all items in each domain by 4 and converting raw scores to transformed scores; each domain score ranges from 4 to 20. Higher scores indicate better perceived quality of life. The psychometric properties, including validity and reliability, have been reported to range from good to excellent (Skevington et al., 2004).
Physical and Psychological Impact of Multiple Sclerosis.
The Multiple Sclerosis Impact Scale (MSIS–29; Hobart et al., 2001) consists of two subscales: Physical (20 items) and Psychological (9 items). The sum scores of the Physical and Psychological subscales can be transformed into percentages. Higher scores indicate that the disease has a higher perceived impact on daily life. The validity and reliability of the domains have been reported to be good (Hobart et al., 2001).
Disease Severity.
The severity of MS was evaluated by a neurologist using the EDSS (Kurtzke, 1983). The EDSS score ranges from 0 (no impairment) to 10 (death) in 0.5-point increments.
Statistical Analysis
Descriptive statistics were calculated using IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY). Mutual relationships between variables were estimated with the statistical modeling program Mplus Version 6.12 (Muthén & Muthén, 2010). The IPA Work and Education domain (6 items) was excluded from the analysis because the items were applicable to only 51 participants.
Structural equation modeling (SEM) was considered an appropriate method for testing a model in which several factors were hypothesized to be predictors of participation and autonomy. SEM is premised on two statistical assumptions, independence of observations and multiple normally distributed data. The first assumption was met, but some correction was needed to satisfy the second assumption. Owing to the non-normal distribution of the data (tested with the Kolmogorov–Smirnov test), both the correlation analysis and SEM were estimated using the full information maximum likelihood method with scale-corrected χ2 test values and robust standard errors (MLR estimate in Mplus). The few missing values (0%–3.6%) in the data were considered to be missing at random. The first step of the analysis was estimation of the factor model, which, in the second step, was modified with the help of standardized residuals and modification indexes. If model fit is poor, the modification indexes show how two variables or factors should be associated with each other, whereas the standardized residuals provide information about structure in cases of multiple variables.
The fit of the models was tested using χ2 and several goodness-of-fit indexes. A statistically nonsignificant (p > .05) χ2 value means that the covariance structure based on the model does not significantly differ from the covariance structure of the data. When the model fit is acceptable, the goodness-of-fit values should be as follows: standardized root mean square residual (SRMR) value below .08, root mean square error of approximation (RMSEA) value below .06, and comparative fit index (CFI) and Tucker–Lewis index (TLI) values of .95 or greater (Hu & Bentler, 1999). In addition, normalized residuals are expected to distribute normally, and absolute values above 2 should not account for more than 5% of all values.
Results
The correlation analysis showed significant associations of all the IPA domains (dependent variables) with all the WHOQOL–BREF domains and the MSIS–29 (independent variables; Table 1). Consequently, a structural equation model (Model 1) based on two latent factors was constructed. The reliability of the IPA domains and MSIS–29 was high (range = .85–.93) in this sample, enabling the creation of latent factors. The WHOQOL–BREF data contained only the domain scores. However, previous studies (Skevington et al., 2004) have shown that the WHOQOL–BREF has acceptable reliability. The IPA domains yielded one latent factor, labeled “participation and autonomy,” and the domains of the WHOQOL–BREF and the MSIS–29 formed a single shared latent factor. Although the EDSS correlated significantly only with the IPA domain Autonomy Indoors, the WHOQOL–BREF Physical Health domain, and the MSIS–29 Physical domain, the EDSS was added to the model as an independent variable. Gender was not significantly associated with any variable. Therefore, gender was omitted from this phase of the analysis.
Correlation Matrix of Predictor and Dependent Variables (N = 194)
Note. EDSS = Expanded Disability Status Scale; IPA = Impact on Participation and Autonomy; MSIS–29 = Multiple Sclerosis Impact Scale; WHOQOL–BREF = World Health Organization Quality of Life–Brief measure.
p < .01.
The model showed poor fit to the data, χ2(43, N = 194) = 234.772, p < .001, CFI = .806, TLI = .752, RMSEA = .152, SRMR = .095 (Figure 1). Therefore, Model 1 was modified. According to the standardized residuals, four specific factors (S1, S2, S3, and S4) were added to the model. Moreover, in Model 1, the EDSS did not significantly predict the latent factor “participation and autonomy.” However, the Mplus modification indexes indicated that the EDSS predicted the IPA domain Autonomy Indoors.
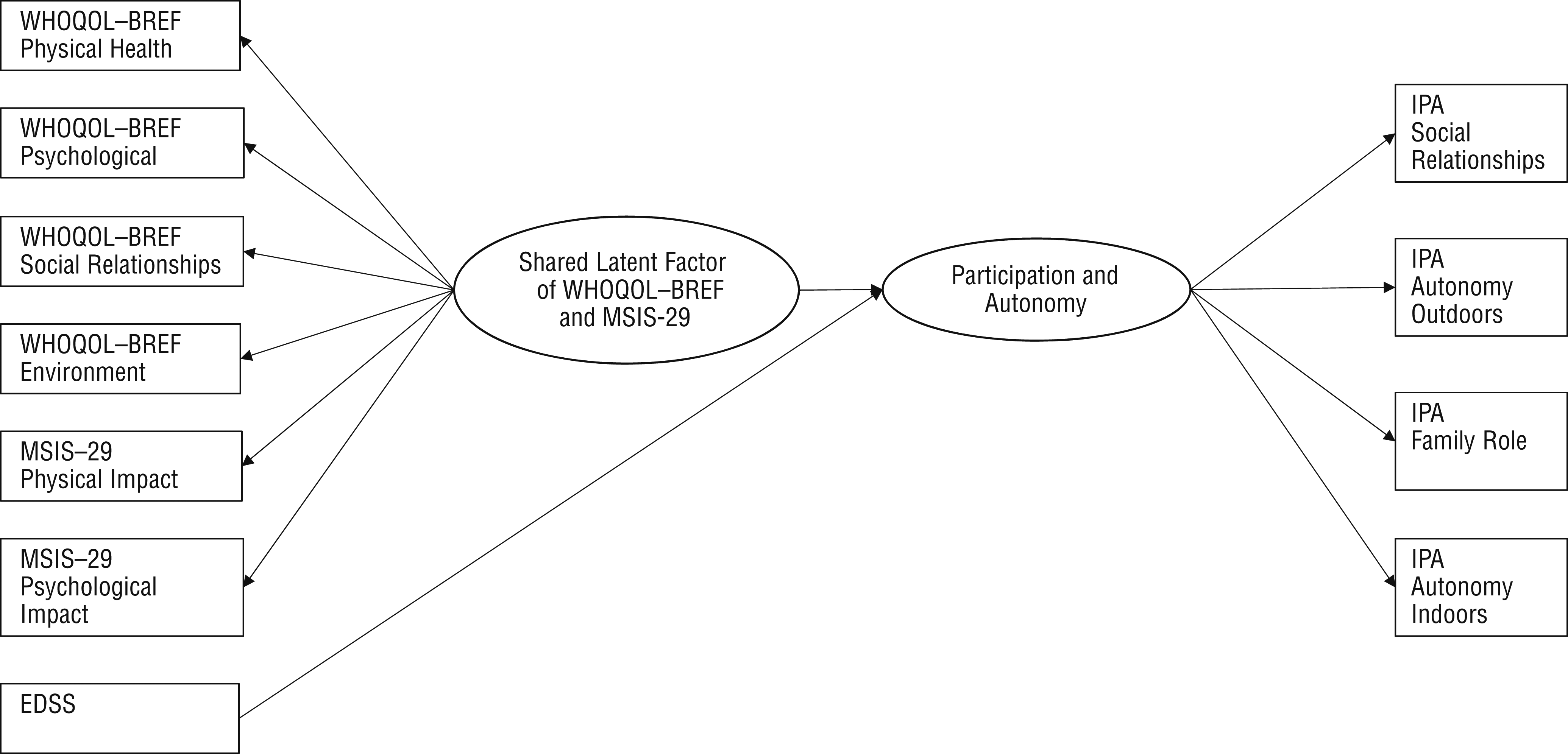
Hypothesized prediction of participation and autonomy by WHOQOL–BREF and MSIS–29 domains and EDSS scores
The final structural equation model (Model 2) showed good fit to the data (Figure 2). All the goodness-of-fit indexes except the χ2 value supported the model, χ2(30, N = 194) = 46.729, p < .026, CFI = .983, TLI = .969, RMSEA = .054, SRMR = .039. Moreover, the normalized residuals were distributed as expected.
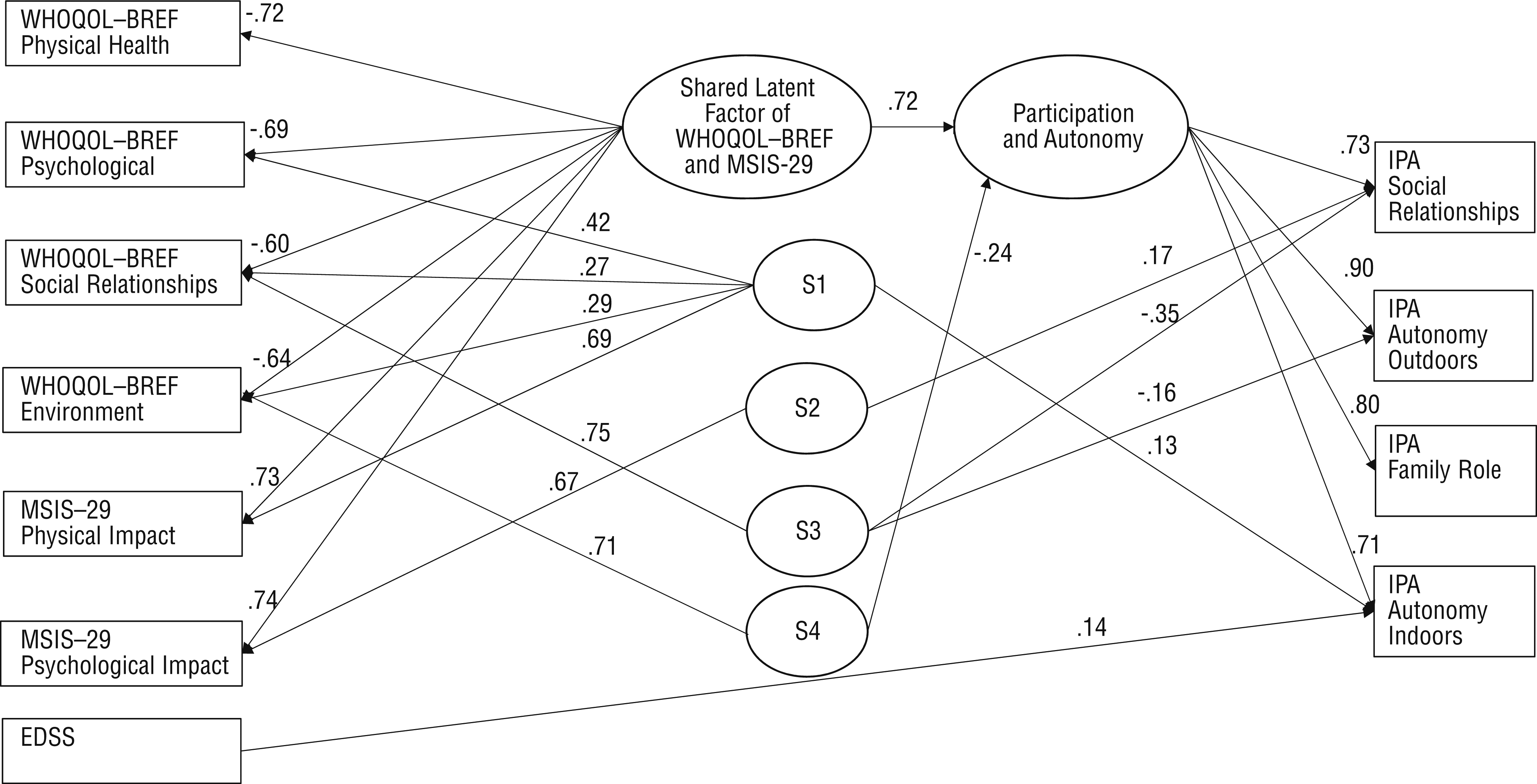
Prediction of participation and autonomy by WHOQOL–BREF and MSIS–29 domains and EDSS scores
Collectively, the WHOQOL–BREF Physical Health, Psychological, Social Relationships, and Environment domains and the MSIS–29 Physical and Psychological domains predicted participation and autonomy as expressed in the Social Relationships, Autonomy Outdoors, Role Performance, and Autonomy Indoors domains of the IPA. The shared latent factor of the WHOQOL–BREF and MSIS–29 predicted the latent factor “participation and autonomy” with an explanation rate of 51.7%. Moreover, Factor S4, comprising the WHOQOL–BREF Environment domain, predicted “participation and autonomy” with an explanation rate of 5.5%. In addition, three specific factors predicted different domains of the IPA. The EDSS predicted only the IPA domain Autonomy Indoors. The whole model accounted for 57.2% of the variance in the latent factor “participation and autonomy.”
Discussion
The current study supports the hypothesis that perceived quality of life and the physical and psychological impact of MS predict perceived participation and autonomy. The IPA domains as a whole were predicted by all of the WHOQOL–BREF and MSIS–29 domains together. However, the results did not confirm the hypothesis that disease severity and gender also predict participation and autonomy. Disease severity predicted participation and autonomy only in indoor activities, and gender did not predict participation and autonomy at all.
One explanation for the strong association of participation and autonomy with the perceived impact of the disease and quality of life is that although these concepts describe different phenomena, they all are patient reported. Individuals’ different internal standards, values, or conceptualization of the measured concept—in other words, response shift—may also influence their evaluations (Schwartz et al., 2007). In clinical practice, it is important to remember that these measures (IPA, WHOQOL–BREF, and MSIS–29) are closely related to each other. People with MS may experience participation in many different measures as demanding or time consuming, and in such cases it is worth selecting the measure that best suits a specific situation. In occupational therapy practice, the IPA merits consideration because it focuses on everyday activities rather than on underlying elements such as muscle stiffness, problems of concentration, or feelings of depression. In this way, the IPA can help people with MS identify limitations in their participation and autonomy and can help occupational therapy practitioners implement occupation-based and client-centered practice.
The present results underline the importance of environmental factors. The Environment domain of the WHOQOL–BREF predicted participation and autonomy. This finding is in line with a previous finding of an association between environmental barriers and perceived participation of people with a chronic condition (Larsson Lund & Lexell, 2009). The finding points to the benefits of holistic models of occupational therapy, such as the Person–Environment–Occupation Model (Law et al., 1996), that emphasize the role of the environment. If clients with MS perceive limitations in participation and autonomy, we recommend that occupational therapists assess the relevant environmental factors and suggest actions to decrease environmental barriers, such as modifying the environment or educating family members and others close to clients.
The results also show that disease severity measured with the EDSS predicted only the IPA domain Autonomy Indoors. A possible explanation for this association is that autonomy indoors—for example, when washing and dressing or toileting—is more dependent on physical than psychological effort. Although the EDSS is widely used to assess disease severity, it is much more closely linked to physical than psychological or cognitive abilities and problems (Cohen et al., 2012). Even if the EDSS score is associated with the physical impact of MS at every level of severity, the psychological impact of MS does not increase along with disease severity (Gray et al., 2009). This would explain why disease severity predicted participation and autonomy only indoors, and not its more social-based dimensions such as family or social relationships.
This study has several limitations. First, the sample included only people with moderate to severe disability as measured by the EDSS. Second, most participants received a disability pension, and consequently the IPA Work and Education domain could not be applied in the SEM. Third, although the results identified specific predictors of participation and autonomy, the causality of these associations remains unknown. To determine causality would require an appropriate study design, such as a before-and-after design.
The results indicate a need for further research. The role of different kinds of environmental factors—physical, psychological, economic, societal, and social—in the participation and autonomy of people with MS needs to be understood in greater detail. We need a better understanding of the kinds of environmental intervention that might improve the participation and autonomy of people with MS despite the degenerative nature of the disease.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice with people with MS:
Experiences of all the dimensions of participation and autonomy were closely associated with perceived quality of life and impact of the disease; hence, it would be useful to assess participation and autonomy and plan interventions using this information. The IPA appears to be an appropriate measure for these purposes.
Disease severity alone should not guide the occupational therapy process. Although it may influence perceived participation and autonomy in indoor activities, the associations between the other dimensions of participation and autonomy and disease severity were weak.
The environmental factors affecting perceived participation and autonomy should be considered when planning interventions to promote participation and autonomy.
Footnotes
Acknowledgments
We thank all people with MS who participated in this study. Special thanks go to Katja Kanelisto, MSc, for participating in the translation process of the Finnish version of the Impact on Participation and Autonomy instrument. We thank also the Finnish Cultural Foundation’s South Savo Regional Fund for supporting this study by a grant. This study is registered in the ISRCTN registry (ISRCTN72556817).